Embolization of pancreatic arteriovenous malformation: A case report
2020-05-14 01:51:14
World Journal of Clinical Cases 2020年8期
So Yeon Yoon, Gyeong Sik Jeon, Dae Joong Kim, Department of Radiology, CHA Bundang Medical Center, College of Medicine, CHA University, Seongnam-si 13496, Gyeonggi-do,South Korea
Shin Jae Lee, Department of Radiology, Research Institute of Radiological Science, Yongin Severance Hospital, Yonsei University College of Medicine, Yongin-si 17046, South Korea
Chang Il Kwon, Department of Internal Medicine, Digestive Disease Center, CHA Bundang Medical Center, College of Medicine, CHA University, Seongnam-si 13496, Gyeonggi-do,South Korea
Mi Hyun Park, Department of Radiology, Dankook University Hospital, Chungcheongnam-do 31116, South Korea
Abstract
BACKGROUND
Pancreatic arteriovenous malformation (AVM) is a rare disease with a number of different reported treatment methods, but there are as yet no established or definite treatments for the disease.
CASE SUMMARY
A 43-year-old man visited the hospital due to periumbilical pain. The patient underwent imaging study and laboratory testing for evaluation of cause.Pancreatic AVM associated with pancreatitis was suspected on computed tomography and magnetic resonance imaging. The patient was diagnosed with pancreatic AVM with pancreatitis on imaging study and angiography.Transcatheter arterial embolization with various embolic materials was performed. Follow-up computed tomography scan revealed progressive regression of AVM and improvement of pancreatitis. At two-year follow-up, the patient showed no recurrence of symptom or pancreatitis.
CONCLUSION
Transcatheter arterial embolization can be considered an effective treatment modality for selective cases of pancreatic AVM.
Key words: Pancreas; Arteriovenous malformation; Pancreatitis; Pancreatic pseudocyst;Embolization; Therapeutic; Case report
INTRODUCTION
Pancreatic arteriovenous malformation (AVM) is a rare disease. Since its first report by Halpernet al[1]in 1968, the number of AVM cases has increased due to development of imaging modalities. However, only fewer than 100 cases have been reported[2]. Symptoms of AVM are variable; gastrointestinal bleeding and abdominal pain have been commonly reported, while duodenal ulcer and pancreatitis are less common. In fact, sometimes AVM is incidentally found without specific symptoms.
Owing to the uncommon nature of this disease entity, researchers have not yet established definitive treatments. Surgery is the mainstay of treatment[3,4], but researchers have reported on other treatment modalities such as conservative treatment and radiation therapy[4,5]. Transcatheter arterial embolization (TAE) is a minimally invasive treatment for many disease entities, and it is also used preoperatively to reduce blood loss in major surgery. In some cases, TAE is performed for treating pancreatic AVM[2,6,7], but it has only been performed for selective cases.Herein we report a case of pancreatic AVM accompanied by pancreatitis that was successfully treated with TAE.
CASE PRESENTATION
Chief complaints
A 43-year-old man visited the emergency department (ED) due to periumbilical pain and numeric rating scale of 4 points, both subjective. The patient’s symptoms had worsened over the two days prior.
History of present illness
At the patient’s first visit to the ED because of periumbilical pain, he underwent contrast-enhanced computed tomography (CT) scan. After conservative treatment, his symptoms improved, and he was discharged. One week later, he was having recurrent episodes of periumbilical pain, so he underwent magnetic resonance imaging (MRI) at the outpatient clinic of the digestive internal medicine department.One month later, the patient revisited the ED with severe periumbilical pain that had worsened from the previous day.
History of past illness
The patient was a healthy person without any underlying disease.
Personal and family history
The patient had no family history.
Physical examination
On the patient’s first and second visits to the ED, his vital signs were within normal range. He had no abdominal tenderness or rebound tenderness on physical examination.
Laboratory examinations
On the patient’s first visit to the ED, his laboratory test findings were within normal range. On his second visit, his laboratory test results confirmed pancreatitis as follows: Elevated amylase and lipase (120 U/L and 83 U/L), C-reactive protein (CRP,5.73 mg/dL), lactate dehydrogenase (285 U/L), D-dimer (2074.59 ng/mL), and erythrocyte sedimentation rate (62 mm/hr).
Imaging examinations
An initial contrast-enhanced CT scan revealed clustered dilated vessels in the pancreas body and tail with small pseudocyst. Twelve days later, the patient underwent pancreatic MRI that showed multifocal tortuous arterial enhancing lesions at the mid to distal body of the pancreas with mild atrophy and pseudocyst. The possibility of pancreas AVM was suggested.
One month later, the patient underwent a repeated CT scan because of symptom recurrence, and the scan (Figure 1) showed findings of AVM accompanied by acute pancreatitis, multifocal vascular structures, and pseudocyst in the pancreas body and tail.
Further diagnostic work-up
Tumor markers were within the normal range. Before any intervention, the patient underwent follow-up laboratory tests. In the results, leukocytosis was newly noted,and CRP (30.04 mg/dL) was further elevated. Amylase and lipase (66 U/L and 64 U/L) were slightly lower.
TREATMENT
For diagnosis and initial treatment, angiography and embolization were planned.Celiac trunk angiogram was performed, and there was abnormal staining in the left upper abdomen. There were numerous fine feeders mainly originating from the left gastric, splenic, and dorsal pancreatic arteries as well as early portal vein opacification. These findings confirmed pancreatic AVM (Figure 2).
Each feeding artery and the left gastric, splenic, and dorsal pancreatic arteries were selected using microcatheter. Distal portions of these arteries were not supplied for AVM; therefore, coil embolization was performed to protect the distal branch.Microcoils, gelatin sponges (gelfoam), and n-butyl-2-cyanoacrylate (histoacryl glue)were used as embolic materials. During catheterization of the dorsal pancreatic artery originating from the celiac trunk, focal dissection of celiac trunk occurred. The distal portion of the dorsal pancreatic artery had communicated with the left colic branch of the inferior mesenteric artery, and thus, catheterization was doneviainferior mesenteric artery.
OUTCOME AND FOLLOW-UP
Amylase and lipase levels were the highest on day 6 post-embolization, and CRP level was the highest on day 3. The patient underwent follow-up CT after one week that showed slight improvement of peripancreatic inflammation and small AVM remaining. No dissection of the celiac trunk was identified. The patient’s abdominal pain was relieved, and he was discharged uneventfully on day 9 post-embolization.
At three-month follow-up, there was no recurrent abdominal pain, and laboratory findings were all within normal ranges. Minimal AVM was still suspected even though the enhancing lesions on the pancreas had almost disappeared on CT scan;however, previously noted peripancreatic infiltration and fluid collection had disappeared. One year after embolization, CT scan (Figure 3) showed regression of most vascular networks except for a few small residual vessels in the pancreas proximal body, and there was no evidence of pancreatitis. There was no recurrence during the two-year follow-up period; the patient was symptom free for 15 mo.
DISCUSSION
Pancreatic AVM has various presentations, and in fact, it is sometimes asymptomatic and only found on image study. Investigators have identified gastrointestinal bleeding, abdominal pain without or with pancreatitis as in our case, portal hypertension possibly, and, rarely, pseudoaneurysm resulting from eroding peripancreatic vessels (splenic or gastroduodenal arteries,etc.)[8,9]as well as pancreatic AVM associated portal vein thrombosis[3]. There is not yet an established treatment of choice for AVM. Previous researchers have reported on medical treatment, radiation therapy, surgery, and embolization, and complete resection has been thought to be the ultimate treatment. However, pancreatectomy for AVM has a risk of massive bleeding, and in addition to the invasiveness of the procedure, it can also cause diabetes.
TAE is possibly indicated for selective cases, for instance for patients who have a single feeding artery, who are at high surgical risk, and/or who have no hemorrhage[10]. In our patient’s case, the manifestation was pancreatitis. Although pancreatitis can cause pancreatic AVM[11], our patient did not have history of alcoholic consumption, gallstone, or previous pancreatitis. The exact correlation between pancreatic AVM and pancreatitis has been unknown, but it is highly likely that AVM causes pancreatitis. Therefore, less invasive embolization was planned for our patient.
In our case, there were three large feeders, and it was not possible to embolize all fine feeders excluding these three; as a result, we could not completely exclude pancreatic AVM even after embolization. However, the patient’s pancreatitis had improved completely in follow-up study. Even when embolization is not complete, as in our case, researchers have reported progressive regression of AVM and no symptom recurrence[6,7]. The difference between our case and cases in previous studies was that we used variable embolic materials whereas previous researchers used liquid embolic agent (N-butyl-2-cyanoacrylate)[6,7]. There are several reports about different embolic materials for AVM embolization such as coils, particles, n-butylcyanoacrylate, and ethylene vinyl alcohol copolymer (Onyx)[2,6,12]. However,researchers have not yet established the most suitable embolic materials because there have been so few reports. Further long-term follow-up is needed to establish a clinical course for remnant AVM. In addition to the possibility of incomplete embolization of all feeders, duodenal ulcer can occur following TAE, and additional surgery is needed in recurrent cases[2].
CONCLUSION
Despite the above mentioned limitations of embolization, TAE can be considered a safe and effective treatment for selective cases of pancreatic AVM.
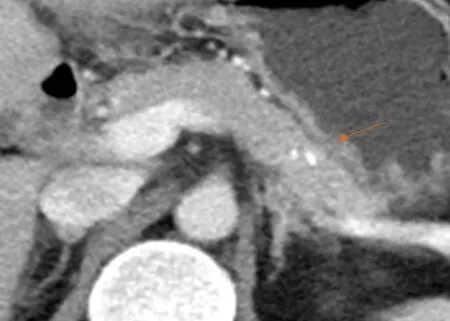
Figure 3 One-year follow-up contrast enhanced computed tomography scan. Computed tomography scan shows regression of most vascular networks except for a few small residual vessels in the pancreas proximal body. There was no evidence of pancreatitis. A high-density spot (orange arrow) in the pancreas was embolic agent (histoacryl glue).
 World Journal of Clinical Cases2020年8期
World Journal of Clinical Cases2020年8期
- World Journal of Clinical Cases的其它文章
- Clinicopathological differences and correlations between right and left colon cancer
- Bedside score predicting retained common bile duct stone in acute biliary pancreatitis
- Stability and infectivity of coronaviruses in inanimate environments
- Status, challenges, and future prospects of stem cell therapy in pelvic floor disorders
- Unusual presentation of congenital radioulnar synostosis with osteoporosis, fragility fracture and nonunion: A case report and review of literature
- Predictive factors for central lymph node metastases in papillary thyroid microcarcinoma