Unusual presentation of congenital radioulnar synostosis with osteoporosis, fragility fracture and nonunion: A case report and review of literature
2020-05-14 01:54:04
World Journal of Clinical Cases 2020年8期
Zhan-Yu Yang, Jiang-Dong Ni, Ze Long, Le-Tian Kuang, Shi-Bin Tao, Department of Orthopedics,The Second Xiangya Hospital, Central South University, Changsha 410000, Hunan Province,China
Abstract
BACKGROUND
Congenital radioulnar synostosis (CRUS) is a rare deformity of the upper extremity. It is characterized by loss of rotation of the involved forearm and functional limitations in daily activities. No studies on CRUS with osteoporosis have been reported to date, and osteoporosis is usually recognized as an important dimension of genetic disorder in children. We discuss the possible relationship among this disorder, osteoporosis and fracture nonunion, investigate the strict surgical indications and recommended treatments.
CASE SUMMARY
A 14-year-old male patient with bilateral CRUS with osteoporosis, fragility fracture and nonunion of fractures in ulna and radius presented our institution for further treatment, complaining of limitation in rotation. The bone mineral density of the hip and lumbar spine was 0.687 g/cm2 and 0.705 g/cm2,respectively, and the Z-score for both was -2.1, which revealed osteoporosis and a high risk of fracture. Tow serum bone turnover markers indicated an imbalance of bone metabolism. Reoperation for ulna fracture with autogenous bone grafting and a postoperative physiotherapy program were adopted rather than the separation of pathological synostosis. Radiological examination, observational posture assessment and limb function scale were evaluated before and 1 year after surgery. At 1 year, the fracture nonunion had almost recovered, forearm movement function on the fracture side was restored, and function on the healthy side was significantly improved compared with that before rehabilitation.
CONCLUSION
Surgical indications for CRUS vary from person to person. Surgery should not be the first choice of treatment, and physiotherapy is not inferior to surgical treatment.
Key words: Congenital radioulnar synostosis; Surgical indication; Osteoporosis; Fragility fracture; Nonunion; Case report
INTRODUCTION
Congenital radioulnar synostosis (CRUS), which is caused by fusion between the proximal end of the radius and ulna with the forearm fixed in some degrees of pronation, is a rare deformity of the upper extremity. It is common, however, in congenital elbow anomalies, and approximately 60%-80% of cases are bilateral[1-3]. It is characterized by loss of rotation of the involved forearm and a variety of functional limitations in daily activities in severe cases, presumably as a result of an insultin uteroat the time when the proximal ends of the radius and ulna were connected by a common perichondrium[4,5]. The etiology has been reported to be genetic and multifactorial[1]. Pain or restriction of elbow flexion-extension movements is absent in most patients with CRUS; their forearm is usually fixed in the pronation, and the function of supination is lost to varying degrees[1,6]. In most cases, the evaluation of the malformation is based on the classification by Cleary and Omer[7,8]. It is classified into four radiographic types, as shown in Table 1[9].
No studies on CRUS with osteoporosis have been reported to date, but osteoporosis is usually recognized as an important dimension of genetic disorder in children.Childhood osteoporosis is typically divided into primary and secondary causes, with osteogenesis imperfecta (OI) representing the prototypical primary osteoporosis of childhood, predisposing to bone fragility and fracture[10-13]. Low-trauma non-vertebral fractures in children with osteoporosis are observed most frequently at the femur,tibia, forearm, humerus, feet and ankles[14-16].
We here report a 14-year-old male patient with bilateral CRUS with osteoporosis,fragility fracture and nonunion of fracture in ulna and radius. Informed consent was obtained from the patient and his guardians for using the data of this case to be submitted for publication.
CASE PRESENTATION
Chief complaints
A 14-year-old right-handed boy with CRUS of the bilateral forearm and a fragility fracture of both bones of the forearm in a fall presented to the Department of Orthopedics of our hospital.
History of present illness
In another hospital, open reduction and internal fixation were performed, while the ulna was fixed with a Kirschner wire, maintaining neutral forearm position in a plaster cast for 8 wk before rehabilitation was initiated. At 3 mo after surgery, since the location of the reduced ulna was lost and the fracture was nonunion, the patient came to our hospital and asked for further treatment.

Table 1 Cleary and Omer classification of congenital proximal radioulnar synostosis
History of past illness
The boy had two previous fractures, including one distal radius fracture and one tibiofibular fracture.
Personal and family history
There was a possible hereditary history in his family, where his mother and younger brother had a similar elbow deformity.
Physical examination upon admission
On physical examination, a hard but painless lump was found in the posterolateral region of the bilateral elbow, and it could not be reduced in flexion-extension or in pronation-supination. A deficiency in active motion was present at the left forearm(Figure 1). Right forearm function was slightly limited for the compensation of the ipsilateral shoulder, and the patient had no flexion and extension dysfunction on both sides of the forearm.
Laboratory examinations
Bone mineral density (BMD) was measured by Dual Energy X-ray Absorptiometry.BMD of the hip and lumbar spine was 0.687 g/cm2and 0.705 g/cm2, respectively, and the Z-score for both was -2.1. The 2013 International Society for Clinical Densitometry recommended a BMD Z-score threshold (?2.0 or worse) in children to denote childhood osteoporosis, provided such children also have a clinically significant fracture history, defined as ≥ 2 long bone fractures by age 10 and ≥ 3 long bone fractures by age 18[17]. According to the recommendation, the patient was identified as childhood osteoporosis with an increased fracture risk. Serum collagen type I crosslinked C-telopeptide (a marker of bone resorption) and serum procollagen I N-terminal propeptide (a marker of bone formation) of the patient were 1832 ng/mL and 347 ng/mL, respectively. These two bone turnover markers are recommended by the International Osteoporosis Foundation and the International Federation of Clinical Chemistry and Laboratory Medicine for the assessment of bone health[18].
Imaging examinations
Plain radiography showed a fracture of both bones of the left forearm and pathologic fusions between the proximal diaphysis of radius and ulna, with a small bone diameter (Figure 2).
FINAL DIAGNOSIS
Bilateral CRUS with osteoporosis, fragility fracture and nonunion of fractures in ulna and radius.
TREATMENT
Bilateral synostoses of this case were both classified as type II according to Cleary and Omer. Considering that the child’s forearm function of the dominant side was not significantly affected with the compensation of the ipsilateral limb and could ensure necessary living requirements, reoperation for ulna fracture with autogenous bone grafting and a postoperative physiotherapy program were adopted rather than the separation of pathological synostosis. Physiotherapy was performed by a professional rehabilitation physician, and all exercises were practiced bilaterally. These exercises consisted of actively stretching the muscle to the point of limitation of supination,followed by a passive supination movement, and then practicing compensatory movement of adjacent joints.
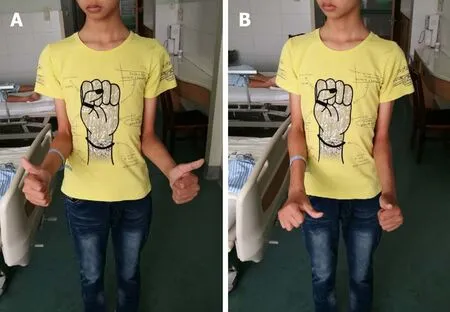
Figure 1 Active motion of the left forearm was limited. In order to reduce the rotation error caused by the compensation of elbow motion, the elbow joint was tightly attached to the waist. A: Supination; B: Pronation.
OUTCOME AND FOLLOW-UP
The patient was evaluated before and 1 year after surgery with radiological examination, observational posture assessment, the Activities of Daily Living Scale,the Liverpool Elbow Score, the Disabilities of the Arm, Shoulder, and Hand score and the Failla classification system. The Activities of Daily Living Scale was used to evaluate subjectively the degree of improvement in activities of daily living, including 11 that related to hygiene and self-care, eight that related to feeding, and seven that assessed environmental interaction on a 5-point scale. The Liverpool Elbow Score was first introduced in 2004 as an elbow-specific outcome score to be completed by both the clinicians and patients, combining a nine-item patient-answered questionnaire and a six-item clinical assessment score[19]. The Disabilities of the Arm, Shoulder, and Hand score is a 30-item questionnaire that quantifies physical function and symptoms in persons with any or multiple musculoskeletal disorders of the upper limb[20]. The Failla classification system is a grading system used by Faillaet al[21]to evaluate the functional ranges of rotation of the forearm. The evaluation results are given in Table 2. One year later, the fracture had almost recovered (Figure 3), and the range of motion was significantly improved (Figure 4).
DISCUSSION
The forearm complex functions to rotate the hand in space and allow for a redistribution of forces during functional tasks. Disruptions of any one of the components can potentially lead to limitations in forearm rotation and function[22].CRUS as a rare malformation is thought to be an anomaly of longitudinal segmentation that develops in the early fetal life. The elbow begins to appear at day 34-35 of fetal life, while the humerus, radial bone and ulna appear at day 37[7]. The humerus, radius and ulna are continuous with each other and are joined by a common perichondrium within the first 60 d of embryologic development. The cartilaginous anlage between these bones is separated by condensation, while the forearm is in a neutral position. Deformity of the radial head may be closely related to complete proximal union caused by early interference with joint formation[23]or unequal growth of the radius head caused by limited distal epiphyseal fusion[24].
CRUS is usually bilateral and subject to autosomal dominant inheritance[25].Moreover, CRUS is one of many components of malformation syndromes in children with chromosomal aberrations[8,26]. A number of authors have claimed that there is a genetic basis for radioulnar synostosis. Evidence for this etiology, like in this case,includes familial occurrence and the close relation with other congenital syndromes such as acrocephalosyndactyly, microcephaly, Apert's syndrome, Carpenter's syndrome, arthrogryposis, Klinefelter syndrome, multiple exostoses, Holt-Oram syndrome, fetal alcohol syndrome, Ayme-Gripp syndrome, Saethre-Chotzen syndrome, mandibulofacial dysostosis with microcephaly and William's syndrome[2,27-30].

Figure 2 Plain radiographs of the bilateral forearm at 3 mo after surgery. A, B: Left side with loss of reduced location; C, D: Right side with the same deformity of radioulnar synostosis.
Because children can easily compensate for rotational limitations caused by joint deformities, the disease is usually not diagnosed early[31]. Although the pronation and supination movements of forearm are limited, elbow flexion and extension exercises are generally unaffected. Most patients with CRUS can manage daily activities through the overuse and compensation of shoulder and wrist[6,32]. Shoulder abduction compensates for inadequate pronation, and shoulder adduction compensates for inadequate supination[33].
Our patient had type II bilateral synostoses, according to the Cleary and Omer classification, and had an accessory bone in the proximal part of his bilateral forearm wedged between the radius and ulna. In addition, there was a fracture with slender long bones and thin cortex after a low-energy injury. Laboratory examination also revealed the presence of osteoporosis as compared with peers. The only available method to determine the pathogenesis with certainty is to measure directly bone formation and resorption on trabecular surfacesviatransiliac bone biopsy. However,the patient refused this procedure because of the potential risks. We hypothesize that patients with CRUS may have OI or calcification disorder due to genetic defects.Therefore, for such patients with fractures, in addition to strong internal fixation, bone grafting or stimulation of osteogenesis may have more benefits than expected.
Many studies have examined different surgical methods for CRUS, such as derotational osteotomy of radial shaft, radial head excision and graft applications (see Table 3 for details). As CRUS is rare, it is difficult to conduct randomized-controlled trials, and there are generally only case reports or case series in the literature. Surgical techniques for treating radioulnar synostosis can be categorized into two groups: (1)Operations that improve pro-supination through synostosis resection, with or without interposition of biological or synthetic materials; and (2) Operations that improve the forearm’s fixed position[34]. Surgery is performed with the intention of restoring normal anatomical alignment, thus preserving normal forearm biomechanics.However, some studies have shown a high incidence of postoperative complications[35-37]. It is almost impossible to restore the complete rotation of theaffected forearm, and although the initial results might be satisfactory, the range of motion would return to the preoperative status over time[37,38]. Satisfactory results were usually achieved in patients with very severe preoperative disability[31,39-42].
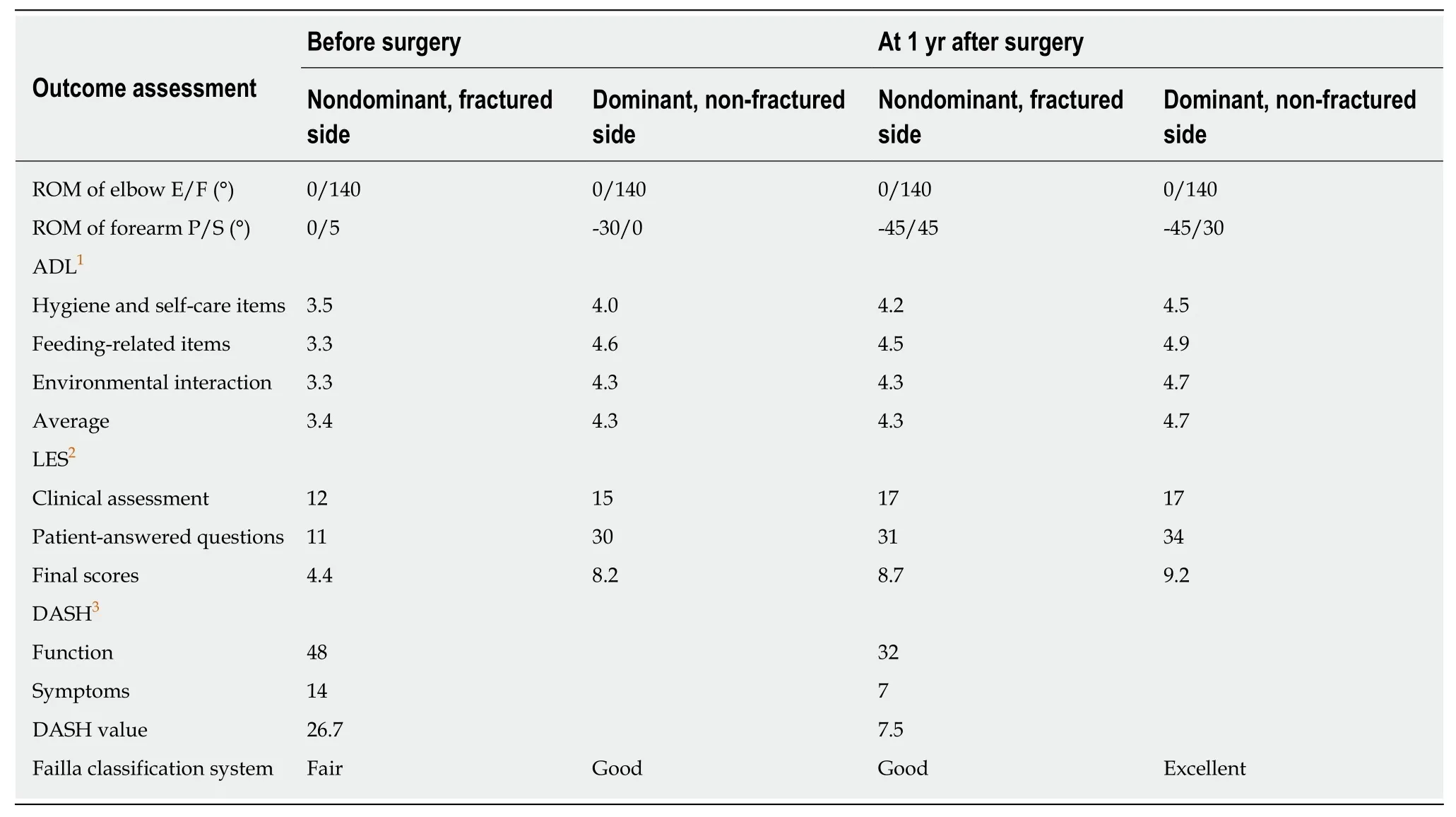
Table 2 The evaluation results before and after surgery
Although an indication for operation in a patient with more than 60 degrees of fixed pronation was proposed, it must be individualized in patients with pronation between 15 and 60 degrees[43]. The patients with > 60 degrees of pronation usually have restrictions in daily activities[44]. Generally, the surgical protocol is dependent more on functional deficits than absolute forearm position. Studies have shown that physiotherapy is effective in the functional recovery of the upper extremities in patients with CRUS[45].
In the present case, forearm rotation function was compensated well through the adjusted movements of the adjacent joints, wrists and shoulders, and there was no obvious limitation in daily life. Therefore, we suggest that the choice of procedure should be individualized as not all the patients are eligible for surgery.
CONCLUSION
In summary, based on a review of all similar reported cases, we believe that patients with CRUS complicated with osteoporosis and fracture, due to the suspicious geneinduced OI or calcification disorder, may benefit not only from indispensable firm internal fixation but also bone grafting or stimulus of osteogenesis. In addition,surgical indications in such patients vary from person to person. Surgery should not be the first choice except for those with severe limitations in daily activities, and physiotherapy may be a new method of functional rehabilitation. However, these are just conjectures obtained from a common case, and more research is needed to confirm these predictions in the future.

Table 3 Different surgical methods used in the treatment of congenital radioulnar synostosis

Figure 3 Plain radiographs showing the formation of callus, the disappearance of fracture line and the healing of fracture. A: At 2 mo after surgery; B: At 1 yr after surgery.
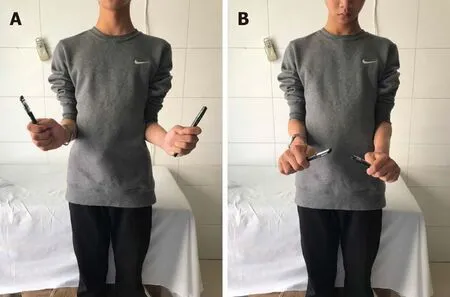
Figure 4 The range of motion of the left forearm was restored to the pre-injury state and was significantly improved after operation. A: Supination; B:Pronation.
 World Journal of Clinical Cases2020年8期
World Journal of Clinical Cases2020年8期
- World Journal of Clinical Cases的其它文章
- Clinicopathological differences and correlations between right and left colon cancer
- Bedside score predicting retained common bile duct stone in acute biliary pancreatitis
- Stability and infectivity of coronaviruses in inanimate environments
- Status, challenges, and future prospects of stem cell therapy in pelvic floor disorders
- Predictive factors for central lymph node metastases in papillary thyroid microcarcinoma
- Suicide attempt using potassium tablets for congenital chloride diarrhea: A case report