Hyoid-complex elevation and stimulation technique restores swallowing function in patients with lateral medullary syndrome:Two case reports
2020-04-25 05:00:46YuErJiangQianQianLyuFengLinXueTingYouZhongLiJiang
World Journal of Clinical Cases 2020年5期
Yu-Er Jiang,Qian-Qian Lyu,Feng Lin,Xue-Ting You,Zhong-Li Jiang
Yu-Er Jiang,Qian-Qian Lyu,Feng Lin,Xue-Ting You,Zhong-Li Jiang,Department of Rehabilitation Medicine,Sir Run Run Hospital,Nanjing Medical University,Nanjing 211100,Jiangsu Province,China
Yu-Er Jiang,Qian-Qian Lyu,Feng Lin,Xue-Ting You,Zhong-Li Jiang,Department of Rehabilitation Medicine,The First Affiliated Hospital of Nanjing Medical University,Nanjing 210029,Jiangsu Province,China
Abstract
BACKGROUND
A swallowing disorder may occur following a brainstem stroke,especially one that occurs in the swallowing centers.Lateral medullary syndrome(referred to as LMS),a rare condition in which a vascular event occurs in the territory of the posterior inferior cerebellar artery or the vertebral artery,has been reported to lead to more severe and longer lasting dysphagia.
CASE SUMMARY
We report two patients with dysphagia due to LMS and propose a novel technique named hyoid-complex elevation and stimulation technique(known as HEST).The two patients had no other functional incapacity back into life,but nasogastric feeding was the only possible way for nutrition because of severe aspirations.Swallowing function was evaluated by functional oral intake scale,modified water swallow test,surface electromyographic signal associated with video fluorography swallowing study to assess the situation of aspiration,pharyngeal residue,pharyngeal peristalsis,upper esophageal opening and the ability of deglutition.Both patients were treated with the HEST method for dysphagia and recovered quickly.
CONCLUSION
HEST is effective for shortening the in-hospital time and improving the quality of life for patients with dysphagia who suffer from LMS and likely other strokes.
Key words:Lateral medullary syndrome;Hyoid-complex elevation and stimulation technique;Upper esophageal sphincter;Dysphagia;Treatment;Case report
INTRODUCTION
A swallowing disorder(dysphagia) may occur following a brainstem stroke,especially one that occurs in the swallowing centers in the posterior and lateral regions of the medulla oblongata.Lateral medullary syndrome(LMS),also known as Wallenberg syndrome,is a rare condition in which a vascular event occurs in the territory of the posterior inferior cerebellar artery or the vertebral artery[1]and reportedly leads to severe and long-lasting dysphagia[2]due to the absence of the swallowing reflex,extension of swallowing latency,dysfunction of the upper esophageal sphincter(UES) opening,and pharyngeal constriction.Nasogastric feeding has been the only possible method for obtaining nutrition because of severe aspiration.For patients with LMS,swallowing training is an indispensable treatment,and recovery of swallowing occurs with the restoration of pharyngeal function[3].
Here,we report two cases of patients with LMS who had restored swallowing function in a short period of time by using a hyoid-complex(the hyoid bone with pedunculus or epiglottidean complex tissues) elevation and stimulation technique(HEST).The operation procedure of this technique was as follows(Figure 1).First,a balloon catheter was inserted through the mouth to the edge of the UES,and the balloon was inflated by water when it was located at the lower edge of the cricoid cartilage and the UES.Then the balloon was lifted up at the same time as the hyoidcomplex.Finally,patients were asked to swallow hard while the suprahyoid muscles were facilitated by electrical stimulation with a stimulus intensity dependent on the measured surface myoelectricity results.When an effective swallow was completed,the inflated balloon was very easy to remove.Aside from dysphagia due to lateral medullary infarction,neither patient with LMS had other functional incapacities in daily life.
CASE PRESENTATION
Chief complaints
Case 1:A 58-year-old male with LMS was admitted to the hospital with a chief complaint of “aphagosis for 20 d accompanying salivation and emaciation”.
Case 2:A 72-year-old male with LMS was admitted to the hospital with a chief complaint of “dysphagia for 24 d”.
History of present illness and past illness
Case 1:The patient had lost approximately 3 kg over the past 20 d and exhibited nutritional deficiency caused by dysphagia.
Case 2:The patient had lost approximately 5 kg over the past 24 d and exhibited nutritional deficiency caused by dysphagia.
History of past illness
Case 1:The patient was diagnosed with diabetes at the age of 48.His family members were all healthy.
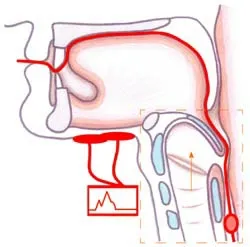
Figure 1 Placement of electrical stimulation and balloon dilatation in the hyoid-complex elevation and stimulation technique.
Case 2:The patient had suffered from hypertension for over 10 years and from diabetes for over 5 years.His family members were all healthy.
Examinations
Case 1:An absent gag reflex,dystaxia in the left arm and leg,and decreased pain and temperature sensations in the right side of body were noted.Magnetic resonance imaging showed a left lateral medullary infarction(Figure 2A).The final diagnosis of the presented case was LMS.In the very beginning,the patient was unable to initiate a swallowing motion due to the absence of a swallowing reflex.The result of functional oral intake scale(FOIS) was performed at 20 d after the onset of stroke was level 1(nothing by mouth),and the result of the modified water swallow test(MWST)was grade 1(dysphagia with bucking,a wet voice and palatal paresis).On the 4thd after hospitalization,the surface electromyography(sEMG) signals of the suprahyoid muscles were recorded when the patient was asked to try to swallow,in which an imperfect swallowing motion and delayed pharyngeal transit time could also be observed(Figure 3A).A video fluorography swallowing study(VFSS) was examined on the 5thd after hospitalization,which showed leakage or aspiration,pharyngeal residue,incomplete epiglottic closure and UES dysfunction(Figure 4A).In addition,the fiberoptic endoscopic evaluation of swallowing examination(FEES) demonstrated epiglottis insufficiencies(Figure 5).
Case 2:An absent gag reflex and decreased sensation on the left side of the body were found by physical examination.Magnetic resonance imaging showed a right lateral medullary infarction(Figure 2B).The final diagnosis of the presented case was LMS.The initial FOIS result was level 1(nothing by mouth).A VFSS was examined on the 19thd after the onset of the stroke,which showed leakage or aspiration,pharyngeal residue,decreased laryngeal elevation and impaired opening of the UES(Figure 4B).The result of the MWST performed on the 24thd after the onset of the stroke was grade 4(no bucking,no residue and 1 swallowing movement could be initiated).Imperfect swallowing waves were observed by sEMG,especially when swallowing occurred on the left side(Figure 3B).
FINAL DIAGNOSIS
The final diagnosis of the presented two cases was LMS.
TREATMENT
Case 1
During the patient's first week in the hospital,he received conventional treatment,including a behavioral approach and electrical stimulation.Swallowing function was not significantly improved.HEST was adopted in the second week and performed twice a day,5 d per wk.
Case 2
HEST was performed twice a day as well.
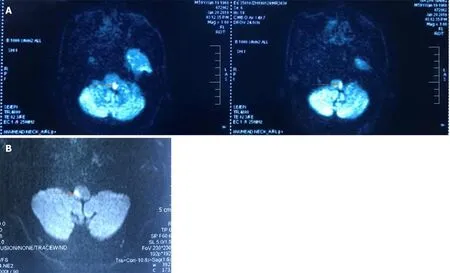
Figure 2 Magnetic resonance imaging of the head.
OUTCOME AND FOLLOW-UP
Case 1
After 2 wk of treatment,the patient was able to resume oral feeding,and the nasogastric tube was removed.The second examination showed that the FOIS result was improved to level 7(total oral diet with no restrictions) and the MWST result improved to grade 5(no bucking,no residue and at least 2 or more swallowing motions could be initiated),and the sEMG signals resembled normal swallowing.At each initial swallowing movement,the target value could be easily achieved,but the latency became longer in the second and subsequent movements(Figure 3C).After discharge,the patient was advised to continue endurance training for a long time.The long-term outcome was investigated 12 mo later over the telephone because the present address of the patient was quite far away from the hospital.The only possible evaluation was FOIS,which maintained level 7 and the nutrition way maintained oral feeding.The time required for each meal was limited in 30 min.
Case 2
On the third day after treatment,the patient was able to resume oral feeding,and the nasogastric tube was removed.The second examination showed that the FOIS result was level 7(total oral diet with no restrictions),and the MWST result was grade 5(no bucking,no residue and at least 2 or more swallowing movements could be initiated).Normal swallowing waves were observed by sEMG(Figure 3D).The follow-up was investigated 9 mo later over the telephone because the patient felt free to eat all kinds of foods and believed there was no need to be hospitalized.The FOIS of the patientmaintained level 7 as well.The nutrition way remained the same with each meal finished within 30 min.
The clinical treatment schedule of the two patients is shown in Table 1.
DISCUSSION
Traditional therapy for dysphagia involves exercises to strengthen the oropharyngeal musculatures,lifting and compensatory maneuvers to facilitate laryngeal elevation and closure,techniques to stimulate and strengthen the swallowing reflex and diet modifications[4].HEST therapy combines balloon techniques with electromyography-triggered electrical stimulation(ETS) patterns to reshape the physiological order of swallowing.The former technique was used to loosen the UES and elevate the hyoidcomplex,meanwhile the latter technique was used for myoelectric biofeedback training.First,a No.14 balloon catheter was gently inserted through the pharyngeal into the esophagus.If the patient did not cough and phonation was normal,3 ml of water was injected into the balloon,and then the catheter was pulled upward until resistance was encountered,indicating the balloon was positioned at the lowest edge of the UES[5].The plump balloon distracted the UES and lifted up when the sustaining resistance generated.Second,2 electrodes of ETS were placed on mylohyoid muscles in the submental region above the hyoid bone[6].ETS patterns were observed with the Guardian Aspire2[7],which incorporates neuromuscular electrical stimulation and surface electromyography biofeedback technology for measurement and treatment.The threshold value of the electrical stimulation was set in advance depending on the intensity to evoke the macroscopic contraction of mylohyoid muscles,which could be revealed by the movement of prominentia laryngea.In other words,ETS patterns were delivered to help accomplish the complete swallowing at the moment of every beginning.Hence,when the inflated balloon encountered resistance,the patients were instructed to swallow with effort,and ETS stimulation was simultaneously administered.A complete swallowing exercise was completed when the balloon could be pulled out with ease,which means the UES was loosen up and the hyoid-complex was elevated.This treatment was terminated when the patients reported restoration of full oral intake.
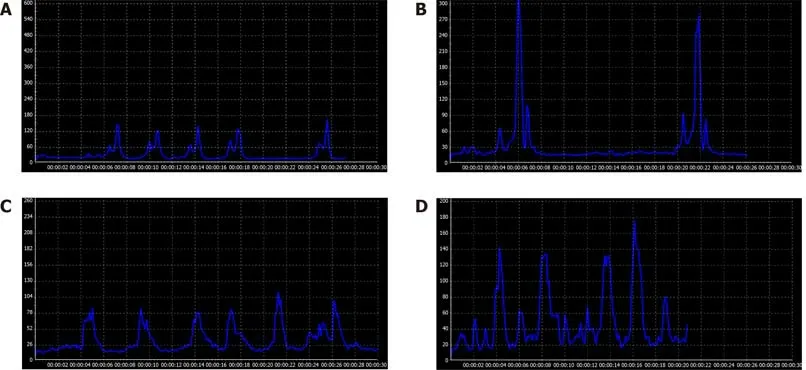
Figure 3 Surface electromyographic signal recording of two patients before and after hyoid-complex elevation and stimulation technique treatment.
Swallowing is a patterned sequence of motor activity coordinated by bilateral swallowing centers in the rostral dorsolateral medulla[8].The swallowing sequence involved with pharyngeal function followed seven steps[9]:(1) Laryngeal elevation;(2)Anterior hyoid motion;(3) Epiglottis movement;(4) Laryngeal closure;(5) Pharyngeal stripping wave;(6) Pharyngeal contraction;and(7) Pharyngoesophageal segment opening(Figure 6).Lateral medullary infarction impairs the sequence of swallowing events[10].The patients cannot initiate contraction of the suprahyoid muscles for complete swallowing,and thus,the movements of the pharynx and the root of the tongue are affected.Without enough pressure from the tongue base,the epiglottis loses the ability to sufficiently close.However,HEST helps elevate the hyoid-complex and opens the UES at the right time,which are the beginning and ending of the normal swallowing movements,respectively.To be specific,ETS stimulation and balloon lifting work together to upraise the hyoid bone with pedunculus and epiglottidean complex tissues,while the active swallowing along with the balloon dilation help loosen the UES.
Compared with isolated muscle strength exercises such as the Mendelson maneuver,Masako maneuver,and electrical stimulation,HEST can improve the strength of suprahyoid muscles and lift the hyoid bone as well.In addition,HEST solves the tricky problem of UES opening,which results in leaking or aspiration fromresidue.On the other hand,balloon dilatation is an effective approach for UES opening and pharyngeal contraction[11].However,patients with LMS require UES relaxation only during swallowing movements instead of plastic deformation[12,13].The use of balloon dilatation alone does not improve laryngeal elevation,epiglottic closure,or pharyngeal contraction,which are necessary for swallowing efficiency and safety.In contrast,HEST can help reestablish a normal swallowing mechanism that follow the appropriate steps and complete the integrated movement.
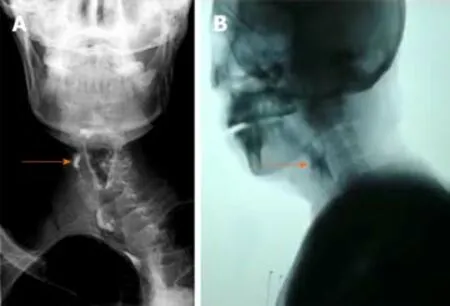
Figure 4 lnitial video fluorography swallowing study showing pharyngeal residue(see arrow).
CONCLUSION
We report two patients with dysphagia,who were treated with HEST technique and had restored swallowing function within a short time.Because this technique is effective,easy to operate,and safe,the possibility of a wider application of HEST is suggested to restore swallowing function in patients with oropharyngeal dysphagia.Further studies with a larger population are needed to clearly verify the underlying mechanisms.
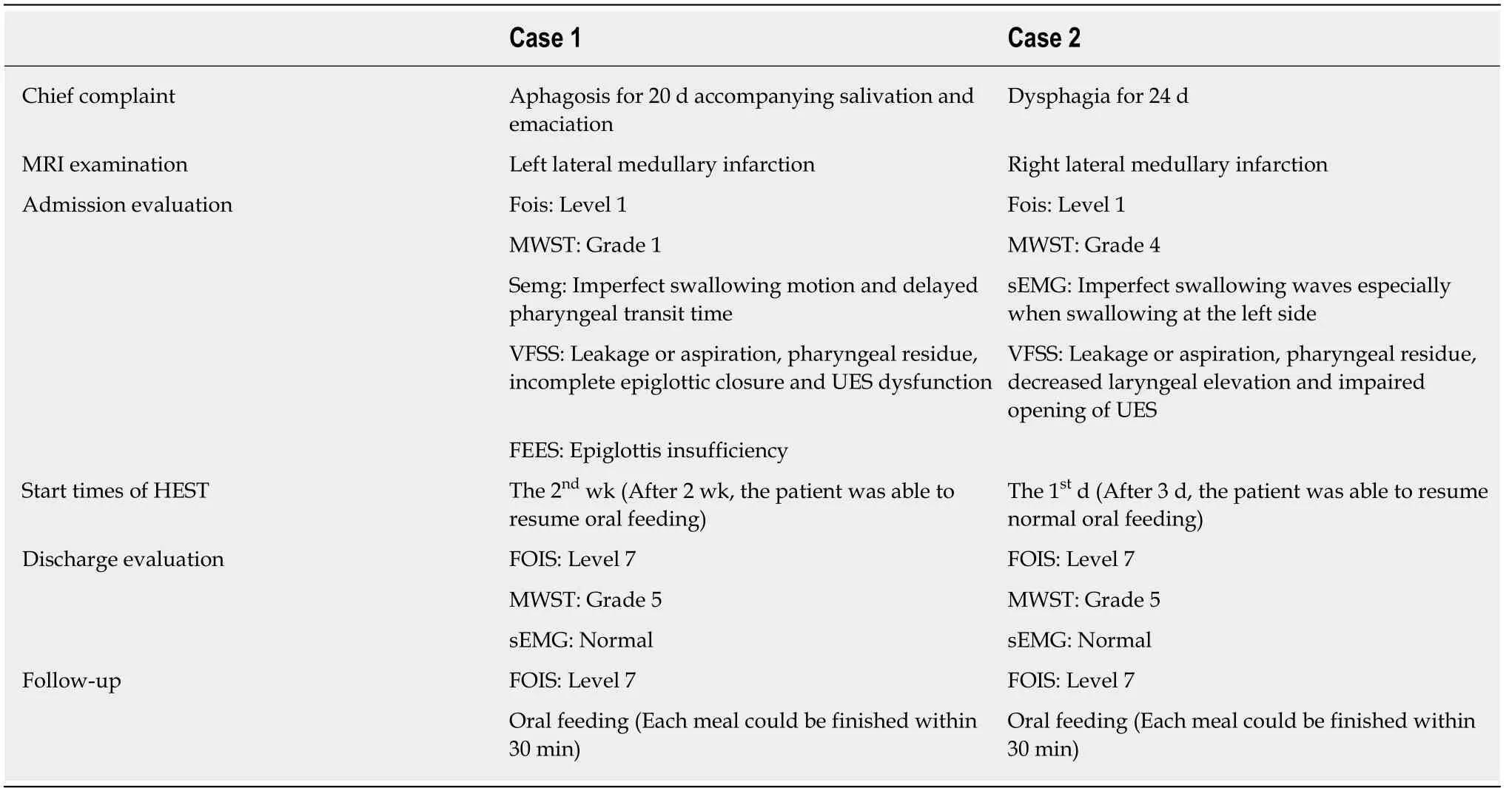
Table 1 Clinical course and treatment timeline
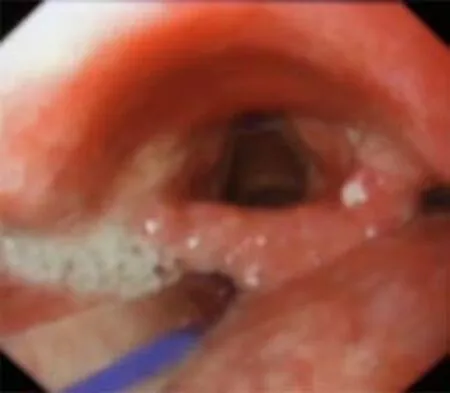
Figure 5 lnitial fiberoptic endoscopic evaluation of swallowing examination showing epiglottis insufficiency in Case 1.
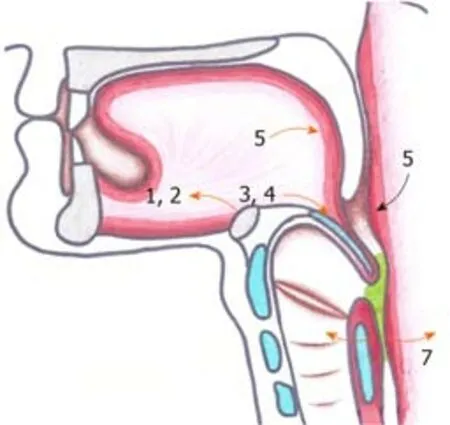
Figure 6 The swallowing sequence of pharyngeal movement.
ACKNOWLEDGEMENTS
The authors would like to thank the rehabilitation team at Sir Run Run Hospital fortheir collaboration and our patients.The patients were informed about,and consented to,publication of the case details.
 World Journal of Clinical Cases2020年5期
World Journal of Clinical Cases2020年5期
- World Journal of Clinical Cases的其它文章
- Laparoscopic repair of complete intrathoracic stomach with iron deficiency anemia: A case report
- Growth hormone therapy for children with KBG syndrome: A case report and review of literature
- Hepatoid adenocarcinoma of the stomach: Thirteen case reports and review of literature
- Cerebral venous sinus thrombosis following transsphenoidal surgery for craniopharyngioma: A case report
- Microscopic removal of type lll dens invaginatus and preparation of apical barrier with mineral trioxide aggregate in a maxillary lateral incisor: A case report and review of literature
- Metabolic and genetic assessments interpret unexplained aggressive pulmonary hypertension induced by methylmalonic acidemia: A case report