Use of omental patch and endoscopic closure technique as an alternative to surgery after endoscopic full thickness resection of gastric intestinal stromal tumors:A series of cases
2020-04-22 07:13:08AmitSachdevShahzadIqbalIgorBragaRibeiroDiogoTurianiHourneauxdeMoura
World Journal of Clinical Cases 2020年1期
Amit H Sachdev,Shahzad Iqbal,Igor Braga Ribeiro,Diogo Turiani Hourneaux de Moura
Amit H Sachdev,Diogo Turiani Hourneaux de Moura,Division of Gastroenterology,Hepatology and Endoscopy,Brigham and Women's Hospital,Harvard Medical School,Boston,MA 02115,United States
Shahzad Iqbal,Good Samaritan Hospital,NY 11795,United States
Igor Braga Ribeiro,Diogo Turiani Hourneaux de Moura,Gastrointestinal Endoscopy Unit,Hospital das Clínicas da Faculdade de Medicina da Universidade de S?o Paulo,S?o Paulo 05403-000,Brazil
Abstract
Key words: Gastric perforation;Gastrointestinal stromal tumors;Gastric tumor;Surgery;Endoscopy;Suturing
INTRODUCTION
Gastrointestinal stromal tumors (GISTs) originate from interstitial cells ofCajal.GISTs can occur anywhere along the GI tract but are most commonly found in the stomach(60%-70% of cases),occurring less frequently in the small intestine (20%-30%),colon and rectum (5%),and esophagus (4%)[1].Large lesions have traditionally been removed surgically.However,with recent innovations in advanced endoscopy,GISTs located in the stomach are now removed endoscopically[2].If the lesion is located deep in the muscularis propria,the en-bloc removal entails endoscopic full-thickness resection (EFTR).EFTR is limited by the size of the full-thickness defect created.The currently available methods for closing defects endoscopically include metallic clipping (+/- endoloop placement),closure using over-the-scope metal clips,and suturing.However,these closure methods may not be successful for large and hard to access defects especially when operating in the retroflexed position.Hence,such defects will need emergent surgical closure.Here we describe a new innovative endoscopic technique to close large and hard to access defects after EFTR of gastric GISTs.
CASE PRESENTATION
Case one
An 81-year-old female was found to have a 22 mm gastric fundus muscularis propria(layer IV) subepithelial lesion on endoscopic ultrasonography (EUS).EUS-fine needle aspiration was performed and pathology confirmed a GIST.The lesion was initially marked circumferentially by the tip of a Dual Knife electrocautery system (Olympus,Tokyo,Japan).Submucosal solution was injected.The overlying mucosa was incised.The lesion was identified,and removed by a combination of Dual and IT-2 knife electrocautery (Olympus,Tokyo,Japan).A large full-thickness defect was noted.Despite the use of CO2,capnoperitoneum was diagnosed and decompressed.Initial attempts at closure using endosuturing failed due to the slippage of sutures and Ttags.Attempts to close the defect using hemoclips and an endoloop were also unsuccessful.It was decided to pull omental fat into the gastric lumen and clip to the edges of the defect.Then,hemoclips along with endoloop placement (“tulip-bundle”technique) were used to close the defect (Figure 1).The patient did well postprocedure.Abdominal computed tomography (CT) was performed the next day,and extravasation of contrast was not observed.
Case two
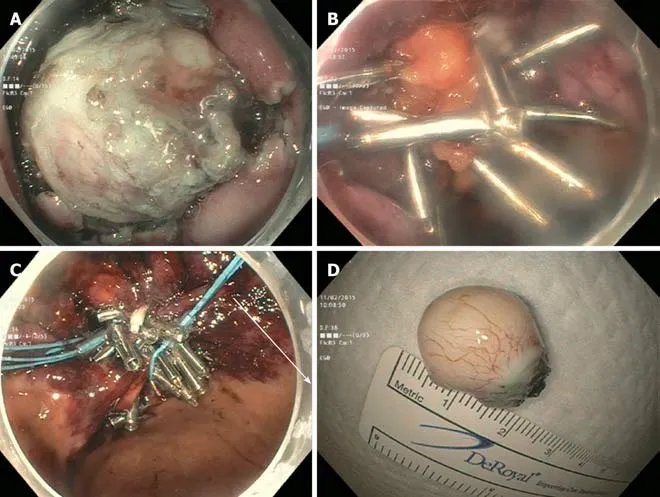
Figure1 Full thickness resection of a gastrointestinal stromal tumor.
The second case was a 79-year-old gentleman with a 28 mm gastric cardia muscularis propria GIST.The lesion was removed by EFTR.The resulting capnoperitoneum was decompressed.However,initial attempts at closing the large defect using an endosuture was only partially successful.Only the distal margin was closed.The proximal margin was difficult to visualize.Attempts at closure using hemoclips and an endoloop were unsuccessful.The omental fat was then pulled into the gastric lumen and clipped to the edges of the defect.Continuous endosutures were placed at four different areas in a purse-string fashion in the surrounding mucosa,and cinched leading to successful closure (Figure 2).A nasogastric tube was inserted,and attached to intermittent suction.No contrast extravasation was noted on abdominal CT the following day.The nasogastric tube was subsequently removed,and the patient was placed on a PO diet.
還有一則報道說,經過專家們的多年研究發現:晚睡晚起的人比早睡早起的人更長壽,他們甚至還舉出丘吉爾等名人的例子來佐證,說這些人都是“夜貓子”,習慣于白天睡覺、晚上工作,結果都活過了80多歲。對此,我們一些陰陽顛倒,晚上生龍活虎、白天卻萎靡不振的人可高興啦,這不,專家們也在這么說。
Case three
The third case was a 54-year-old gentlemen with a 35 mm gastric cardia muscularis propria GIST.The lesion was exophytic in location,and difficult to identify after incision of overlying mucosa.After identification with repeat EUS,the lesion was removed by a combination of IT-2 knife and snare polypectomy.The resulting capnoperitoneum was decompressed.The lesion was closed by the endoscopic omental patch technique as described in case two.
FINAL DIAGNOSIS
The three patients were diagnosed with muscularis propria GIST of the stomach.
TREATMENT
“Omental patching” was initially introduced in 1937 by Roscoe Reid Graham of Toronto to successfully close perforated duodenal ulcers.Generally,three or four fullthickness or seromuscular (as introduced by Lambert) sutures are placed perpendicularly between the edges of the perforation and are laid out on each side of the duodenum.A patch of omentum is then brought upward and the sutures are tied across[3].Here we describe omental patchingviaendoscopic techniques to close large and hard to access defects after EFTR of gastric GISTs.
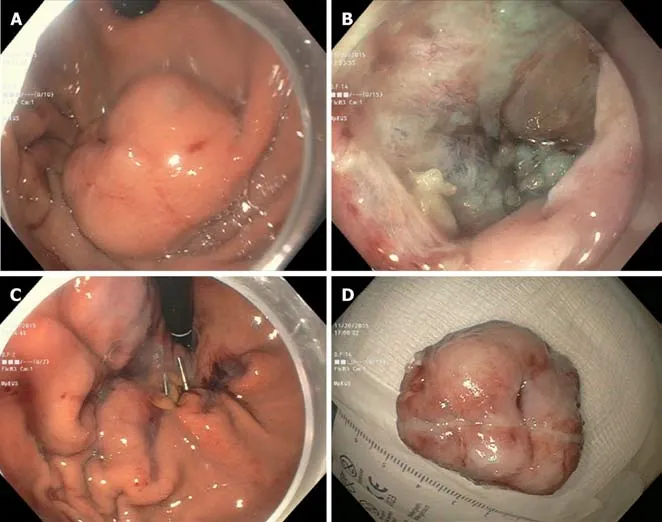
Figure2 Full thickness resection of a gastrointestinal stromal tumor.
In our practice,we have successfully used either hemoclipping along with endoloop placement (“tulip-bundle” technique) or endosuturing to close iatrogenic defects.However,when lesions are located in either the gastric fundus or cardia these closure methods do not always succeed.In the three cases presented,the proximal edges (especially) were difficult to access due to the large size of the defects.The omentum was noted nearby.It was pulled inside the gastric lumen,and clipped to the edges of the defect.In two cases,continuous endosutures in a purse-string fashion were placed at four different sites around the defect and cinched.In one case,when endosuturing was not available,we used hemoclips along with endoloop placement(“tulip-bundle” technique).The resulting capnoperitoneum was decompressed in all cases by passing a 10 mL syringe half-filled with sterile saline into the right upper quadrant of the abdomen under aseptic conditions.The plunger was removed to let the CO2 evacuate.Abdominal CT was performed one day post-procedure to rule out any contrast extravasation.Prophylactic antibiotics were given for 3-5 d.All procedures were performed under general anesthesia.
OUTCOME AND FOLLOW-UP
All lesions were successfully removed and iatrogenic defects were closed endoscopically.No post-procedure complications were noted.Post-procedure hospital length of stay ranged from 3-4 d.Histopathology examination showed GIST with complete R0 resection in all three cases.Pathology showed low-grade dysplasia,with the exception of case two which showed moderate grade dysplasia (with 6 per 50 HPF).No further surgical or oncological treatment was required.Patients were followed clinically in an outpatient setting with surveillance abdominal CT performed at 6 month intervals.The follow-up period ranged from 8-17 mo.No recurrence was noted (Table 1).
DISCUSSION
Traditionally,the majority of localized GISTs larger than 1 cm and involving the muscularis propria are managedviasurgical resection.The consensus guidelines dictate that all GISTs greater than or equal to 2 cm in size should be resected[1].Although a 2 cm cutoff is somewhat arbitrary,the most recent data indicates that this is appropriate[4].The goal of surgery is complete resection of the tumor,leaving the pseudocapsule intact and obtaining negative margins.However,with recent innovations in advanced endoscopy,it is feasible to offer patients a less invasive approach for removal of their tumors[5].

Table1 Patient characteristics
Endoscopic resection of GISTs has been reported;however,as the procedure is technically challenging and numerous obstacles may arise,the role of endoscopic resection is controversial.First,tumors may be difficult to access by endoscopy.Second,if a tumor is located deep in the muscularis propria,removal involves EFTR,which is technically challenging and is limited by the size of the defect created.Thus,it presents the inherent risk of positive margins.Furthermore,full-thickness resection imparts a risk of tumor spillage.Finally,the EFTR results in an iatrogenic perforation.Historically,iatrogenic GI perforations were referred for surgery.However,developments in advanced endoscopy have paved the way for novel endoscopic closure techniques[6-8].
To date,different techniques have been designed for the closure of GI defects.Certain therapeutic methods have been more thoroughly explored in iatrogenic colonic perforations[9-11].With the development of endoscopic mucosal resection and endoscopic submucosal dissection,iatrogenic perforations have been seen more frequently over the last 20-30 years;this has allowed endoscopists additional opportunities to perform endoscopic closure.
A retrospective study from Japan by Minamiet al[12]revealed that endoclips are an effective conservative closure method for perforation caused by endoscopic mucosal resection.Multiple studies have reported on the use of the over-the-scope clip technique to close perforations[13-16].All studies concluded that this technique is an effective endoluminal closure method;however,the studies in question only assessed method efficacy on relatively small defects.For closure of full-thickness defects,Stavropouloset al[17]described the effectiveness of endoscopic suturing in clinical practice using the OverStitch.One limitation of this procedure is that it must be performed with a double channel gastroscope,which limits flexibility.Thus,suturing in a location such as the gastric fundus is often challenging.
The previously-noted closure methods may not be successful for large or difficultto-access defects.Full-thickness resections will inherently leave a large defect.Hence,a novel technique for the closure of large and difficult-to-access defects caused by EFTR of GISTs located in the stomach was assessed in our series.Similar methods have been reported as early as 2001 in porcine models[18].Comparable techniques have also been attempted and described in case reports[19,20].While our report includes three cases,a larger sample size is needed to accurately assess the efficacy of this technique.If the closure of iatrogenic perforations with an omental patch using endoscopic techniques can be shown to be a reliable and reproducible procedure,it may become an attractive alternative to surgery,with the hope of reducing morbidity and mortality.
CONCLUSION
The omental plug closure technique may be used as an alternative to surgery in selected cases of gastric perforation.However,the technique requires the endoscopist to be experienced and proficient in endoscopic closure devices.
 World Journal of Clinical Cases2020年1期
World Journal of Clinical Cases2020年1期
- World Journal of Clinical Cases的其它文章
- Cluster headache as a manifestation of a stroke-like episode in a carrier of the MT-ND3 variant m.10158T>C
- Primary intestinal extranodal natural killer/T-cell lymphoma,nasal type:A case report
- Six families with balanced chromosome translocation associated with reproductive risks in Hainan Province:Case reports and review of the literature
- Clinical characteristics on manifestation and gene mutation of a transient neonatal cyanosis:A case report
- Sarcomatoid intrahepatic cholangiocarcinoma mimicking liver abscess:A case report
- Value of dynamic plasma cell-free DNA monitoring in septic shock syndrome:A case report