Association of non-alcoholic fatty liver disease and COVID-19: A literature review of current evidence
2021-09-03 02:44:10PrajnaAnirvanShivaramSinghAlexaGiammarinoSanjayaSatapathy
World Journal of Hepatology 2021年8期
Prajna Anirvan, Shivaram P Singh, Alexa Giammarino, Sanjaya K Satapathy
Prajna Anirvan, Shivaram P Singh, Department of Gastroenterology, Sriram Chandra Bhanj Medical College and Hospital, Cuttack 753007, Odisha, India
Alexa Giammarino, Department of Internal Medicine, Donald and Barbara Zucker School of Medicine at Hofstra, Manhasset, NY 11030, United States
Sanjaya K Satapathy, Division of Hepatology at Sandra Atlas Bass Center for Liver Diseases and Transplantation, Donald and Barbara Zucker School of Medicine at Hofstra, Manhasset, NY 11030, United States
Abstract The coronavirus disease 2019 (COVID-19) pandemic has swept through nations, crippled economies and caused millions of deaths worldwide.Many people diagnosed with COVID-19 infections are often found to develop liver injury, which, in a small portion of patients, progresses to severe liver disease.Liver injury in the form of elevated transaminases, hyperbilirubinemia and alterations in serum albumin has been observed to be higher in patients with severe forms of the disease.Those who already have insult to the liver from chronic disease, such as nonalcoholic fatty liver disease (NAFLD) may be at the greatest disadvantage.The severity of COVID-19 also seems to be driven by the presence of NAFLD and other co-morbidities.About 25% of the global population has NAFLD.With such a widespread prevalence of NAFLD, understanding the disease progression of COVID-19 and the occurrence of liver injury in this vulnerable population assumes great significance.In this review, we present an overview of COVID-19 infection in patients with NAFLD.
Key Words: SARS-CoV-2; Fatty liver; Mitochondria; Nitrosative stress; Oxidative stress; COVID-19; Metabolic associated fatty liver disease; Nonalcoholic fatty liver disease; Progressive liver disease; Nonalcoholic steatohepatitis
INTRODUCTION
The worldwide figures of coronavirus disease 2019 (COVID-19) presently stand at 154640649 confirmed cases with 3232285 deaths[1].Although primarily a respiratory syndrome, COVID-19 has been reported to cause liver injury in multiple studies, including metanalyses[2-4].The incidence of liver injury as assessed by several indicators like transaminases, bilirubin and albumin has been found to be higher in patients with severe COVID-19 infection[3,5].Increasing severity of liver chemistry abnormalities on hospital admission predicts early in-hospital mortality in COVID-19 patients[4].
There is a high global burden of pre-existing liver disease[6], including chronic viral hepatitis, nonalcoholic fatty liver disease (NAFLD) and alcohol-associated liver disease (ALD).For example, in China, where the pandemic originated, liver cirrhosis affects around 7 million people[7].Similarly, in the United States which has the highest number of recorded COVID 19 cases, about 4.5 million of adults are diagnosed with chronic liver disease[8].In a cross-sectional analysis based on data from National Health and Nutrition Examination Surveys (NHANES), it was observed that the prevalence of NAFLD (by US-Fatty Liver Index) spiked from 20.0% (1988-1994) to 28.3% (1999-2004) to 33.2% (2009-2012) and 31.9% (2013-2016)[9].This increasing trend is in concurrence with increases in obesity, diabetes mellitus, hypertension and insulin resistance[9].It is also to be noted that many patients with fatty liver disease remain undiagnosed and are incidentally detected.Therefore, the actual prevalence of NAFLD may be much higher.In such a background of widespread prevalence of chronic liver disease especially NAFLD, the incidence of liver injury in COVID-19 and its impact on disease progression assumes greater significance.In a recent study, we found that mortality associated with the known risk factors of COVID19 (hypertension, diabetes, male sex, and old age) was accentuated in the presence of liver chemistry abnormalities in those diagnosed with COVID-19[4].
PATHOGENESIS AND PATTERN OF LIVER INJURY IN COVID-19
The pathogenesis of liver injury in COVID-19 is multifactorial.A number of factors have been identified for perpetuating and potentiating liver injury in COVID-19.Direct viral-mediated hepatocyte injury, liver injury ensuing from cytokine release syndrome, drug-induced liver injury and ischemic hepatitis are just some of the mechanisms responsible for hepatic dysfunction in COVID-19[10].The pattern of liver injury in COVID-19, as evidence from multiple studies, is a rise in liver enzymes [primarily aspartate aminotransferase and alanine aminotransferase (ALT)] with mild increases in bilirubin[10].In a study by Caiet al[11] from China, among 417 patients, 20.75% had hepatocellular pattern of liver injury, 29.25% had a cholestatic pattern, while 43.4% had a mixed type of liver injury.Liver injury is transient in most cases and liver enzymes usually return to normal with recovery from COVID-19[2].The rampant use of multiple medications-antibiotics, antivirals, nonsteroidal anti-inflammatory drugs, herbal medications, interferon and other immunomodulators has been associated with increased liver test abnormalities[11].To add to this is the presence of pre-existing liver disease in patients with COVID-19 which makes the pathogenesis of hepatic dysfunction even more complex.In the largest reported cohort of 745 chronic liver disease and cirrhotic patients with COVID-19, it was observed that baseline liver disease stage and ALD were independent risk factors for death from COVID-19[12].The APASL COVID19 Liver Injury Spectrum (APCOLIS) Study has shown that preexisting liver disease is associated with poor outcome in patients with SARS CoV2 infection.Additionally, if these patients also have chronic liver disease, diabetes and/or obesity, they are more vulnerable and should be closely monitored[13].In a study on 12 COVID-19 patients with pulmonary embolism on autopsy, hepatic steatosis involving 50-60 percent of hepatocytes was found in all patients.This data supports the fact that pre-existing liver diseases like ALD and NAFLD could play significant roles in COVID-19 progression[14].
COVID-19 IN THE SETTING OF NAFLD
Whether NAFLD is an independent or dependent determinant for worse outcomes in COVID-19 has been a hot topic of debate in recent times.A look at the figures and the results of several studies done in the midst of this pandemic opens up conflicting and debatable viewpoints in this regard.Interestingly, in this above-mentioned cohort of 745 patients, 43% of patients had NAFLD, while hypertension, diabetes and obesity — established risk factors for developing severe COVID-19 — constituted the major comorbidities[12].While one can argue that it is ALD and not NAFLD which has been observed to be a significant predictor of mortality in COVID-19, it would be worthwhile to take note of the fact that patients with ALD had more severe underlying liver disease compared to those with NAFLD.In a retrospective study on 202 patients with confirmed COVID-19, it was observed that patients with NAFLD had a higher risk of disease progression, greater likelihood of abnormal liver function from admission to discharge and longer viral shedding time[15].An association between the presence of metabolic associated fatty liver disease (MAFLD) and COVID-19 severity was observed in younger patients[16].In another study on 589 patients from the eastern Mediterranean region, NAFLD has been found to be a predictor of liver injury in COVID-19.However, quite contrary to the results of other studies, NAFLD did not seem to be an independent predictor of mortality, disease severity, or markers of disease progression[17].Similarly, in another study by Huanget al[18], although more patients with NAFLD developed abnormal liver function tests, concurrent NAFLD was not found to be associated with adverse clinical outcomes in patients with COVID-19.Table 1 shows a summary of the various studies describing the association between NAFLD and COVID-19.
MECHANISM OF COVID-19 PROGRESSION IN PATIENTS WITH NAFLD
The role of inflammation in the pathophysiology of NAFLD has been well recognized[19].It has been hypothesized that hepatic inflammation resulting from pro-inflammatory cytokines released by adipose tissue is even furthered by COVID-19[15].The liver is a major site of lipid metabolism and the generation of lipid species plays an important role in regulating metabolic inflammation.The complex pathways in lipid metabolism drive innate immunity and have been found to affect the progression to steatohepatitis and fibrosis in NAFLD[20].Additionally, NAFLD patients are found to have elevated plasma levels of von Willebrand factor and circulating plasminogen activator inhibitor type 1[21].This has been hypothesized to predispose such patients to higher risks of adverse cardiovascular events.It has also been postulated that hepatic and systemic immune responses due to underlying NAFLD could contribute to the cytokine storm in younger patients with COVID-19[16,22].While severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) binds to angiotensin-converting enzyme 2 (ACE2) receptors and attaches to the cell, cellular entry is made possible by cleavage of the SARS-CoV-2 spike protein by transmembrane serine protease 2 (TMPRSS2)[23].Interestingly, it has been seen that while there were no differences in liver mRNA expression of both ACE2 and TMPRSS2 between subjects without liver injury and patients with only steatosis, upregulation of these genes occurred in obese patients with nonalcoholic steatohepatitis (NASH).Additionally, there was positive correlation of ACE2 and TMPRSS2 with NAFLD activity score and TMPRSS2 positively correlated with weight, body mass index (BMI) and cholesterol[24].However,to complicate matters, in another study by Biquardet al[25], none of the genes necessary for SARS-CoV-2 infection-TMPRSS2 and ACE2 included- were differentially expressed between lean or obese controls and patients with simple steatosis or with NASH.Hence the role of underlying NAFLD on the outcomes of COVID-19 infection is still up for debate.
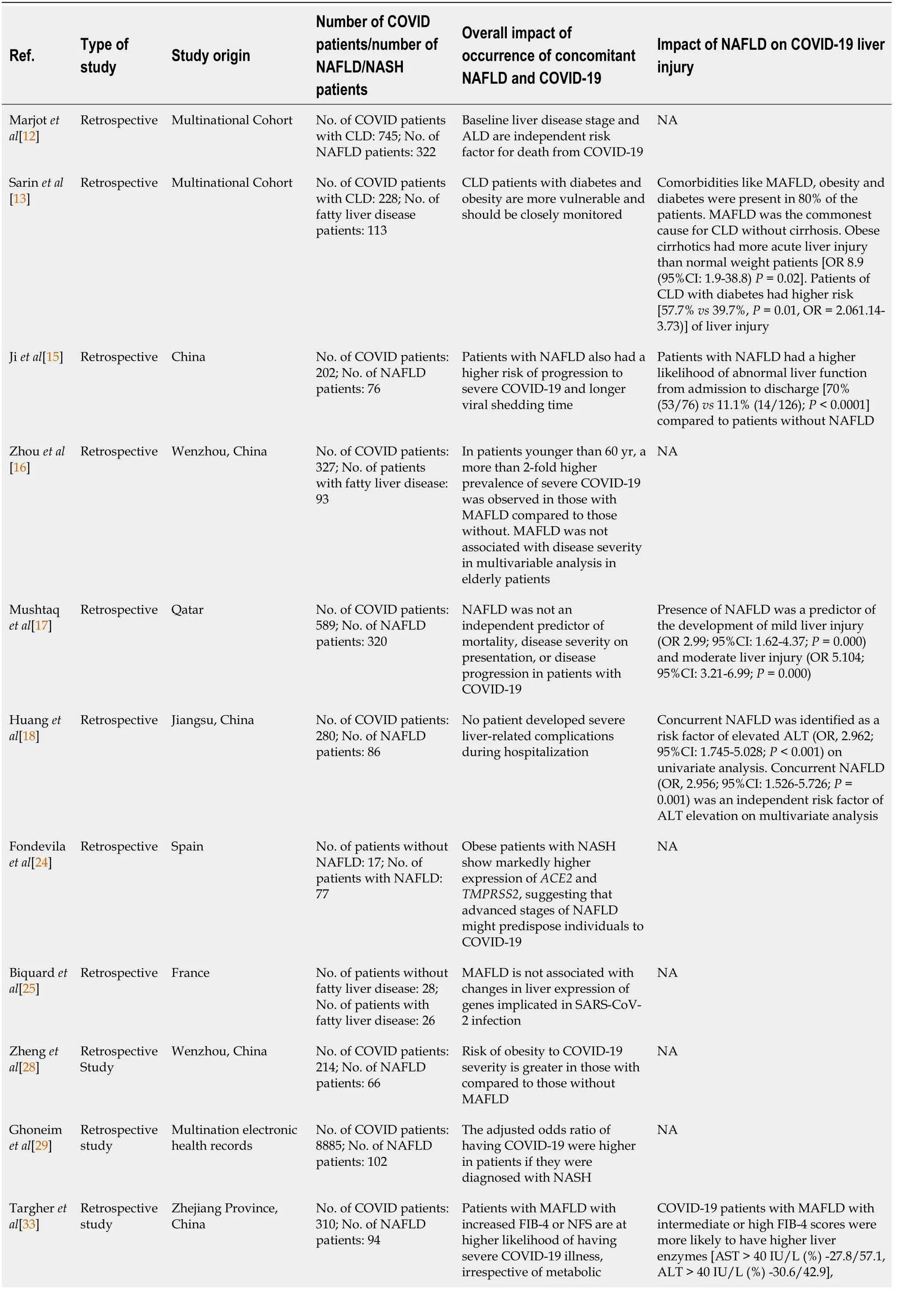
Table 1 Summary of various studies describing the association between nonalcoholic fatty liver disease and coronavirus disease 2019
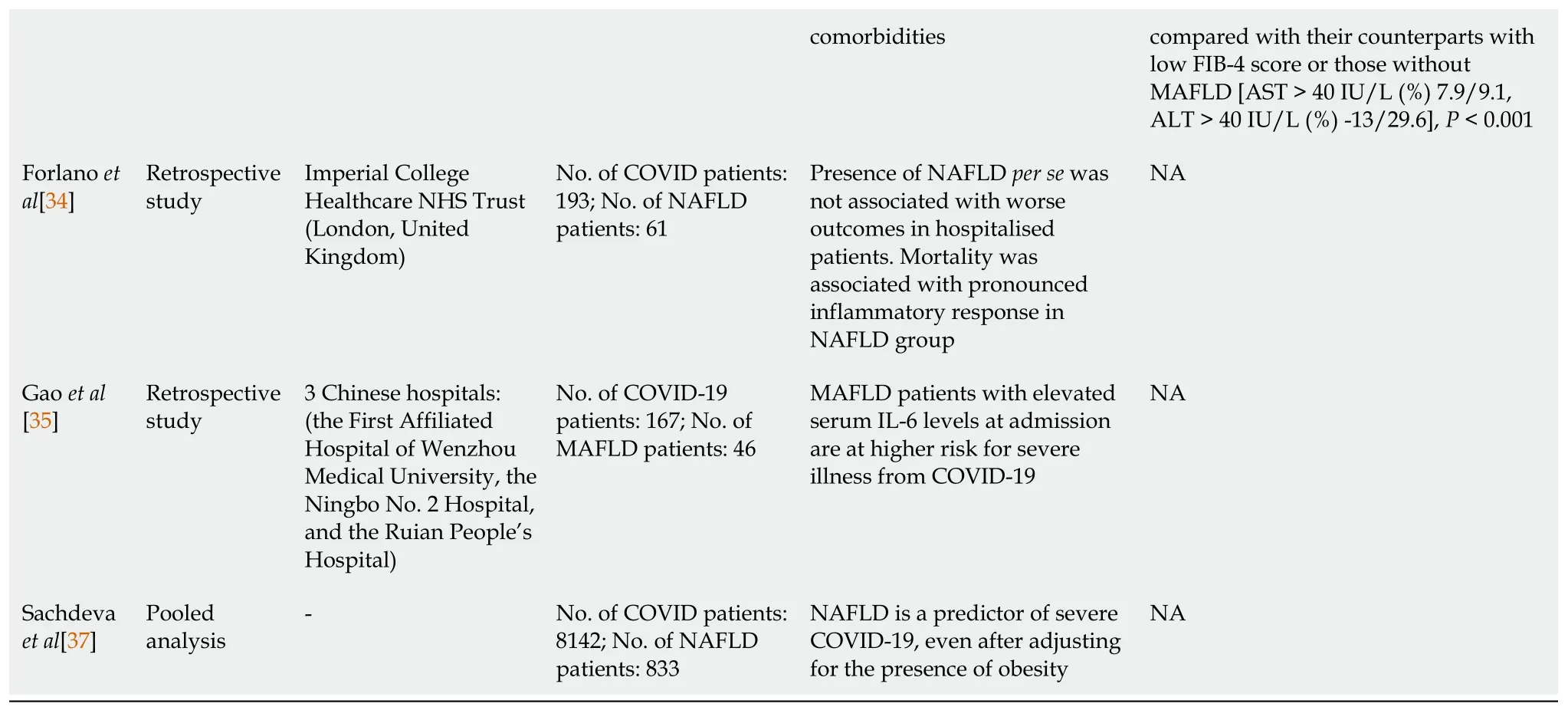
NAFLD: Nonalcoholic fatty liver disease; COVID-19: Coronavirus disease 2019; CLD: Chronic liver disease; ALD: Alcohol-associated liver disease; NA: Not available; MAFLD: Metabolic associated fatty liver disease; CI: Confidence interval; OR: Odds ratio; ALT: Alanine aminotransferase; NASH: Nonalcoholic steatohepatitis; ACE2: Angiotensin-converting enzyme 2; TMPRSS2: Transmembrane serine protease 2; SARS-CoV-2: Severe acute respiratory syndrome coronavirus 2; AST: Aspartate aminotransferase; IL-6: Interleukin-6.
ROLE OF COMORBIDITIES
In such a background of conflicting data, it is worthwhile to analyze the role of comorbidities that are present in patients with NAFLD which might lead to disease progression in COVID-19.It needs no reiteration that NAFLD is usually accompanied by a cluster of several other conditions such as obesity, insulin resistance, dyslipidemia and hypertension, collectively reflecting underlying metabolic syndrome (MS).According to the ATP III criteria, the prevalence of the MS in patients with NAFLD is 22.8%[26].The strong association between MS and NAFLD has led investigators to term NAFLD the hepatic component of MS[27].Thus, it is entirely understandable that the presence of these components would potentially cause increased severity of COVID-19.This has been validated by a multicentric study by Zhenget al[28] which showed that obesity conferred a nearly sixfold higher risk of severe COVID-19 in patients with NAFLD.A strong positive association between the different components of MS and COVID-19 has also been reported in a population-based study[29].Obesity and a state of insulin resistance impairs the ability to mount an effective immune response and predisposes to viral infections and respiratory diseases[30,31].The questions that naturally arise from these observations are: (1) Do the different components of MS drive outcomes in COVID-19 infection and is NAFLD merely a bystander? and (2) Does NAFLD independently drive inflammation and disease progression in COVID-19? The latter is supported by the finding that NAFLD is associated with 30-d all-cause mortality in patients with community-acquired pneumonia with a significant higher degree of association in patients with advanced hepatic fibrosis[32].
IS NAFLD INDEPENDENTLY ASSOCIATED WITH COVID-19 SEVERITY?
In the population-based study by Ghoneimet al[29], among different components of MS, NASH was found to be associated with the highest risk of COVID-19 after calculating the adjusted odds ratio.A study by Targheret al[33] sheds some light on this conundrum.In this study on 310 COVID-19 patients, subjects with MAFLD with increased fibrosis-4 (FIB-4) or NAFLD fibrosis score were more likely to have severe COVID-19 illness, irrespective of metabolic comorbidities like obesity and diabetes.Forlanoet al[34] showed that although NAFLD patients have higher levels of inflammatory markers like CRP compared to the non-NAFLD group, the presence of NAFLDper sewas not associated with adverse outcomes in the whole study population.Additionally, the presence of intermediate/high-risk FIB-4 scores as well as the presence of liver cirrhosis did not demonstrate any association with adverse outcomes in the NAFLD cohort[34].Furthermore, a study by Gaoet al[35] showed that patients with MAFLD and elevated serum interleukin-6 levels at admission are at higher risk for severe illness from COVID-19.However, mortality in the NAFLD cohort was associated with a pronounced inflammatory response.Therefore, what could be inferred from these results is that rather than attributing the severity of COVID-19 to underlying liver disease, it might possibly be a result of the general state of host inflammation in NAFLD patients.Increased liver fat has been independently associated with a higher likelihood of testing positive for COVID-19 in a United Kingdom based study[36].In a pooled analysis on the association of fatty liver and COVID-19, it was found that NAFLD was associated with an increased risk of severe COVID-19, even after adjusting for obesity as a possible confounding factor[37].From these results, one is led to believe that NAFLD is indeed independently associated with increased severity in COVID-19.Whether it is the liver disease that is responsible for this increasing severity, the general state of inflammation that accompanies NAFLD or the associated comorbidities that drives the outcome is a matter of debate.Interestingly, a recent study showed that the presence of fibrosis rather than the presence of MAFLD is associated with increased risk for mechanical ventilation, development of acute kidney injury, and higher mortality in COVID-19 patients[38].
LEAN VS OBESE NAFLD IN COVID-19
While a BMI greater than 23 kg/sq.metres increases the risk of developing fatty liver disease[39], many people with normal BMI’s are capable of developing NAFLD.Additionally, significant proportion of NAFLD patients do not have insulin resistance either[40,41].Termed ‘lean’ NAFLD, this so-called ‘entity’ indicates that there is more to NAFLD than just the mere presence of MS.Zhenget al[28] showed that compared to MAFLD patients without obesity those with obesity were at a 6-fold increased risk of severe COVID-19 illness and this association was significant even after adjusting for various parameters like diabetes, hypertension and dyslipidemia.This raises an important question as to whether the worse outcome in NAFLD patients is related to underlying liver disease or related to associated obesity? However, the small sample size of this study makes it difficult to arrive at such sweeping conclusions.Also, the cut-off for obesity in this study has been taken as 25 kg/m2.
INFLAMMATION IN NAFLD
The bidirectional relationship between hepatic steatosis and insulin resistance is well established[42].Hepatic steatosis can itself be a driver of insulin resistance and MS has opened avenues for further investigation in the pathophysiology of inflammation in NAFLD.There has been increasing evidence of the presence of significant cross-talk between the liver and other extrahepatic tissues and organs mediated by cytokines, hepatokines.It also involves nuclear factor-κB and c-Jun N-terminal kinase pathways which implies that hepatic inflammation could be a potential driver of cellular dysfunction, cell death and deleterious remodelling in various body tissues and organs[43].This state of chronic inflammation may directly impact disease severity by adding up to the dysregulated immune response in COVID-19.In a peripheral blood genomewide gene expression analysis among 1650 participants, it was observed that after adjustment for known risk factors, fatty liver was associated with blood gene sets of extracellular matrix turnover, inflammatory response, immune system activation and a prothrombotic state[44].This could lead to morbidities in multiple organs including the cardiovascular system, and may, in our opinion, exacerbate disease processes in COVID-19.
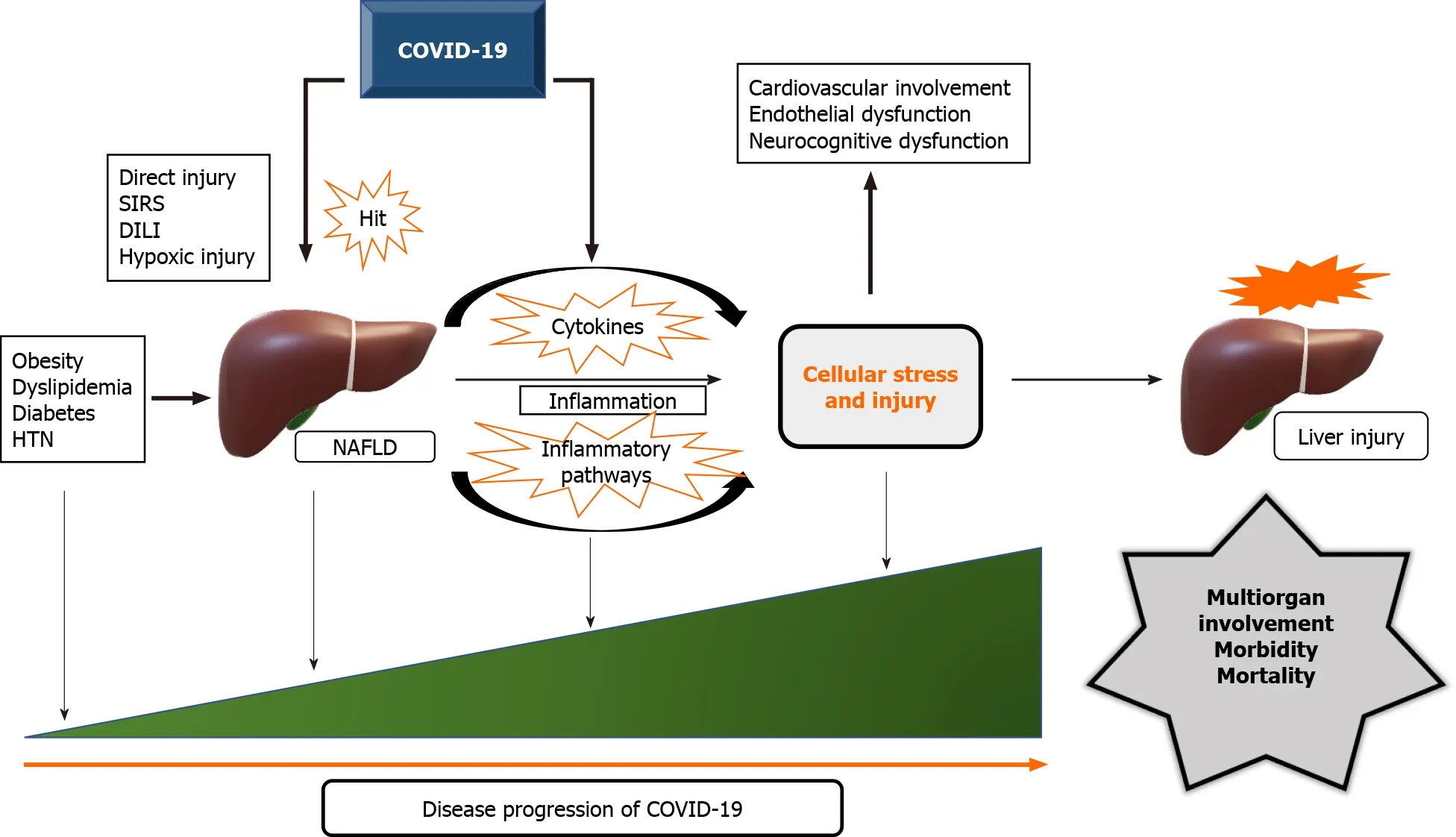
Figure 1 Pathophysiological processes driving disease progression in patients of nonalcoholic fatty liver disease with coronavirus disease 2019 and the impact on hepatic status.
LIVER INJURY IN NAFLD PATIENTS WITH COVID-19
NAFLD patients have been reported to be more likely to develop liver injury when infected by COVID-19[18].Median ALT levels and the proportion of elevated ALT were found to be significantly greater in patients with NAFLD than in patients without NAFLD on admission.In addition, the proportion of elevated ALT in patients with NAFLD was significantly higher than patients without NAFLD during hospitalization.However, severe liver-related complications during hospitalization were not observed in any of the patients.Mushtaqet al[17] found that NAFLD is an independent predictor of the development of mild to moderate liver injury in hospitalized patients with COVID-19.Moreover, COVID-19 patients with persistent liver injury have been found to have NAFLD and high BMI in one particular study[15].The APCOLIS study also found that the presence of MAFLD aggravates the risk of liver injury in COVID-19[13].In the study by Targheret al[33], COVID-19 patients with MAFLD with intermediate or high FIB-4 scores were more likely to have higher liver enzymes, compared with their counterparts with low FIB-4 score or those without MAFLD.The reasons for this increased likelihood of liver injury in NAFLD patients affected by COVID-19 could be multifactorial- pre-existing steatohepatitis, systemic inflammation, the severity of COVID-19 itself and a combination of any of these.The ‘cocktail’ of medications used in this pandemic deserves special attention while evaluating the relationship between NAFLD and COVID-19.Antivirals, antibiotics and glucocorticoids have been the most rampantly used medications in the quest to control COVID-19 and may contribute to liver injury, especially in those with NAFLD.
A summary of the pathophysiological processes that could presumably drive disease progression in patients of NAFLD with COVID-19 and the resulting impact on hepatic status is illustrated in Figure 1.
CONCLUSION
The bulk of the evidence-based on pooled analysis so far shows NAFLD patients are at increased risk of severe COVID-19 infection.However, judging by the results based on few studies that have been carried out to date, it seems the disease severity is determined more by the presence of co-morbidities like obesity, insulin resistance and dyslipidemia which are frequent accompaniments of NAFLD.The studies showing the association of NAFLD/MAFLD with severity of COVID-19 independent of associated comorbidities have shown conflicting results.The presence of fibrosis rather than the presence of MAFLD/NAFLD is associated with worse clinical outcomes and higher mortality in COVID-19 patients.Additionally, there seems to be an increased likelihood of liver injury in NAFLD patients with COVID-19.Further studies are required to delineate these pathophysiological details.
 World Journal of Hepatology2021年8期
World Journal of Hepatology2021年8期
- World Journal of Hepatology的其它文章
- Solid pseudopapillary neoplasm of the pancreas
- Non-invasive tests for predicting liver outcomes in chronic hepatitis C patients: A systematic review and meta-analysis
- Hepatocellular injury and the mortality risk among patients with COVID-19: A retrospective cohort study
- Clostridioides difficile infection in liver cirrhosis patients: A population-based study in United States
- Therapeutic plasma exchange in liver failure
- Current state of endohepatology: Diagnosis and treatment of portal hypertension and its complications with endoscopic ultrasound