Primary rhegmatogenous retinal detachment: evaluation of a minimally restricted face-down positioning after pars plana vitrectomy and gas tamponade
2021-06-11 00:49:32KiichiroKusabaKotaroTsuboiTsuneakiHandaYukihikoShirakiTakuyaKataokaMotohiroKmaei
Kiichiro Kusaba, Kotaro Tsuboi, Tsuneaki Handa, Yukihiko Shiraki, Takuya Kataoka, Motohiro Kmaei
Department of Ophthalmology, Aichi Medical University,Tazako, Nagakute‐city, Aichi 480‐1195, Japan
Abstract
● KEYWORDS: retinal detachment; vitrectomy; flexible postoperative positioning
INTRODUCTION
A face‐down position is considered necessary for reattachment of a detached retina after pars plana vitrectomy (PPV) and gas tamponade for primary rhegmatogenous retinal detachment (RRD) in many regions and countries[1‐4].However, children, some older adults, and patients with cervical spondylosis, coronary heart disease, obesity, and other comorbidities have serious difficulties maintaining a face‐down position. Silicone oil tamponade is employed for those cases.Furthermore, in rare cases, the face‐down position can also cause systemic complications such as pulmonary embolism,thrombophlebitis, and ulnar nerve palsy[5‐7]. To overcome these problems, recent studies have reported that a strict face‐down position may not be necessary[8‐11]. PPV with complete drainage of subretinal fluid (SRF) and no face‐down positioning in the postoperative period leads to a high anatomical retinal reattachment rate in the primary pseudophakic RRD[4,8‐9].Chenet al[10]reported that for RRD repair, the primary retinal reattachment rate of PPV with gas tamponade and a flexible postoperative position (alternative upright or lateral recumbent)was the same as that with a strict face‐down position. According to Linet al[12], PPV with a flexible postoperative position (face‐down position or alternatively face‐down or lateral position,according to the location of retinal tears) has a primary retinal reattachment rate up to 93.3%[13]. However, there are no reports showing that the patients were recommended a face‐up positioning, thus implying lying on the back or any other position that prevents downward movement of retinal tears after PPV. This study aimed to provide evidence on the safety and efficacy of minimally restricted positioning after PPV and gas tamponade for primary RRD.
SUBJECTS AND METHODS
Ethical ApprovalThis study was approved by the Institutional Review Board (IRB) of Aichi Medical University Hospital and was conducted in accordance with the Declaration of Helsinki.Consent was obtained from all subjects, who were informed of the nature of the disease and of all potential treatment options.This observational study reviewed the records of 40 eyes belonging to 39 patients who had primary RRD and had undergone PPV. The procedures were conducted at the Aichi Medical University Hospital between September 2015 and August 2017, and the patients were followed up for at least 6mo.
The exclusion criteria were as follows: 1) primary RRD with a history of intraocular surgery other than cataract surgery,2) previous retinal reattachment surgery, 3) giant retinal tear or RRD caused by trauma, 4) proliferative vitreoretinopathy(PVR), 5) macular hole retinal detachment, and 6) a follow‐up period of less than 6mo.
Each patient received a complete ocular examination, including best‐corrected visual acuity (BCVA) measurement converted to the logarithm of the angle of minimal resolution (logMAR),intraocular pressure (IOP), slit‐lamp examination, and fundus examination with a binocular indirect ophthalmoscope. The number, type, location, and size of the retinal tears were diagnosed and recorded during the surgery. All patients underwent almost the same surgical procedure. PPV was performed using either a 25‐G system (Constellation; Alcon Laboratories, Inc., Fort Worth, TX, USA) or a 27‐G system(EVA; Dutch Ophthalmic Research Center, Zuidland, the Netherlands) after administration of sub‐Tenon’s anesthesia with 2% lidocaine. Trocars of 25‐G or 27‐G were placed at 3.5 to 4 mm posterior to the limbus. Simultaneous cataract surgery was performed for all phakic eyes.
The mean age of the patients was 59.2y, and most of them suffered from age‐related cataracts. As the vitrectomy procedure can accelerate age‐related cataract formation, we performed simultaneous cataract surgery instead of subsequent treatments for cataract and vitreoretinal pathology. In two other cases of relatively young patients (19y and 23y), simultaneous cataract surgeries were performed as the eyes had traumatic cataracts and dialysis tears along with liquified vitreous bodies due to posterior vitreous detachment (PVD).
All cataract surgeries were performed through a clear corneal 2.4‐mm incision. After the cataract surgery, a core vitrectomy followed by a peripheral shaving with scleral depression was performed to remove any residual traction. If the macula was detached or if the RRD was highly bullous, liquid perfluorocarbon (Perfluoron?, Alcon Laboratories, Inc.) was injected into the vitreous cavity to flatten the detached retina.All retinal tears were surrounded by two to three rows of confluent endophotocoagulation. Lattice degeneration and atrophic retina were treated with laser photocoagulation. An intentional hole was not created unless the SRF was highly viscous. A complete fluid‐air exchange was performed. Sulfur hexafluoride (SF6, 20%) or perfluoropropane gas (C3F8, 6%‐8%)was then used to fill the vitreous cavity. The choice to use SF6or C3F8was left to the surgeon’s discretion for each subject.The patients were instructed to keep flexible head positions to avoid original breaks downward and reopening in the vitreous fluid for around 1wk after the surgery. For example, patients with superior breaks were given no specific instruction with respect to their position. Patients with a lateral break were instructed only to avoid lying on the ipsilateral side of the original retinal tear. These patients were allowed to stay in the upright position when sitting, standing, or walking, or the side position with the break‐side up, face up (supine position),or face down when lying on a bed. Patients with an inferior break were instructed to avoid only the upright position, that is, to look down when sitting, standing, or walking, and were allowed any position when lying on a bed. A face‐up position(lying on the back) was recommended for any type of breaks and especially for those with inferior breaks. The face‐down postoperative position was only temporarily asked for cases with macular detachment for a couple of hours immediately after surgery. Postoperative examinations were performed every day during hospitalization, almost for a week, and at 2wk, 1, and 3mo after surgery. Some patients were followed up as necessary. IOP, anatomical status of the retina, and postoperative complications were recorded at each follow‐up visit. Visual acuity was measured during visits after the intraocular gas was absorbed. The primary outcome was defined as the primary and final anatomical reattachment rate at the 6‐month visit after surgery. The secondary outcome was defined as changes in the BCVA and the incidence of postoperative complications.
Statistical AnalysisContinuous variables were presented as means and standard deviations, whereas categorical variables were expressed as numbers and percentages.
RESULTS
Forty eyes of 39 patients with primary RRD were included in this study (29 eyes of 28 males, 72.5%; 11 eyes of 11 females,27.5%). The mean age was 59.2±13.0y (range, 19‐86y). The mean follow‐up period was 4.5±0.9mo. The baseline clinical characteristics of the enrolled patients are shown in Table 1.
The mean number of quadrants affected was 1.8±0.7 (range,0.5‐4). Of the 40 eyes, 30 eyes (75.0%) had a single break,nine eyes (22.5%) had multiple breaks, and one eye (2.5%)had an oral dialysis. Of the retinal tears, 33 eyes (82.5%) had horseshoe tears, six eyes (15.0%) had atrophic holes, and one eye with a retinal tear and vitreous collagen liquefaction dueto PVD (2.5%) had an oral dialysis. Of 30 eyes with a single tear, 17 (56.7%) of the retinal tears were in superior areas (10 to 2 o’clock); nine (30.0%) were located in lateral areas (2 to 4 o’clock or 8 to 10 o’clock); four (13.3%) were located in the inferior areas (4 to 8 o’clock). The macula was detached in 14 eyes (35.0%) and still attached in 26 eyes (65.0%).
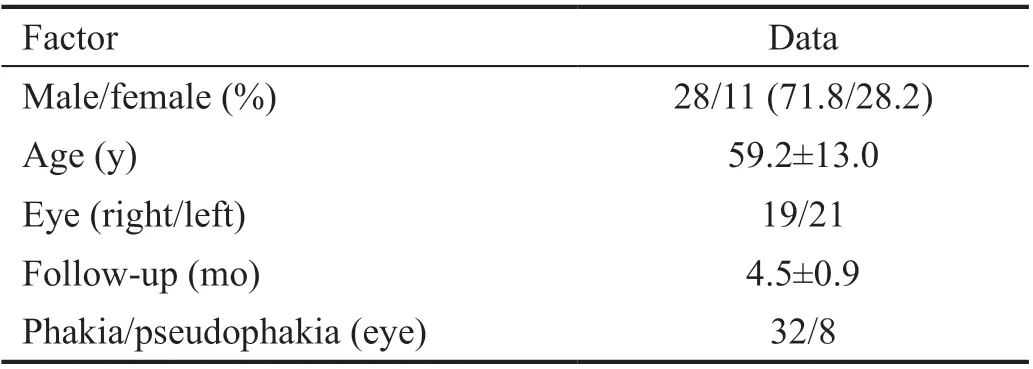
Table 1 Baseline clinical characteristics of patients (n=39) with primary rhegmatogenous retinal detachment
Simple PPV was performed for eight pseudophakic eyes(20.0%), and the triple procedure of PPV with simultaneous phacoemulsification plus intraocular lens (IOL) implantation was performed for the remaining 32 phakic eyes (80.0%). The 25‐G Constellation vitrectomy system was used for 31 eyes(77.5%), and the 27‐G EVA vitrectomy system was used for nine eyes (22.5%). Liquid perfluorocarbon was used in 18 eyes(45.0%). An intentional hole for internal drainage of subretinal fluid was created in three eyes (7.5%). As a tamponade, 20%SF6was used in 31 eyes (77.5%) and 6%‐8% C3F8was used in nine eyes (22.5%).
Initial reattachment was achieved in 36 eyes (90%). Final reattachment was achieved in 40 eyes (100%). Two eyes(5.0%) detached again due to new retinal tears, and one eye(2.5%) detached again due to a hole caused by overpowered endophotocoagulation around the original break. One eye(2.5%) detached again due to a failure in the development of the chorioretinal scar around the original break. Postoperative complications included IOP elevation (ranging from 25 to 44 mm Hg) in 11 eyes (27.5%), which was successfully treated with topical and oral medications; fibrin formation in two eyes (5.0%), which was treated with a steroid ointment;pupillary capture of the IOL in two eyes (5.0%), which was treated by maintaining face‐down postoperative position with tropicamide drops; posterior synechia in one eye (2.5%),which was released with a 30‐G needle; and residual subretinal perfluorocarbon in one eye (2.5%), which was observed because its size was small and its location was around the vascular arcade with no visual field loss.
DISCUSSION
This study aimed to provide evidence on the safety and efficacy of this minimally restricted positioning, including face‐up positioning, after PPV and gas tamponade for RRD.The anatomical success rate was 90.0% (36 cases) after the primary surgery and eventually 100%, which is almost equal to the anatomical success rate of previous reports employing face‐down positioning (85.4%‐91.0%)[2].
A number of groups have reported the efficacy of non‐face‐down positioning after vitrectomy during RRD management[4,8‐12,14]. Those studies were principled on the effects of gas tamponade on surface tension rather than buoyancy. Due to the surface tension of the gas, intraocular fluid cannot access the subretinal space through retinal tears[15‐16]. Kuhn and Aylward[17]reported that the relation between intraoperative SRF drainage and simple gas coverage of the retinal tears after sufficient photocoagulation is a key feature for chorioretinal adhesion[18‐20]. However, especially for an inferior break, continuous contact with the gas is very hard because it is impossible for patients to keep a complete face‐down position all day long for several days[21‐23].
There are risks of glaucoma associated with vitrectomy[24‐25].Frammeet al[26]reported that the IOP after PPV with gas tamponade was slightly elevated and peaked at 24h. Wonget al[16]reported that there was a 20%‐21% increase in the rate of postoperative IOP of 30 mm Hg for patients after PPV with gas tamponade. Our results are similar to those of the aforementioned reports. The mean IOP peaked on postoperative day 1 and returned to normal (with the help of medication in some cases) within 7d. Our results indicate that postoperative posture has a minor impact on the change in IOP that was reported by previous studies[11‐12]. However, it should be considered that a face‐up positioning poses a risk of secondary pupillary block or angle closure glaucoma in patients[10]. In our study, only six cases had a postoperative IOP of 30 mm Hg, which is low, and complications such as pupillary block and iris bombe did not occur. In this study,there were complications of pupillary capture of the IOL in two eyes (5.0%), posterior synechia in one eye (2.5%),and fibrin formation in two eyes (5.0%). It is also hard to compare the rates of these instances with other studies since the complications of pupillary capture of the IOL and posterior synechia after vitrectomy for RRD have not been reported. Shirakiet al[11]reported significant fibrin formation more often in the anterior chamber 1d after vitrectomy in a group with prone positioning (26.2%) compared with a non‐prone positioning group (12.8%). In eyes filled with gas,inflammatory cells and cytokines should accumulate inferiorly after vitrectomy. With C3F8(6%‐8%), the gas in the vitreous cavity disappears in approximately 30d, which is longer than that with SF6(2wk), and C3F8is most commonly used as the intraocular gas to manage complicated RRD. Although the cases in the present study did not include PVR, C3F8was used at the surgeon’s discretion.
Our study had some limitations. First, it was an observational study with a non‐randomized design. Second, we did not have a control group that used a strict face‐down position.The primary retinal reattachment rate of 90% that we used to compare our results with was taken from previous studies. We believe that a large retrospective study can provide stronger evidence as to whether patient positioning is important postoperatively, and ideally, a prospective randomized controlled study is required.
ACKNOWLEDGEMENTS
Editorial support, in the form of medical rewriting, assembling tables based on authors’ detailed directions, collating author comments, copyediting, fact checking, and referencing, was provided by Editage, Cactus Communications.
Conflicts of Interest: Kusaba K,None;Tsuboi K,None;Handa T,None;Shiraki Y,None;Kataoka T,None;Kamei M,None.
 International Journal of Ophthalmology2021年6期
International Journal of Ophthalmology2021年6期
- International Journal of Ophthalmology的其它文章
- A decrease in macular microvascular perfusion after retinal detachment repair with silicone oil
- Role of bevacizumab intraocular injection in the management of neovascular glaucoma
- Rectangular 3-snip punctoplasty versus punch punctoplasty with silicone intubation for acquired external punctal stenosis: a prospective randomized comparative study
- Association of eleven single nucleotide polymorphisms with refractive disorders from Eskisehir, Turkey
- Evaluation of macular vessel density changes after vitrectomy with silicone oil tamponade in patients with rhegmatogenous retinal detachment
- Triamcinolone as an adjunct to the combination of anti-VEGF for the management of diabetic macular edema