Changes in peak inspiratory f ow rate and peak airway pressure with endotracheal tube size during chest compression
2020-03-02 10:44:36JungWanKimJinWoongLeeSeungRyuJungSooParkInSoolYooYongChulChoHongJoonAhn
Jung Wan Kim, Jin Woong Lee, Seung Ryu, Jung Soo Park,2, InSool Yoo,2, Yong Chul Cho, Hong Joon Ahn
1 Department of Emergency Medicine, Chungnam National University Hospital, Jung-gu, Daejeon, Republic of Korea
2 Department of Emergency Medicine, College of Medicine, Chungnam National University, Jung-gu, Daejeon, Republic of Korea
KEY WORDS: Cardiopulmonary resuscitation; Intratracheal intubation; Airway pressure
INTRODUCTION
Adequate ventilation plays an important role in highquality cardiopulmonary resuscitation (CPR), but it is difficult to maintain proper ventilation during CPR.[1,2]Excessive ventilation leads to an increase in the intrathoracic pressure (ITP) that could decrease the survival rate by reducing venous return, cardiac output, and coronary perfusion pressure.[3-5]Studies[6-10]have reported various methods that prevent excessive ventilation such as capnography and tracheal pressure monitoring.However, the proper ventilation method and effectiveness of ventilation in early CPR remain debatable.[11,12]Among the various ventilation methods, endotracheal intubation(ETT) has the advantage of minimizing the interruptions during chest compressions, and it improves the return of spontaneous circulation (ROSC) and alleviates the reduction of coronary perfusion pressure.[13]Thus, it is recommended that an advanced airway is in place during CPR, if possible.[14]
In previous studies, a small-sized ETT increased airway resistance and the work of breathing during mechanical ventilation.[15-17]In experiments using pediatric ETTs, for smaller ETT size, there was greater difference in pressure between the proximal and distal portions of ETT than for larger ETT size.[18]However,most of these studies have been for pediatric ETTs, and no study has assessed the changes in f low rate and airway pressure with respect to ETT size during CPR.
This study aimed to measure the changes in peak inspiratory f low rate (PIFR), peak airway pressure (Ppeak),and mean airway pressure (Pmean) with respect to ETT size during CPR and identify the appropriate ETT size for adults.
METHODS
Simulation design and data collection
To observe the physiological changes with respect to ETT size during CPR, we used a CPR manikin (Resusci Anne Skill Reporter?, Laerdal, Stavanger, Norway).The lung compliance of the CPR manikin was set within the range of 0.025–0.03 L/cmH2O (Table 1), which was similar to the lung compliance measured in patients who had out-of-hospital cardiac arrests (OHCAs) (0.022 L/cmH2O).[19]ETT (Henan Tuoren Medical, Henan,China) was connected to the artif icial airway of the CPR manikin performed by the same emergency medicine doctor. Three different sizes of ETT were used to observe the physiological changes with changes in ETT size(internal diameter 6.0, 7.0, and 8.0 mm) (Figure 1A) and each ETT was fixed at 21 cm. Flow analyzer (Certifier FA Plus Ventilator Test System 4080, TSI Incorporated,USA) was connected to ETT to measure the changes in PIFR, Ppeak, and Pmeanwith changes in ETT size. For constant ventilation support (Figure 1B), the mechanical ventilator (MV2000 SU:M2, MEK-ICS CO., Pajusi, South Korea) was used under the same conditions:volume-controlled mandatory ventilation, tidal volume of 500 mL, inspiration time of 1.2 seconds, constant f low pattern, ventilation rate 10 breaths/minute, positive end expiratory pressure of 3 cmH2O, and maximum trigger limit.[20]
To compare the physiological changes during CPR,we divided the study into two groups (no CPR group and CPR group). In the CPR group, physiological changes were continuously measured during chest compression.Mechanical chest compression device (LUCAS2, Stryker Medical, 3800 E. Centre Ave. Portage, Michigan, USA)was used to maintain constant chest compression depth and rate (LUCAS2, mode: active continuous, chest compression rate 102±2/minute, chest compression depth 2–2.5 inches). Each group was continuously measured by the f low analyzer for 10 minutes.
Statistical analysis
The Mann–Whitney U test and Kruskal-Wallis test were conducted for comparisons of the continuous variables. Continuous variables are presented as median with interquartile range. Bonferroni correction was used for multiple comparisons (P<0.05/3 caused by 3 groups).Data were analyzed using PASW/SPSS, version 19.0(IBM Inc., Chicago, IL, USA). Signif icance level was set at P<0.05.
RESULTS
The compliance of the prepared CPR manikin was not significantly different according to ETT size.However, the resistance increased as the ETT size decreased (Table 1).
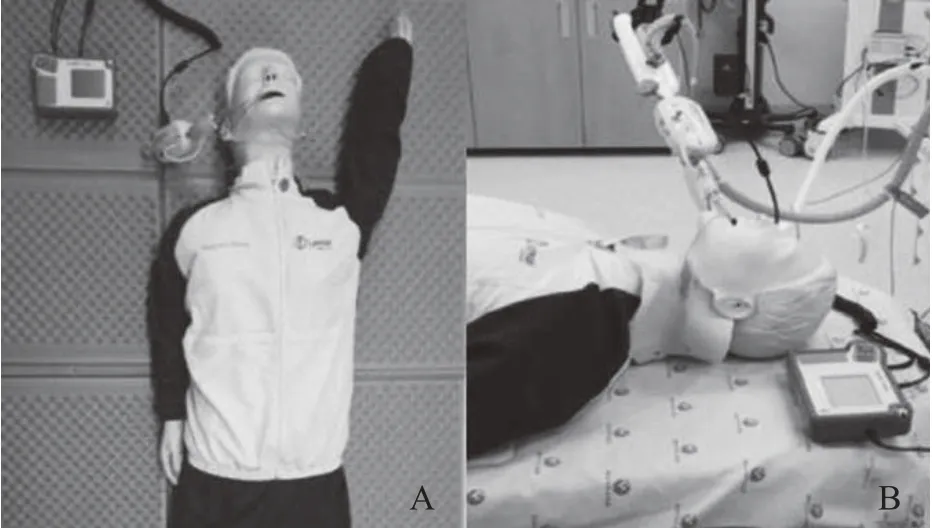
Figure 1. Manikin model. A: CPR manikin with airway circuit connected to the f low analyzer; B: connection with ventilator circuit.
No CPR group
PIFR, Ppeak, and Pmeantended to decrease with increasing ETT size, with PIFR (6.0 mm: 30.9 L/minute[30.8–31.1], 7.0 mm: 27.5 L/minute [27.1–27.9], 8.0 mm: 27.8 L/minute [26.9–28.2]), Ppeak(6.0 mm: 24.42 cmH2O [24.20–24.51], 7.0 mm: 23.79 cmH2O [23.51–23.96], 8.0 mm: 23.44 cmH2O [22.78–23.56]), Pmean(6.0 mm: 6.97 cmH2O [6.85–7.04], 7.0 mm: 6.74 cmH2O[6.61–6.85], 8.0 mm: 6.62 cmH2O [6.53–6.65]).
There was a signif icant difference in the comparison to ETT size (6.0 mm vs. 8.0 mm): PIFR (30.9 L/minute[30.8–31.1] vs. 27.8 L/minute [26.9–28.2], P<0.001),Ppeak(24.42 cmH2O [24.20–24.51] vs. 23.44 cmH2O[22.78–23.56], P<0.001), Pmean(6.97 cmH2O [6.85–7.04]vs. 6.62 cmH2O [6.53–6.65], P<0.001). Further, a signif icant difference was observed in PIFR between ETT size 6.0 mm and the other ETT sizes (Figure 2A), and a significant difference in Ppeakand Pmeanwas observed between ETT sizes 7.0 mm and 8.0 mm (Ppeak: 23.79 cmH2O [23.51–23.96] vs. 23.44 cmH2O [22.78–23.5],P<0.001; Pmean: 6.74 cmH2O [6.61–6.85] vs. 6.62 cmH2O[6.53–6.65], P<0.001) (Figure 2B and C).

Table 1. Compliance and resistance of the simulation manikin
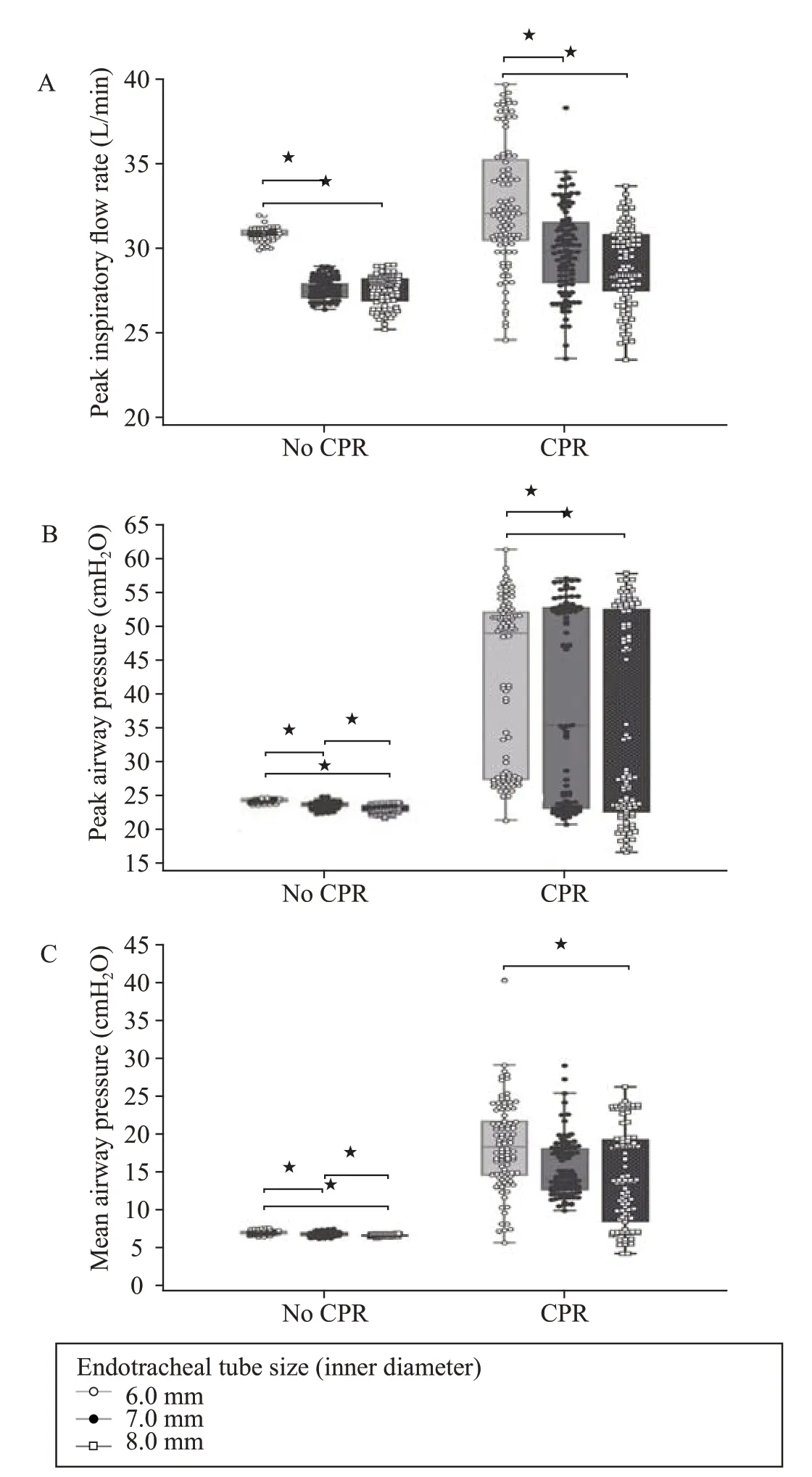
Figure 2. Changes of the f low rate, peak airway pressure, and mean airway pressure according to each endotracheal tube size (internal diameter). Bonferroni correction for multiplicity, P<0.05/3.
CPR group
PIFR, Ppeak, and Pmeantended to decrease with increasing ETT size in the CPR group too, with PIFR (6.0 mm: 32.1 L/minute [30.5–35.3], 7.0 mm: 29.9 L/min[28.0–31.6], 8.0 mm: 28.9 L/minute [27.5–30.8]), Ppeak(6.0 mm: 48.84 cmH2O [27.46–52.11], 7.0 mm: 35.31 cmH2O [23.15–52.69], 8.0 mm: 27.45 cmH2O [22.53–52.57]), Pmean(6.0 mm: 18.34 cmH2O [14.61–21.66], 7.0 mm: 35.31 cmH2O [23.15–52.69], 8.0 mm: 13.66 cmH2O[8.41–19.24]).
However, the range of these changes was greater in the CPR group than in the no CPR group (6.0 mm vs.8.0 mm): PIFR (32.1 L/min [30.5–35.3] vs. 28.9 L/min[27.5–30.8], P<0.001), Ppeak(48.84 cmH2O [27.46–52.11]vs. 27.45 cmH2O [22.53–52.57], P=0.007), and Pmean(18.34 cmH2O [14.61–21.66] vs. 13.66 cmH2O [8.41–19.24], P<0.001). Moreover, a significant difference was observed in PIFR, between 6.0 mm and the other ETT sizes, similar to the results observed for the no CPR group (Figure 2A). Between 7.0 mm and 8.0 mm ETT,there was no signif icant difference in Ppeak(P<0.088) and Pmean(P<0.131) (Figure 2B and C).
DISCUSSION
To reduce the ITP during CPR, various studies have been carried out and new, supplementary instruments have been developed. Active compression-decompression(ACD) and inspiratory impedance threshold device (ITD)have been designed to increase the coronary perfusion with negative ITP. The ACD + ITD CPR lifts the chest using the suction force of the machine itself to the recoil phase and prevents the inhalation of air during recoil phase, thereby causing the reduction of the ITP. However,the effect of these devices is still controversial. In a recent study, ITD attached to a face mask or an ETT resulted in a significantly lower negative ITP in the recoil phase of ACD-CPR than in controls. Further, survival rates improved in the ACD-CPR group.[21,22]These instruments are good examples of continuous research on proper ventilation to maintain high quality CPR.
In a recent meta-analysis study, patients with OHCAs who received ETT were more likely to have improved ROSC and greater survival till hospital admission and were more likely to be neurologically intact than those who received supra-glottic airway (SGA).[23]However, another study has shown that SGA is superior to endotracheal tube intubation (ETI) in the emergency medical services (EMS) stage and 72-hour prognosis of SGA.[24]As such, which method is superior between the ETI and the SGA has not yet been established. ETI has the disadvantage of increasing the interruption time according to the degree of skill of the provider. Nevertheless, ETI is being used at the hospital level because of its ability to continue chest compression during CPR. In this study, we have determined the physiological differences among the different ETT sizes which may help in determining the appropriate ETT size for an adult.
Flevari et al[25]demonstrated the relationship between inspiratory resistance and inspiratory flow in commonly used adult ETTs within a range of in vitro conditions using the Rohrer equation. In their study, the resistance of ETT increased with increasing inspiratory flow and decreasing the internal diameter of ETT. We obtained similar results in our study in the no CPR group(Table 1). Several studies have been published on the changes in gas dynamic according to ETT size. However,none of these changes in ETT have been studied in the presence of CPR. To the best of our knowledge, this is the first study to evaluate the changes in PIFR, Ppeak,and Pmeanwith a change in ETT size during adult CPR.We demonstrated that the change in PIFR, Ppeak, and Pmeanwas related to the internal diameter of ETT. High airway pressure and high tidal volume are known to be associated with lung injury. In the animal model,it is suggested that the peak airway pressure causes progressive impairment in lung function and lead to acute respiratory failure when the peak airway pressure is 50 cmH2O or higher.[26,27]In our study, CPR group showed a sharp increase in Ppeakas compared to the no CPR group.In case of the 6.0 mm ETT in the CPR group, Ppeakwas observed to increase up to 62 cmH2O. This tendency was found to be statistically signif icant even when compared with 8.0 mm ETT (6.0 mm vs. 8.0 mm, Ppeak: 48.84 cmH2O [27.46–52.11] vs. 27.45 cmH2O [22.53–52.57],P<0.001). This rapid increase in the airway pressure was observed when inspiration was initiated by compression phase in chest compression. Therefore, this sudden increase in Ppeakduring chest compression is considered to be the cause of lung injury. Thus, using an ETT with a large internal diameter during CPR will prevent a sharp increase in Ppeakand this may reduce lung injury. On the other hand, no study has been conducted to investigate the effect of ETT size on the change of intubation time,but it was expected that the larger ETT size had a greater intubation primary failure rate than a smaller ETT size. In this study, there was no statistically significant difference in Ppeakbetween 7.0 mm and 8.0 mm in CPR group. Therefore, the clinician should consider using ETT of the largest size which is appropriate to the body shape and weight of the patient.
This study has some limitations. First, the experiment was conducted using a manikin model since we cannot conduct experiments on human subjects due to ethical concerns. However, in general, there is a clear difference in lung compliance and airway resistance between a human and a manikin. Wright et al[28]showed that the difference in resistance according to ETT size was greater in vivo than in vitro. They explained that in vivo,the resistance increases due to differences caused by secretion, turbulence flow, and head and neck position.Thus, the manikin is considered to be a limitation due to these reasons. Second, the ETT used in this study ranged from 6.0 to 8.0 mm, and each tube had a difference in overall length depending on its diameter. According to the law of Hagen-Poiseuille, when laminar resistance (R)of ETT is directly proportional to the tube length (L),inversely proportional to the fourth power of its internal radius (r), and independent of f low, that is, R = 8ηL/ πr4.Mohr et al[29]showed that the shortening of ETT length had minimal effect on the work of breathing by using an in vitro lung model. The change in resistance and work of breathing due to the difference in ETT length was minimal but is considered to be a limitation.
CONCLUSION
The changes of PIFR, Ppeak, and Pmeanvaried according to the inner diameter of ETT. As the inner diameter of ETT decreased, the values of PIFR, Ppeak,and Pmeantended to increase. Higher airway pressures were measured in the CPR group than in the no CPR group. This rapid increase in Ppeakmay cause lung injury.Therefore, the use of large sized ETT in adult CPR will help in reducing lung injury.
Funding:This work was supported by the Chungnam National University Hospital Research Fund, 2016.
Ethical approval:Not needed.
Conflicts of interests:The authors declare that they have no competing interests. The funders had no role in the design, conduct,analysis, or interpretation of data or in writing the manuscript.
Contributors:JWK wrote the f irst draft of this paper. All authors approved the f inal version.
 World journal of emergency medicine2020年2期
World journal of emergency medicine2020年2期
- World journal of emergency medicine的其它文章
- Information for Readers
- Food poisoning associated methemoglobinemia: Time to wake up
- Acute obstructive f brinous laryngotracheobronchitis induced by severe glyphosate surfactant intoxication:A case report
- A young lady presenting to the emergency department with blue lips: A case study with review of literature
- Outcome predictors for severely brain-injured patients directly admitted or transferred from emergency departments to a trauma center
- An unexpected electrocardiogram sign of subacute left ventricular free wall rupture: Its early awareness may be lifesaving