Outcome predictors for severely brain-injured patients directly admitted or transferred from emergency departments to a trauma center
2020-03-02 10:44:42RyneJenkinsNicholasMorrisBryceHaacRichardVanBesienDeborahSteinNeerajBadjatiaAmirMedicGaurikaMesterQuincyTran
Ryne Jenkins, Nicholas A. Morris, Bryce Haac, Richard Van Besien, Deborah M. Stein, Neeraj Badjatia,, Amir Medic, Gaurika Mester, Quincy K. Tran,5
1 Program in Trauma, The R Adams Cowley Shock Trauma Center, University of Maryland School of Medicine, Baltimore,MD, USA
2 Section of Neurocritical Care and Emergency Neurology, Department of Neurology, University of Maryland School of Medicine, Baltimore, MD, USA
3 University of Maryland School of Medicine, Baltimore, MD, USA
4 University of Maryland at College Park, College Park, MD, USA
5 Department of Emergency Medicine, University of Maryland School of Medicine, Baltimore, MD, USA
Dear editor,
After sustaining severe traumatic brain injury (TBI),patients frequently require invasive mechanical ventilation(MV). However, up to 26% of patients require tracheostomy due to failure to wean from the ventilator.[1]The decision of when to perform tracheostomy is important as it balances the risk between avoiding prolonged MV and avoiding risk of tracheostomy. Early predictors for tracheostomy,i.e., clinical factors when patients first present to an Emergency Department after trauma or when patient f irst arrive at a regional trauma center, can help clinicians’medical decision-making process.
We retrospectively analyzed the charts of 201 adult patients who sustained severe TBI and received MV>72 hours at our regional trauma center from January to December 2014. Forty-eight (24%) patients were transferred from another hospital’s ED and 153 (76%)patients were admitted directly from sites of injury.Mean age was 48±21 years, and mean Injury Severity Score was 29±10. Multivariable logistic regression of significant independent variables, which were defined as P-value≤0.10 in univariate logistic regression,showed that Shock Index (SI) during ED stay <0.5 was associated with higher likelihood for tracheostomy (Odd Ratio [OR] 11, 95% Confidence Interval [CI] 1.4–87,P=0.022) (Table 1). Among factors at admission to the trauma center, being transferred from trauma-designated EDs (OR 7.6; 95% CI 1.1–51 [P=0.036]) and Glasgow Coma Scale at hospital day 5 (HD5GCS) ≤ 8 (OR 10;95% CI 5.4–53 [P<0.001]) were signif icantly associated with higher likelihood for needs of tracheostomy.
Our finding is consistent with a previous study which suggested that low HD5GCS was associated with higher likelihood of tracheostomy. Ahmadinegad et al[2]found that 85.7% of patients with HD5GCS <9 required tracheostomy. However, it is also possible in our study that trauma intensivists may be inclined to perform tracheostomy early with patients with HD5GCS ≤8, rather than repeatedly attempt to wean them off the ventilator.
Our study might provide information for trauma intensivists at referral tertiary trauma centers, supporting their communications with referring emergency physicians to improve patient outcomes. Previous study of trauma patients suggested that Shock Index, def ined as ratio of heart rate and systolic blood pressure, increasing more than 0.3 was associated with higher mortality.[3]Our data also suggested that emergency physicians should maintain TBI patients’ heart rate and systolic blood pressure within normal range, to prevent rising SI, which is harmful as previously suggested[3]and to avoid lowering Shock Index to less than 0.5, which was associated with increased needs for tracheostomy.Emergency physicians should pay special attention during the peri-intubation period, which is associatedwith an increased likelihood of severe cardiovascular collapse,[4]which will affect SI, particularly among patients with severe TBI, to avoid secondary brain injury.
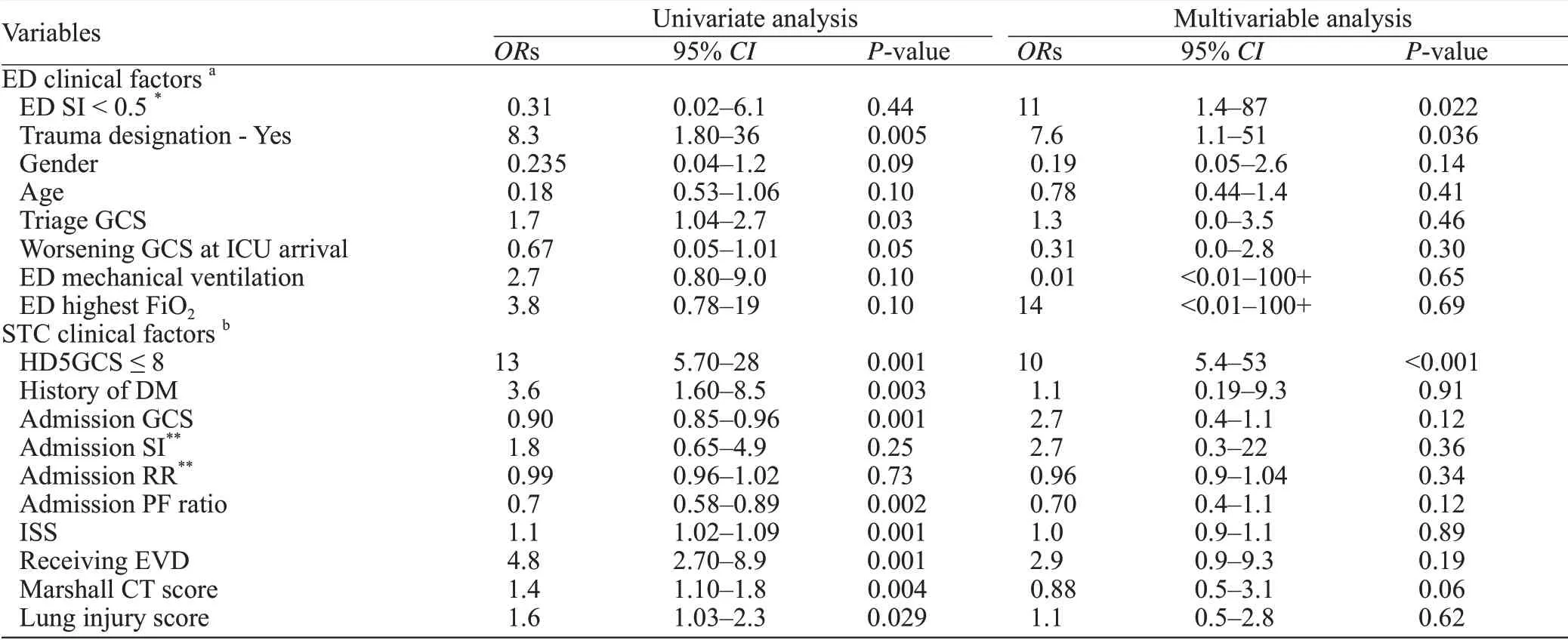
Table 1. Multivariable logistic regressions for association of clinical factors and tracheostomy among patients with severe TBI
Further study is needed to conf irm our f indings that,patients with severe traumatic brain injury while having a SI <0.5 in the ED, or Glasgow Coma Scale score on hospital day 5 ≤8, were associated with increased likelihood of requiring tracheostomy.
ACKNOWLEDGEMENT
We thank Ms. Linda Kesselring for her edits of the manuscript.
Funding:The authors received no financial support for the investigation or manuscript development.
Ethical approval:Not needed.
Conf icts of interest:The authors declared no conf lict of interest in preparation of this manuscript.
Contributors:RJ, QKT participated in study concept and design;data acquisition, analysis, and interpretation; drafting of the manuscript; and critical revision of the manuscript. RVB, AM,GM, NM, BH participated in data acquisition, drafting of the manuscript and provided critical revision of the manuscript. NB,DSM participated in study concept and design; drafting of the manuscript; and critical revision of the manuscript.
 World journal of emergency medicine2020年2期
World journal of emergency medicine2020年2期
- World journal of emergency medicine的其它文章
- Information for Readers
- Food poisoning associated methemoglobinemia: Time to wake up
- Acute obstructive f brinous laryngotracheobronchitis induced by severe glyphosate surfactant intoxication:A case report
- A young lady presenting to the emergency department with blue lips: A case study with review of literature
- An unexpected electrocardiogram sign of subacute left ventricular free wall rupture: Its early awareness may be lifesaving
- Effect of low high-density lipoprotein levels on mortality of septic patients: A systematic review and meta-analysis of cohort studies