Prevalence and associated factors of obesity in inflammatory bowel disease: A case-control study
2021-01-15 08:59:44GiuseppeLosurdoRosaFedericaLaFortezzaAndreaIannoneAntonellaContaldoMicheleBaroneEnzoIerardiAlfredoDiLeoMariabeatricePrincipi
World Journal of Gastroenterology 2020年47期
關鍵詞:農村
Giuseppe Losurdo, Rosa Federica La Fortezza, Andrea Iannone, Antonella Contaldo, Michele Barone, Enzo Ierardi, Alfredo Di Leo, Mariabeatrice Principi
Abstract
Key Words: Inflammatory bowel disease; Obesity; Body mass index; Antibiotics; Risk factor; Corticosteroids
INTRODUCTION
Obesity is a growing problem in developed countries, since it is going to become the leading cause for mortality due to cardiovascular events[1]. In Italy, it is estimated that about the 18% of population is suffering from obesity[2]. The World Health Organization (WHO) defines obesity by a value of body mass index (BMI) above 30 kg/m2, but obesity underlies as well an excessive visceral fat distribution, with several alterations at hormonal, inflammatory and endothelial level[3]. Inflammatory bowel disease (IBD) is a group of chronic inflammatory autoimmune disorders of gastrointestinal tract, mainly represented by Crohn’s disease (CD) and ulcerative colitis (UC). The problem of obesity is spreading in the context of IBD, since, in the past, it has been rarely recognized for the frequent association between IBD and malnutrition. However, nowadays, novel and more effective drugs are able to stop the progression of the disease, thus preventing malnutrition[4]. Indeed, a study performed in 2002 found a prevalence of obesity in CD of about 3%[5]; one decade later, however, in another study a prevalence of 31.5% was recorded[6]. Co-occurrence of obesity and IBD is not just a casual phenomenon and it has been emphasized that obesity may lead to a higher risk of perianal complications, higher hospitalization rates and greater risk of disease flares[5]. Moreover, obese patients with IBD on azathioprine were more likely to need courses of systemic corticosteroids and had higher recurrence rates after stopping the drug[7]. Furthermore, it has been estimated that an increase of one unit of BMI may increase the risk of therapeutic failure of 4%[8]and, in particular, a high BMI was an independent predictor of adalimumab therapy failure[9]. Considering that IBD per se could increase the risk of endothelial dysfunction and cardiovascular risk[10,11], the association between obesity and IBD may represent a very important issue.
Therefore, we aimed, in a case-control study, to investigate the prevalence of obesity in IBD patients and detect possible factors associated to this condition.
MATERIALS AND METHODS
Patients
We consecutively recruited IBD patients referred to our outpatient tertiary Gastroenterology Unit (University Hospital Policlinico, Bari, Italy) in the period October 2016-October 2017. We only excluded patients aging < 18, doubtful IBD diagnosis and those who refused to participate in the study. Outpatients with functional gastrointestinal disorders constituted the control group. The study was approved by the independent Ethics Committee of the Policlinico di Bari (protocol No. 4862) and was performed according to the Helsinki declaration 1975 statements.
For each patient, age, sex, abdominal circumference, weight and BMI, smoking habits and relevant comorbidities were collected. Obesity was diagnosed when BMI > 30[3]. For IBD patients, the diagnosis was achieved by a combination of endoscopy, histology (in all cases) and, for all CD patients, a transmural evaluation by magnetic resonance enterography. Then, we collected data about IBD staging (according to Montreal classification), clinical disease activity [partial Mayo for UC and Harvey-Bradshaw index (HBI) for CD] and specific therapies. For IBD patients we recorded data about laboratory investigations, in particular full blood count, erythrocyte sedimentation rate (ESR), C reactive protein (CRP), parameters of liver function, glucose and fat homeostasis. Liver steatosis was diagnosed by abdominal ultrasound, according to known criteria and already described in a previous experience[12,13].
Controls underwent only anthropometric and clinical history assessment, because all examinations that have been performed for IBD are not indicated nor refunded by Italian Health Service.
Statistical analysis
At univariate analysis, we compared IBD patients with and without obesity. Student's t test was used for continuous variables, while the chi-square test was used for discrete variables. Correlation was analyzed by Pearson’s r. Significant factors in univariate analysis were analyzed at multivariate analysis by binary logistic regression, considering obesity as an independent variable. Odds ratios (ORs) and respective 95% confidence intervals (CI) were calculated. All analyses were two-tailed; P values < 0.05 were considered statistically significant. The analysis was carried out using SPSS.21 software for Windows.
RESULTS
Patients characteristics
We enrolled 807 patients with IBD. The process of patients selection is reported in Figure 1. Four hundred seventy-four patients were male (58.7%); the average age was 46.2 ± 13.2 years. The average age of onset of IBD was 20 ± 9.4 years and we did not find any difference of age onset between UC and CD (19.8 ± 6.8 vs 20.4 ± 6.2; P = 0.19). Of these, 438 (54.2%) patients had CD and 369 (45.8%) UC.
The majority of CD patients had an inflammatory behavior (54.1%) and an ileal localization (45.2%); perianal involvement was reported only in 3 patients (0.68%). The 24.9% of patients with CD had undergone previous surgical treatment. The average clinical disease activity detected at enrollment and assessed by Harvey Bradshaw Index was 1.3 ± 2.4.
Regarding UC, 164 (44.4%) patients had proctitis. 30 patients (8.1%) had undergone colectomy. The mean clinical activity of disease detected at the time of enrollment, assessed by Mayo partial Score, was 1.7 ± 1. Further details about baseline features of IBD population are reported in Table 1.
We enrolled 378 controls, who were comparable to IBD group for age and sex, asshown in Table 2, reporting the main characteristics of IBD patients and controls.
建立多層次、多方面的農村社會保險、社會福利、社會救助和社會互助的體系,擴大農村基本養老保險、醫療保險、失業保險等的覆蓋面,堅持并優化“置換社會保障”和“置換宅基地”政策[20-25],如永久放棄土地承包經營權的農民,可以按照征地補償標準享有社會保障和就業扶持。
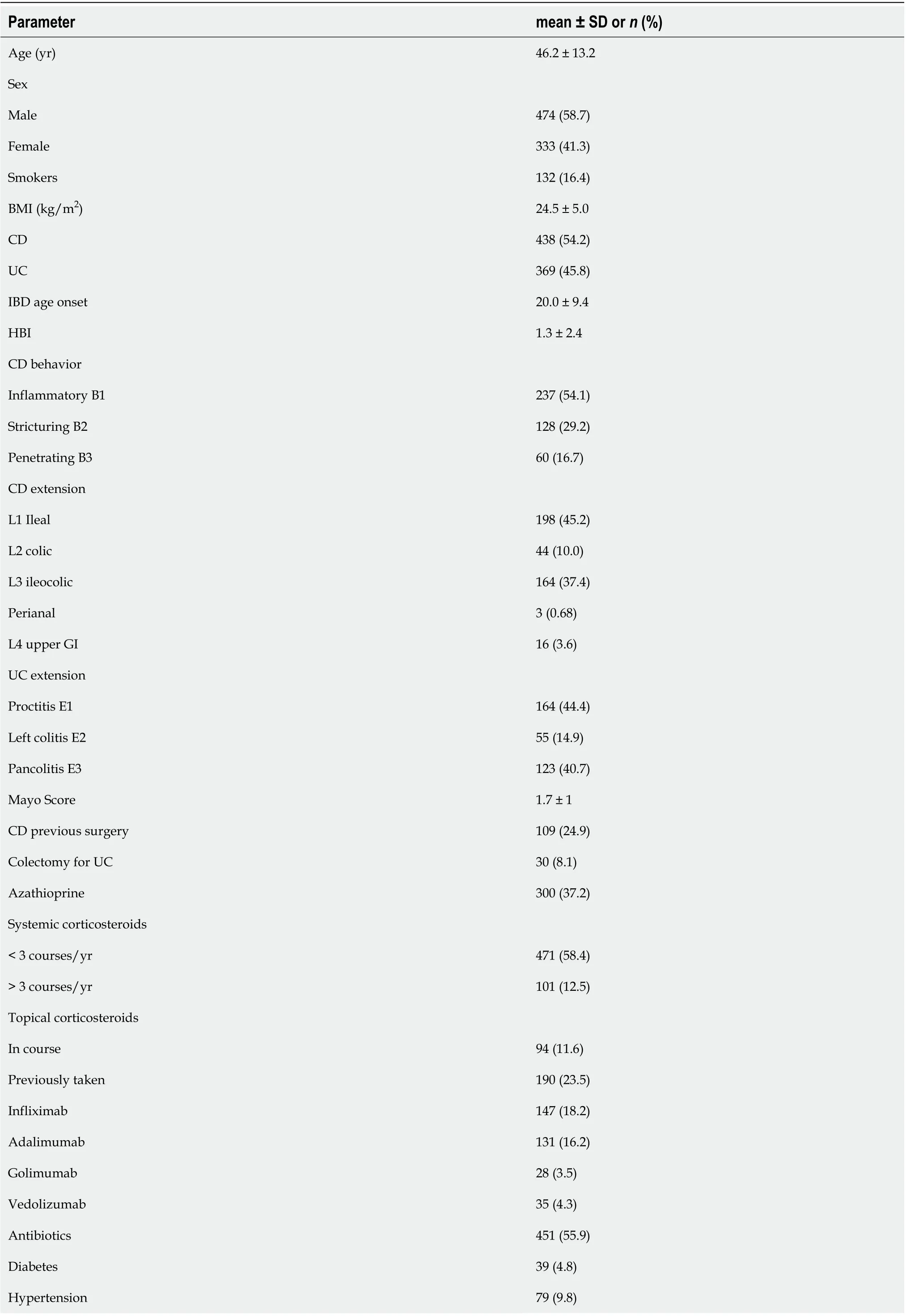
Table 1 Baseline demographic and disease characteristics of inflammatory bowel disease population

Waist circumference (> 102 cm males, > 88 females)138 (17.1)Liver steatosis 232 (28.7)BMI: Body mass index; UC: Ulcerative colitis; CD: Crohn’s disease; IBD: Inflammatory bowel disease; HBI: Harvey-Bradshaw index; SD: Standard deviation; GI: Gastrointestinal.
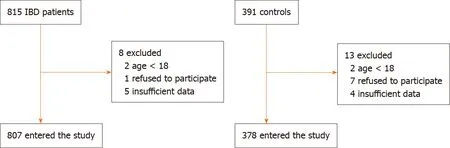
Figure 1 Flowchart reporting the process of patients selection. IBD: Inflammatory bowel disease.
The prevalence of obesity was 6.9% in IBD and 7.9% in controls (not statistically different; P = 0.38). Values of BMI were comparable between the two groups (24.5 ± 5.0 vs 24.4 ± 4.4, P = 0.74). More patients with hypertension and more smokers were observed in control group. Obesity rate did not differ between CD and UC (respectively 7.3% and 6.5%, P = 0.65).
Obesity in IBD vs controls
In the comparison of obese IBD patients and obese controls, we did not find any difference in main comorbidities (diabetes and hypertension). No differences in sex or smoking habits were observed. Obese IBD patients were younger than obese controls (51.2 ± 14.9 years vs 60.7 ± 12.1 years, P = 0.03). Additionally, an abdominal circumference > 102 cm in males and > 88 cm in females was observed more frequently in obese IBD group (83.9% vs 46.7%, P < 0.001). The results of such analyses are graphically represented in Figure 2.
Factors associated to obesity in IBD
At univariate analysis, we compared IBD obese vs IBD non obese patients. We observed that obese ones were older than normal weight subjects (51.2 ± 14.9 vs 44.5 ± 15.8, P = 0.002). IBD onset age was earlier in obese population (44.8 ± 13.6 vs 35.6 ± 15.6, P = 0.004). We did not detect any difference regarding other considered characteristics of IBD, such as disease location according to Montreal classification. When the drugs used for IBD therapy were taken into account, obese subjects had consumed more frequently long courses of systemic steroids (66.6% vs 12.5%, P = 0.02) as well as antibiotics such as metronidazole or ciprofloxacin (71.4% vs 54.7%, P = 0.05). No difference about other drugs (biologics, mesalazine or thiopurines) was observed.
Disease activity was similar between obese and non obese subjects both for UC and CD. Indeed, among UC patients, we did not find any correlation between BMI and partial Mayo subscore (r = -0.06; P = 0.25), as illustrated in Figure 3A. Clinical remission phase was observed respectively in the 41.6% and 49.3% of obese and non obese UC patients (P = 0.53; Figure 3B). Among CD patients, we similarly did not detect any correlation between BMI and HBI (r = -0.09; P = 0.08), as reported in Figure 4A. Clinical remission phase was observed respectively in the 93.7% and 87.7% of obese and non obese CD patients (P = 0.41; Figure 4B).
Obese IBD patients suffered more frequently from arterial hypertension (42.8% vs 15.3%, P < 0.001), type 2 diabetes (21.4% vs 3.7%, P < 0.001), liver steatosis (76.8% vs 25.2%, P < 0.001), and had a significantly higher value of abdominal circumference equal to or greater than the cut-offs of central obesity (83.9% vs 17.3%, P < 0.001). Regarding laboratory investigations, obese IBD patients had higher levels of triglyceridemia (161 ± 71 vs 107 ± 55, P < 0.001), fasting blood glucose (113 ± 46 vs 89 ± 18, P < 0.001) , gamma-glutamyl-transpeptidase (0.89 ± 0.99 vs 0.55 ± 0.91, P = 0.04), and low blood levels of HDL Cholesterol (47 ± 12 vs 56 ± 19, P = 0.001).
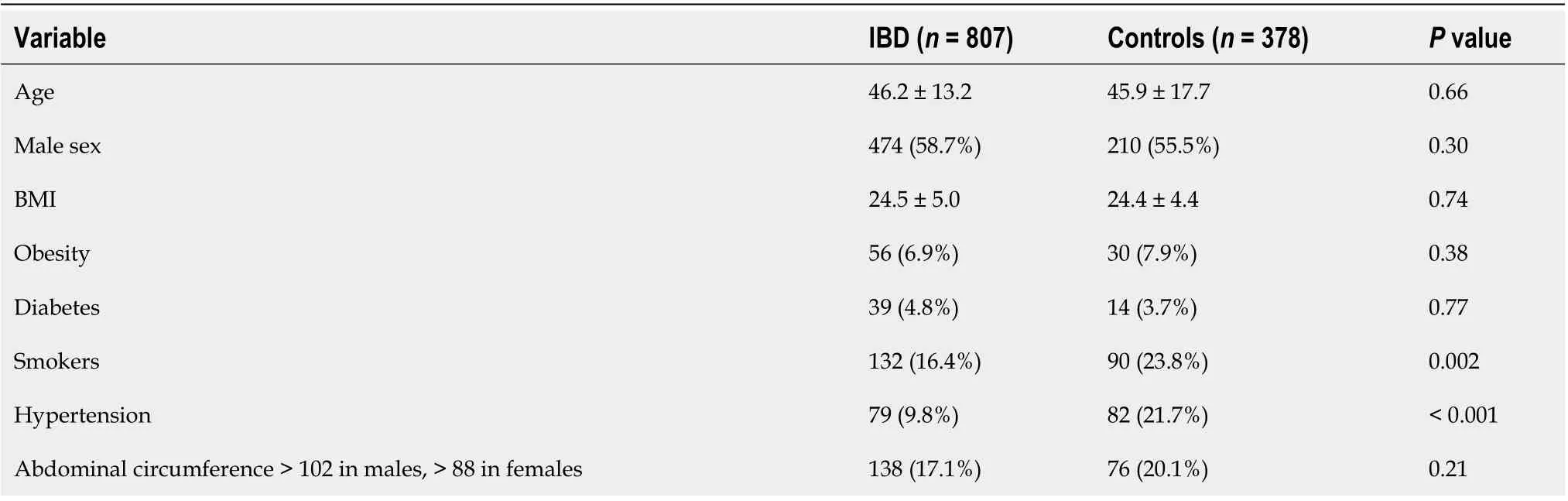
Table 2 Main characteristics of inflammatory bowel disease patients and controls
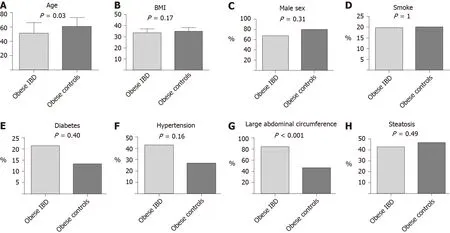
Figure 2 Comparison between obese inflammatory bowel disease and controls. A: Age; B: Body mass index; C: Sex; D: Smoking habits; E: Diabetes; F: Hypertension; G: Abdominal circumference > 102 in males and > 88 in females; H: Liver steatosis. BMI: Body mass index.
On multivariate analysis, however, the only factor that appeared to be independently linked to obesity in IBD was the high abdominal circumference (OR = 16.3, 95%CI: 1.03-250, P = 0.04).
DISCUSSION
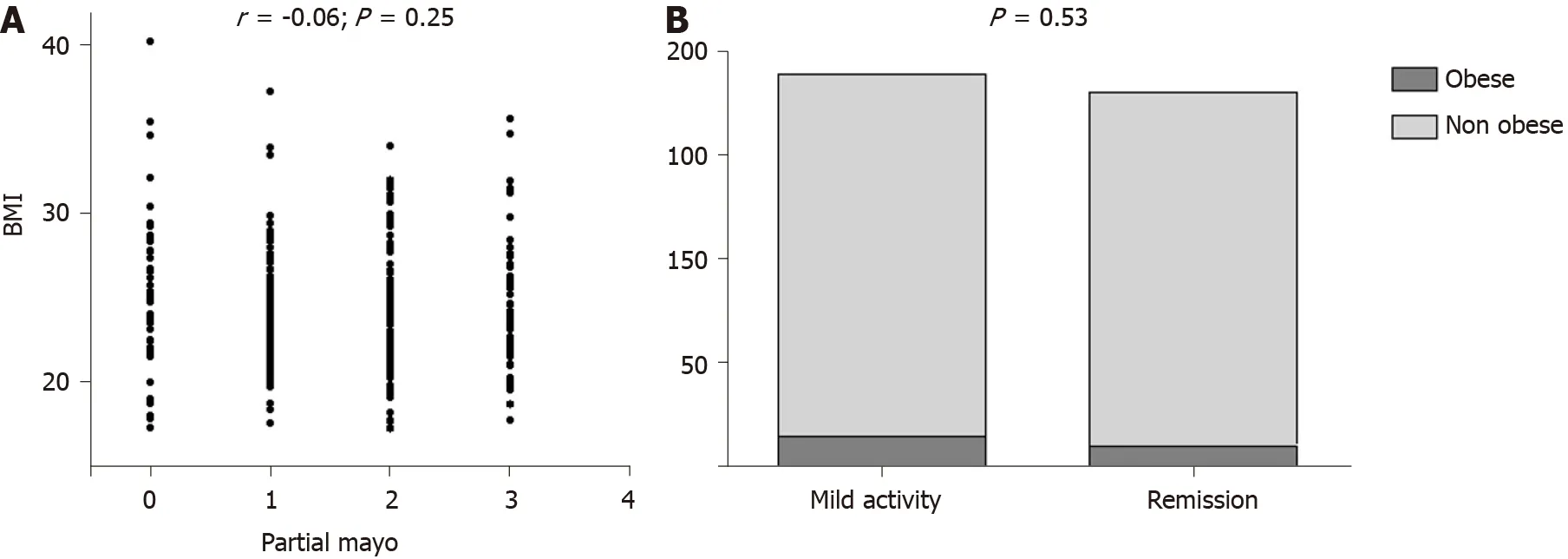
Figure 3 Correlation between ulcerative colitis clinical activity and body mass index. A: Scatterplot of body mass index and partial Mayo scores; B: Distribution of activity phase according to obesity status. BMI: Body mass index.
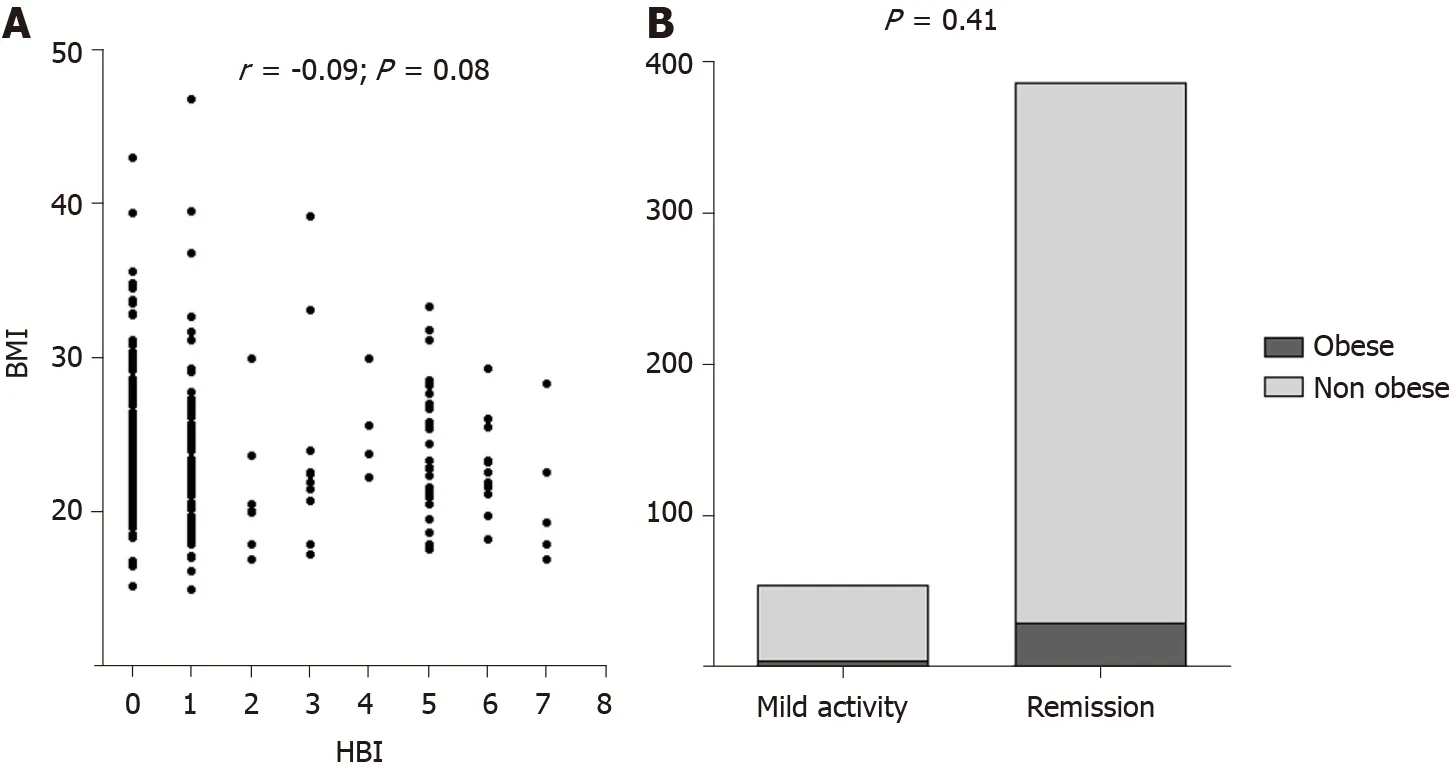
Figure 4 Correlation between Crohn’s disease clinical activity and body mass index. A: Scatterplot of body mass index and Harvey-Bradshaw index scores; B: Distribution of activity phase according to obesity status. BMI: Body mass index; HBI: Harvey-Bradshaw index.
The prevalence of obesity in IBD, a hot topic at the moment, has been investigated in several studies, showing highly variable values ranging from 5% to 30%[5,6]. A Scottish study based on a population of 489 IBD patients showed that 18% of patients had the features of obesity (compared to 23% of the general population); obese patients with CD were 18%, while obese patients with UC were 17.5%[14]. In the present study, we found a similar prevalence between controls and IBD which seems to confirm data from literature. The obesity rate in our cohort (6.9%) was only slightly lower than the 10.8% in the general population reported according to the European Eurostat survey[15]. Our results, additionally, underline that obesity in IBD patients has some peculiar features in comparison with obese controls. In detail, obese IBD subjects are younger than control counterpart, and this could be explained by the fact that, during the history of the disease, some factors such as steroid consumption could have favored weight gain. However, only at univariate analysis, steroid use was a predictor of obesity in IBD even if we were able to evaluate simply the exposure, and not its amount, and this could be considered as a limitation in our study. Additionally, the number of relapses occurred during the clinical history of patients was not collected from medical records, and this could be another limitation. Another feature of obese IBD patients is that they tend to have less frequently a large abdominal circumference than obese controls (Figure 2G), thus suggesting the possibility that fat distribution could be also localized in areas different than waist, such as hip or limbs. Indeed, some studies evidenced that in IBD the ratio between visceral and subcutaneous fat is altered[16]compared to healthy population, and this may explain our finding. Unfortunately, we did not take other anthropometric measurements, therefore we were unable to confirm this hypothesis.
Furthermore, we did not find any correlation between disease activity and BMI. This could be in disagreement with some literature data, showing that visceral fat[17,18]and high BMI[19]are associated with a dismal prognosis. However, our study was cross-sectional, therefore we could not evaluate the evolution of the disease during a follow up period. This could be acknowledged as another limitation. Nevertheless, some other studies did not find a strong association between BMI and disease activity and prognosis[20-23], and this underlines how this topic is still debated and with conflicting evidences.
Another important finding was that only the abdominal circumference was independently associated with obesity in IBD. We are aware that this could be an obvious result, but if we consider that it was not very common in our cohort (less than 50%), it is noteworthy to be underlined. Systemic steroids were associated with obesity only at univariate analysis, and this is an easily comprehensible link that has been already elucidated in literature[24]. Another interesting result was the most extensive use of antibiotics in obese IBD subjects. It is presumable that they could promote a dysbiosis, which in turn might facilitate the development of obesity, as already suggested by many clinical and basic science studies[25]. Finally, the high risk of diabetes, hypertension and liver steatosis is a well know phenomenon that seems to be related to obesity rather than to IBD itself[26].
CONCLUSION
In conclusion, our study may lay the foundation for some additional speculations. Since epidemiologically IBD are increasing in developed countries, the pathogenetic role and influence on the outcome of disease played by the diet should not be underestimated and must be further investigated. In this regard, it has been already demonstrated that IBD patients, even in remission phase, tend to have a high lipid and low fiber intake[27]. Furthermore, It may be useful to plan new clinical studies aimed at evaluating clinical, laboratory and endoscopic parameters at the baseline and following BMI changes induced by dietary regimens, since this topic is still very poorly investigated.
ARTICLE HIGHLIGHTS

猜你喜歡
今日農業(2022年1期)2022-11-16 21:20:05
今日農業(2021年21期)2022-01-12 06:32:04
音樂教育與創作(2020年12期)2020-12-25 06:49:44
音樂教育與創作(2020年9期)2020-02-21 20:13:37
活力(2019年21期)2019-04-01 12:17:48
民族音樂(2018年6期)2019-01-21 09:30:04
中國公路(2017年16期)2017-10-14 01:04:28
湖南農業(2017年1期)2017-03-20 14:04:48
草原歌聲(2016年2期)2016-04-23 06:26:27
新教育時代電子雜志(學生版)(2015年31期)2015-12-20 08:29:14
 World Journal of Gastroenterology2020年47期
World Journal of Gastroenterology2020年47期
- World Journal of Gastroenterology的其它文章
- Artificial intelligence-aided colonoscopy: Recent developments and future perspectives
- Invasive fungal infection before and after liver transplantation
- Molecular overview of progressive familial intrahepatic cholestasis
- Evaluation of an educational telephone intervention strategy to improve non-screening colonoscopy attendance: A randomized controlled trial
- Towards an evaluation of alcoholic liver cirrhosis and nonalcoholic fatty liver disease patients with hematological scales
- Extracellular histones stimulate collagen expression in vitro and promote liver fibrogenesis in a mouse model via the TLR4-MyD88 signaling pathway