Brugada syndrome associated with out-of-hospital cardiac arrest: A case report
2021-08-05 01:11:48GuoHuaNiHuaJiangLiMenYuanYuanWeiDilaXiangMa
World Journal of Clinical Cases 2021年19期
Guo-Hua Ni, Hua Jiang, Li Men, Yuan-Yuan Wei, Dila A, Xiang Ma
Guo-Hua Ni, Sichuan Academy of Medical Sciences & Sichuan Provincial People's Hospital(Chengdu Jinjiang Sohome Comprehensive Outpatient Clinic), Chengdu 610072, Sichuan Province, China
Hua Jiang, Department of Geriatrics, Affiliated Hospital of Chengdu University, Chengdu 610081, Sichuan Province, China
Li Men, Dila A, Xiang Ma, Department of Cardiology, First Affiliated Hospital of Xinjiang Medical University, Urumqi 830000, Xinjiang Uygur Autonomous Region, China
Yuan-Yuan Wei, Department of Physiology, Basic Medicine College, Chengdu University,Chengdu 610106, Sichuan Province, China
Abstract BACKGROUND Brugada syndrome (BrS) is an inherited disease characterized by an electrocardiogram (ECG) with a coved-type ST-segment elevation in the right precordial leads (V1-V3), which predisposes to sudden cardiac death (SCD) due to polymorphic ventricular tachycardia or ventricular fibrillation in the absence of structural heart disease. We report the case of a 29-year-old man with out-ofhospital cardiac arrest. BrS is associated with a high incidence of SCD in adults,and increasing the awareness of BrS and prompt recognition of the Brugada ECG pattern can be lifesaving.CASE SUMMARY A 29-year-old man suffered from out-of-hospital cardiac arrest, and after defibrillation, his ECG demonstrated a coved-type elevated ST segment in V1 and V2.These findings were compatible with type 1 Brugada pattern, and ECG of his brother showed a type 2 Brugada pattern. The diagnosis was BrS, NYHF IV,multiple organ dysfunction syndrome, sepsis, and hypoxic ischemic encephalopathy. The patient had no arrhythmia episodes after discharge throughout a follow-up period of 36 mo.CONCLUSION Increasing awareness of BrS and prompt recognition of the Brugada ECG pattern can be lifesaving.
Key Words: Brugada syndrome; Out-of-hospital cardiac arrest; Electrocardiogram;Ventricular fibrillation; Family history; Case report
INTRODUCTION
Brugada syndrome (BrS) is a rare genetically heterogeneous disease that increases the risk of sudden cardiac death (SCD). It was first described as a case series of eight patients who displayed a right bundle branch block with a history of aborted sudden cardiac death due to ventricular fibrillation (VF) and type 1 ECG in 1992 by Pedro and Josep Brugada[1]. It is estimated to be responsible for 4%-12% of all sudden deaths and at least 20% of deaths in patients with structurally normal hearts[2]. It is characterized by a distinct coved-type ST-segment elevation in the right precordial leads in the absence of significant structural heart disease[3]. Most BrS patients are asymptomatic throughout life, however, BrS typically presents a high risk of SCD, ventricular tachycardia (VT), and/or VF. Implantable cardioverter-defibrillator (ICD) is the only proven effective strategy for preventing SCD in BrS patients, but it has a significant complication rate and should be avoided in asymptomatic patients. Lifestyle measures are vital for asymptomatic patients with BrS.
CASE PRESENTATION
Chief complaints
A 29-year-old man was unresponsive for 5 d.
History of present illness
A 29-year-old man was admitted to our hospital after experiencing out-of-hospital cardiac arrest during sleep at home. He was found unresponsive by his wife, who is a nurse, and she initiated cardiac pulmonary resuscitation (CPR) immediately before the patient was emergently admitted to the local emergency department. The patient presented with VF and subsequently received two defibrillator-delivered electrical shocks (200 J and 300 J). He was intubated to maximize ventilation/oxygenation until the return of spontaneous circulation to sinus tachycardia (120 bpm). He did not experience an episode of chest pain, palpitations, syncope, or SCD prior to admission.His blood pressure was 122/70 mmHg, temperature was 38.5 °C, pulse was 102 bpm,and respiratory was 22 bpm. A small amount of moist rales could be heard in the lungs. The other general physical examinations were normal.
History of past illness
The patient had no history of any previous disease.
Personal and family history
There was no family history of SCD.
Physical examination upon admission
Post-arrest ECG demonstrated a typical type 1 Brugada ECG pattern, with coved-type ST-segment elevations of ﹥ 2 mm in V1 to V2 followed by a negative T-wave in two of the right precordial leads[2] (Figure 1A and B). A typical type 2 Brugada ECG pattern of his brother (25 years old, who had amaurosis) showed a convex ST-segment elevation (﹥ 0.5 mm) in one right precordial lead followed by a positive T-wave(Figure 2A).
Laboratory examinations
Routine blood tests showed a white blood cell count of 21.9 × 109/L (Normal reference range: 3.5-9.5 × 109/L), neutrophil count of 92.7 % (40 %-75 %), and hemoglobin level of 71 g/L (130-175 g/L). He had elevated creatine kinase (CK), 4600 IU/L (50-310 IU/L); CK-MB, 75 IU/L (0-25 IU/L); urea, 36 mmol/mL (3.1-8.0 mmol/mL); and creatinine, 1079 μmol/mL (53-115 μmol/mL). Serum alanine transaminase was 296 IU/L (15-40 IU/L), aspartate aminotransferase was 426 IU/L (9-50 IU/L), total bilirubin was 40.9 μmol/L (5,5-27.5 μmol/L), direct bilirubin was 12.8 μmol/L (0-8.6μmol/L), procalcitonin was 22 ng/mL (0-0.5 ng/mL), D-dimer was 7141 ng/mL (﹤ 280 ng/ml), fibrinogen degradation products were 93 μg/mL (0-5 μg/mL), activated partial thromboplastin time was 91.4 s (23-38 s), and brain natriuretic peptides was 5623 ng/L (0-125 ng/L). All the electrolytes were within the normal range. Echocardiography revealed no structural disease.
Imaging examinations
Chest radiography revealed pulmonary infection, and head computed tomography did not reveal any infarction or hemorrhage.
FINAL DIAGNOSIS
BrS, NYHF IV, multiple organ dysfunction syndrome, sepsis, and hypoxic ischemic encephalopathy.
Differential diagnosis
The main differential diagnosis for the presentation of out-of-hospital cardiac arrest in young adults included: BrS, ventricular tachycardia, left/right bundle branch block,short/long QT syndrome, early repolarization syndrome arrhythmogenic right ventricular cardiomyopathy, acute myocardial infarction, hypertrophic cardiomyopathy, and pulmonary embolism. The diagnosis of BrS is primarily based on a characteristic electrocardiographic pattern.
TREATMENT
After admission, the patient was started on an induced-hypothermia protocol,sedation, analgesia, and continuous renal replacement therapy.
The patient was administered with the following antibiotics: Linezolid injection 600 mg twice a day for 7 d, Sulperazon injection 3 g twice a day, and Mycamine injection 50 mg twice a day. Other therapies include correcting water-electrolyte and acid-base balance, nutritional support, protecting hepatorenal function, and so on. On hospital day 20, a tracheotomy was performed. The patient had no further episodes of VT/VF,and there were various ECG changes in the same lead during treatment (Figure 1C).
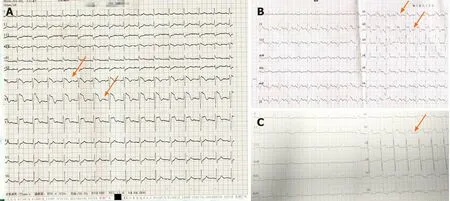
Figure 1 12-Iead eIectrocardiogram of the patient. A and B: A typical type 1 Brugada electrocardiogram (ECG) pattern, with coved-type ST-segment elevations of ﹥ 2 mm in V1 to V2 followed by a negative T-wave in two of the right precordial leads. C: ECG recording in the ward showing the elevation of V2-V3.
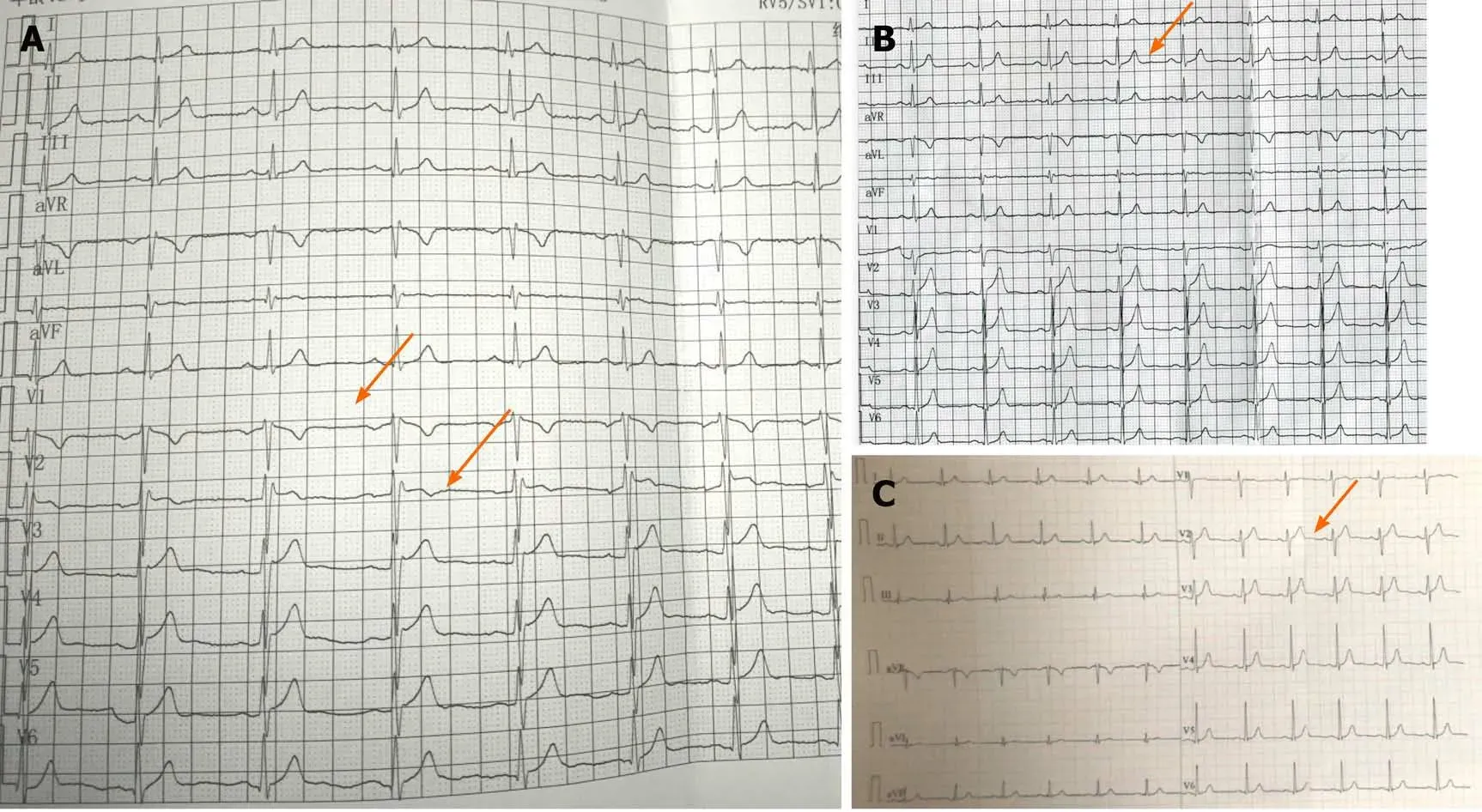
Figure 2 12-Iead eIectrocardiogram of the patient's brother. A: Typical type 2 Brugada electrocardiogram (ECG) pattern, with a convex ST-segment elevation ﹥ 0.5 mm in one right precordial lead followed by a positive T-wave (after placement of leads V1 and V2 in the third and second intercostal space). B: ECG recording in the normal condition showing sinus rhythm. C: ECG recording during follow-up showing sinus rhythm.
OUTCOME AND FOLLOW-UP
The patient refused an ICD for the secondary prevention of SCD. However, his brother received a Reveal LINQ Insertable Cardiac Monitor (ICM) for the primary prevention of SCD. We recommended genetic testing of the patient and his first-degree family members.
After a mean follow-up period of 36 mo, the patient had no arrhythmia episodes after discharge, and he was in good physical condition 3 years later. Subsequent ECGs on follow-up of the patient showed normal sinus rhythm. Through the Carelink Network, remote monitoring for his brother showed no ventricular arrhythmia during the follow-up, and ECG appeared sinus rhythm during follow-up (Figure 2C). The timeline summarizes the patient’s information, clinical findings, diagnostic tests,diagnosis, intervention, and follow-up (Figure 3).
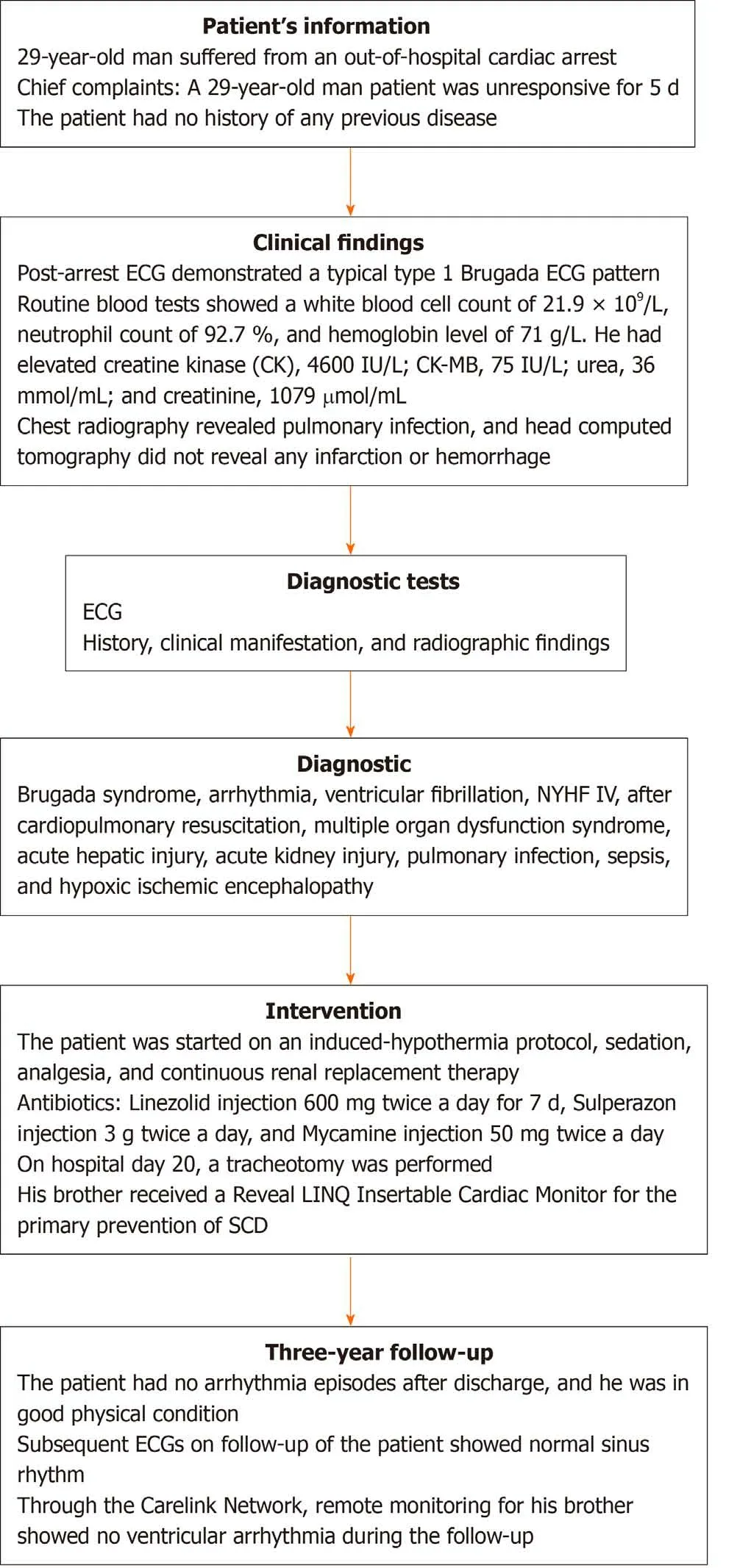
Figure 3 TimeIine summarizing the patient's information, cIinicaI findings, diagnostic tests, diagnosis, intervention, and foIIow-up. ECG:Electrocardiogram; SCD: Sudden cardiac death.
DISCUSSION
The cornerstone of BrS diagnosis and definition is its characteristic ECG pattern. The diagnostic ECG type 1 pattern is described as a prominent coved ST-segment elevation with type 1 morphology ≥ 2 mm in ≥ 1 lead in the right precordial leads V1 and V2, or ST-segment elevation ﹥ 2 mm followed by a negative T-wave. Type 2 pattern is also characterized by an ST-segment elevation followed by a positive or biphasic T-wave that results in a saddle back configuration. Furthermore, the pattern could be recorded not only in the classical V1 and V2 lead positioning, in the 4th intercostal space, but also in higher intercostal spaces[4-6]. The placement of the right precordial leads in more cranial positions (in the 3rd or 2nd intercostal spaces) increases the sensitivity in some patients because of variable anatomical correlation between the right ventricular outflow tract and V1 to V2 in the standard position[7,8]. The patient’s brother, who was 25 years old, had amaurosis twice before, and his ECG showed sinus rhythm(Figure 2B). However, after placement of leads V1 and V2 in the third and second intercostal spaces, his ECG presented with a typical 2 Brugada ECG pattern(Figure 2A). Letsaset al[9] demonstrated that the presence of a family history of SCD(﹤ 45 years of age) was an independent predictor and conferred a nearly nine-fold higher risk for future arrhythmic events.
ICD is effective in both primary and secondary prevention of SCD in patients with BrS[10]; however, inappropriate ICD interventions and ICD-related complications may lead to considerable morbidity[11]. After cautious risk-benefit analysis, the patient’s brother underwent the Reveal LINQ ICM, which provided continuous long-term heart monitoring.
However, the ECG patterns of BrS are transient and often concealed until unmasked during circumstances, such as fever, certain drugs, electrolyte disturbances,pneumonia, hypertestosteronemia, hyperthyroidism, and under vagotonic conditions(a large meal or the recovery phase of exercise)[12-14]. A link between fever and a Brugada type I pattern is very well known. Fever is recognized as a great risk factor for arrhythmia events in BrS patients, and the most frequent clinical manifestation associated with Brugada pattern was fever (83%)[15]. Fever can unmask the typical type I pattern as well as trigger arrhythmic events. Roterberget al[16] described a total of 53 patients who presented with BrS type I pattern induced by fever, and the incidence of arrhythmic events in patients with BrS type I pattern during fever was 38%.
A recent study reported that COVID-19 induced fever led to symptomatic BrS, and the threshold to run an ECG should be low in febrile patients with suspected COVID-19[17,18]. The patient in the study had a fever for more than 9 d, which was induced by pulmonary infection and sepsis. He presented with BrS type I pattern; however, the BrS type 2 pattern appeared in the same lead during treatment and follow-up.
In addition, BrS can be unmasked by drugs that affect ventricular sodium and potassium after exposure to certain drugs, such as antiarrhythmic drugs (propafenone,procainamide, and procaine), alcohol, and cocaine[19]. Drug-induced BrS is often asymptomatic; however, it can precipitate the Brugada pattern and trigger ventricular arrhythmias.
Education and lifestyle measures for the prevention of arrhythmia events are critical for asymptomatic patients and those with a family history of SCD. The wife of the patient initiated CPR immediately. All patients with BrS and their first-degree relatives should be informed about the precipitating factors, and during febrile episodes, fever should be treated immediately with antipyretics. It has been reported that 60 % of recurrent events are fever-related, especially in the pediatric group and those who experienced a previous fever-related arrhythmic event, and they should be admitted to the intensive care unit immediately for observation and treatment[20].
CONCLUSION
We have reported a successful clinical intervention of BrS type 1 patient with a family history of two affected members, and the successful management of the patient required the close cooperation of a multidisciplinary team, including the emergency department, cardiology department, coronary care unit, infectious disease department,nephrology department, nutritional department, respiration department, hepatology department, and so on.
This case illustrates the importance of increasing the awareness and recognition of the Brugada ECG pattern and differential diagnosis for young adults associated with out-of-hospital cardiac arrest. Prompt recognition of BrS ECG can be lifesaving.
ACKNOWLEDGEMENTS
We gratefully acknowledge the kind cooperation of the patient, the family members, and the staff from all the units for their assistance in conducting this study.
 World Journal of Clinical Cases2021年19期
World Journal of Clinical Cases2021年19期
- World Journal of Clinical Cases的其它文章
- Liver injury in COVID-19: Known and unknown
- Small bowel obstruction caused by secondary jejunal tumor from renal cell carcinoma: A case report
- Ectopic opening of the common bile duct into the duodenal bulb with recurrent choledocholithiasis: A case report
- Glutamic acid decarboxylase 65-positive autoimmune encephalitis presenting with gelastic seizure, responsive to steroid: A case report
- Four-year-old anti-N-methyl-D-aspartate receptor encephalitis patient with ovarian teratoma: A case report
- Neuromuscular electrical stimulation for a dysphagic stroke patient with cardiac pacemaker using magnet mode change: A case report