Post-infantile giant cell hepatitis:A single center's experience over 25 years
2020-01-06 05:21:34BassemMattaRicardoCabelloMordechaiRabinovitzMartaMinerviniShahidMalik
World Journal of Hepatology 2019年12期
Bassem Matta,Ricardo Cabello,Mordechai Rabinovitz,Marta Minervini,Shahid Malik
Bassem Matta,Mordechai Rabinovitz,Department of Medicine,Division of Gastroenterology,Hepatology and Nutrition,University of Pittsburgh,Pittsburgh,PA 15213,United States
Ricardo Cabello,Department of Internal Medicine,University of Pittsburgh Medical Center,Pittsburgh,PA 15213,United States
Marta Minervini,Department of Pathology,University of Pittsburgh,Pittsburgh,PA 15213,United States
Shahid Malik,Department of Medicine,University of Pittsburgh,Division of Gastroenterology Hepatology and Nutrition,Pittsburgh,PA 15213,United States
Abstract
Key words:Post-infantile giant cell hepatitis; Liver transplantation; Autoimmune hepatitis
INTRODUCTION
Giant cell hepatitis (GCH) is a relatively common histologic finding in neonates.It is believed to occur secondary to insults to immature hepatocytes.In children,it typically presents with cholestasis,conjugated hyperbilirubinemia and variable degrees of inflammation[1].Idiopathic GCH refers to these histologic findings with a structurally intact biliary system as opposed to conditions where biliary abnormalities are present,such as biliary atresia[1].The most commonly proposed pathophysiological hypothesis to account for the presence of giant cells includes an ineffective cytoplasmic division in the setting of cellular fission (endomitosis) in contrast to cellular hepatocyte fusion secondary to hepatic injury[2].
As common as GCH is in children,it is exceedingly rare in adults.GCH in the adult population remains very poorly defined with only 100 case reports published in the literature over the last three decades[3].In adults the entity is referred to as postinfantile giant cell hepatitis (PIGCH),also known as syncytial or adult onset GCH.PIGCH represents a histologic diagnosis that has been associated with a myriad of medical conditions including infectious,hematologic,autoimmune disorders and drug reactions (Table1)[3-13].Pathological analysis is characterized by the presence of giant multinucleated syncytial hepatocytes.In particular,more than four to five nuclei in hepatocytes should be seen in a single lobule combined with other features of hepatitis such as lobular disarray,inflammation,Kupffer cell hypertrophy and spotty hepatocytes necrosis (Figure1).
The clinical course of patients with giant cells on histology is widely variable,ranging from minimal symptoms without major clinical implications to acute liver failure that is often times fatal despite standard clinical care.In the current study,we aimed to present our center's experience with this very rare disease entity in an attempt to shed more light about its predisposing factors,outcomes and efficacy of proposed therapeutic interventions.
MATERIALS AND METHODS
After obtaining local institutional review board approval,we queried liver biopsy reports (36726) at the University of Pittsburgh Medical Center electronic records usingthe keywords “giant cell hepatitis” from January 1,1991 to December 6,2016.Our search yielded 127 individual patient records,of which 45 were diagnosed prior to 18 years of age.The remaining 82 records were evaluated by three physicians (BM,SM,MM) after which 50 patients were identified as carrying a definite diagnosis of PIGCH based on liver biopsy.In order to better analyze patient characteristics and outcomes,subjects were separated into a non-transplant (native) liver group and a post-liver transplant (allograft) group.

Table1 Reported causes of post-infantile giant cell hepatitis
RESULTS
The incidence of PIGCH was approximately 0.14% of all biopsies queried in the 25-year period.The mean age of the studied patient sample was 48 years with 66%females.Liver function tests were classified as follows:38.2% cholestatic,35.3%hepatocellular and 26.5% mixed; 73.5% of patients had bilirubin values exceeding 1.5 mg/dL at the time of diagnosis and 42% of patients had bilirubin values exceeding 5 mg/dL.Mean follow up of the entire cohort was over six years (79 mo; SD = 76.1).Patient demographics and liver function tests for patients are outlined in Table2.Patients with GCH found in the native liver group were older,had higher aspartate aminotransferase,alanine aminotransferase and total bilirubin when compared to the allograft group.
Autoimmune hepatitis (AIH) was found to be the most prevalent predisposing factor leading to PIGCH constituting 32% of cases,while drugs accounted for 12% of cases.Other etiological associations included viral infections [hepatitis A,B,C (HCV),cytomegalovirus (CMV),Epstein-Barr virus],systemic autoimmune conditions (but not enough to give a diagnosis of AIH) and hematologic conditions.In nearly 1/3 of cases,no predisposing factor for PIGCH was found (idiopathic).In the post-transplant population,the most prevalent predisposing factor leading to PIGCH was AIH as well,accounting for 30% of cases.

Figure1 Liver biopsy of 44-year-old female with autoimmune hepatitis (hematoxylin and eosin stain 40 ×).Biopsy revealed chronic hepatitis with prominent giant multinucleated hepatocytes.
Autoimmune markers related to liver disease were common:Anti-nuclear antibody in 34% of cases,elevated immunoglobulin G in 22% of cases,anti-smooth muscle antibody in 10% of cases,anti-mitochondrial antibody in 8% of cases and anti-liver kidney microsomal antibody in 2% of cases.
Drugs which were identified as the possible culprit for GCH development consisted of microdantin,ranitidine,omeprazole,moxifloxacin,ranitidine,plaquenil as well as chromium picolinate.
由于MOOC教學的特點,在進行教學設(shè)計時可充分利用碎片化的時間來學習課程知識點,教學設(shè)計的時間上不能僅僅局限于課堂的45分鐘,將知識點的學習設(shè)計成三個環(huán)節(jié),包括“任務(wù)導(dǎo)入”、“任務(wù)實施”及“成果評價”。具體的教學設(shè)計見圖1。
Notable pathological findings included diffuse necrosis in 24% of the patients,inflammation and acute hepatitis in 56% of patients and overt cirrhosis in 12% of patients.Of the ten patients with GCH post-liver transplant,five had concomitant features of acute cellular rejection.
Management of PIGCH consisted mainly of immunosuppression,viral targeted therapy,supportive care and in six cases liver transplantation.Management and outcomes are outlined in Table3.Among the patients who were treated with immunosuppression,eight patients (53%) had improvement in their liver function tests.Of the patients treated with ganciclovir,two patients (100%) had improvement in their liver function tests.
Among the native group,five patients (13%) required liver transplantation,and one patient developed graft failure from post-transplant GCH and required a second transplant.Five (13%) patients died from liver-related complications in the native liver group compared to two (20%) in the allograft group.Among these seven patients,five died with acute liver failure.Patient #1 had received two liver transplants.The first transplant was for HCV cirrhosis and subsequently developed PIGCH in the allograft despite achieving a sustained virologic response after antiviral therapy.This patient eventually developed allograft cirrhosis attributed to PIGCH and required a second transplant for this reason.The patient died of a spontaneous intracranial hemorrhage.Patient #2 had developed cirrhosis attributed to PIGCH and died of pneumonia and sepsis.The five remaining patients presented with acute liver failure.Patient #3 was urgently transplanted but developed infected necrotizing pancreatitis to which he succumbed.Patient #4 was found to develop a pneumothorax and died from hemothorax after placement of a thoracotomy tube.Patient #5 died after developing subcapsular hepatic bleeding following a liver biopsy.Patients #6 and #7 developed a massive variceal bleed and lower gastrointestinal bleeding (exact cause unknown),respectively,that led to their demise.
Of the 50 patients with GCH,12 (6 native and 6 allograft) underwent a repeat liver biopsy of which 66% still had evidence of GCH despite treatment.Half of these patients had undergone liver transplantation (AIH,primary sclerosing cholangitis/AIH overlap,HCV,GCH,alcoholic and cryptogenic cirrhosis).These patients had persistent GCH on repeat biopsies despite immunosuppression.The patient with primary sclerosing cholangitis/AIH overlap had improvement of GCH findings on subsequent biopsy.One subject had evidence of acute cellular then chronic rejection on subsequent biopsies.Cirrhosis developed in a patient transplanted for alcoholic cirrhosis and GCH.Among the native liver group,six patients had recurrent GCH on biopsy.One had acute hepatitis B,while the rest did not have a specific predisposing factor.
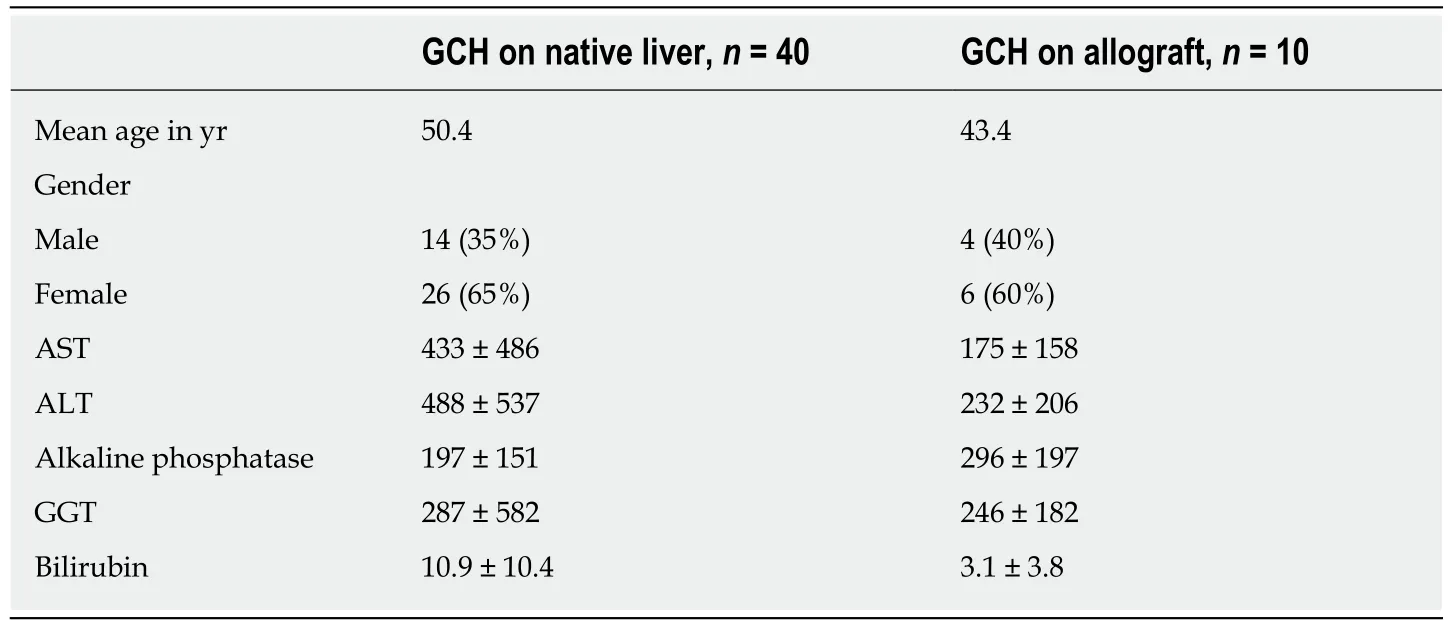
Table2 Patient characteristics and liver function tests
DISCUSSION
With only 100 cases reported in the adult literature,PIGCH remains poorly understood.The prevalence of this disease has been reported at 0.1% to 0.25%[3],which is consistent with the incidence in our cohort (0.14%).Given the rarity of this entity,outcomes and management are largely based on anecdotal evidence.There are no approved therapies and no consensus on management strategies[13].
The histological finding of giant cells in adults seems to be a manifestation of hepatic stress as opposed to a primary hepatic injury[3,10].The diagnosis is made based on the presence of multinucleated giant cells usually evident in zones 1 and 3 of the Rappaport acinus.More than four to five nuclei in hepatocytes should be seen in a single lobule combined with other features of hepatitis such as lobular disarray,acinar inflammation,Kupffer cell hypertrophy and spotty hepatocytes necrosis.Other common features may include non-suppurative cholangitis,ductopenia and different stages of periportal fibrosis leading to cirrhosis[6,14].Similar histological findings were observed among our patient cohort:The majority had notable inflammation on pathology,while a quarter of them exhibited evidence of hepatic necrosis (28% spotty necrosis,48% bridging/confluent necrosis,19% sub-massive necrosis and 5% massive necrosis),with 12% demonstrating overt cirrhosis,which is comparable to previous reported rates in the literature of about 13%[3].
Out of the six liver transplant recipients for PICGH,two died with recurrent disease.The first patient died in the early post-transplant period,and the second patient died 11 years later.Two patients required two more liver transplants each for recurrent decompensated cirrhosis despite being on standard immunosuppression.One patient developed cirrhosis with features of chronic rejection,which was thought to be related to recurrent hepatitis C,and another was related to CMV hepatitis.
Scant data exists on PIGCH in the post-transplant setting with prior observations indicating the need for re-transplantation in the majority of recipients due to recurrent disease.Pappoet al[15]examined the clinical and pathologic course of seven patients who developed GCH after liver transplantation.Five of these patients had GCH as their native liver disease.Two patients died.Two patients required re-transplantation because of recurrent GCH.One patient with recurrent GCH was still alive six years after transplantation.Similarly,in our study,ten patients developed GCH after liver transplantation.Two patients had GCH as their native liver disease.One patient died due to sepsis related to a second liver transplantation.Two patients developed recurrent GCH on the allograft; one of those patients had their immunosuppression increased and had survived at two years and the other patient required retransplantation.Two patients developedde novoGCH that required an increase in immunosuppression; one patient eventually needed liver transplantation and the other one improved with medical management.One patient developedde novoGCH and CMV hepatitis and was treated with ganciclovir.The remaining four patients were lost to follow up.
Management strategies to treat recurrence mainly consisted of increasing immunosuppression and in rare cases the institution of ribavirin with variable success[16,17].
Our results were consistent with prior reports indicating a potential autoimmune link to the findings of PIGCH.We concluded that an autoimmune type hepatitis was seen in 1/3 of our patients; 34% of the patients had a positive anti-nuclear antibody,22% had an elevated immunoglobulin G,while 12 patients would fulfill at least a probable diagnosis of AIH based on the AIH scoring system[18](Table4).

Table3 Predisposing factors,n (%)
The majority of our patients were female (66%),which is somewhat different to previous reports with approximately equal numbers between genders[3].Idiopathic PIGCH was present in 30% of our cohort,which is much higher than prior published studies.A higher incidence of idiopathic PIGCH in our cohort compared to the published literature is likely a manifestation of publication bias,i.e.cases of PICGH where there is no clear link may be less apt to be reported[3].Drug induced liver injury was the culprit in 12% of cases with all of the reported drugs being novel associations with PIGCH (Table4).
Viral causes amongst our cohort seem to have been less frequent than previously reported.Outcomes of those with a viral cause was variable,although the cases where CMV infection was felt to be the culprit did respond well to ganciclovir,similar to cases reported in the literature[7,19].
The majority of deaths were in the group labeled idiopathic PIGCH,while only two out of sixteen patients with autoimmune like features died.Notably,all of the idiopathic patients were managed supportively while most of the autoimmune cases were managed with immunosuppression.One patient who died had chronic HCV in addition to AIH.HCV therapy (standard of therapy at the time was interferon-based treatment) was not offered given the patient's decompensated state.PIGCH has been described in both acute and chronically infected HCV patients (or co-infected with HIV) with a relatively good prognosis after treatment with interferon and ribavirin or immunosuppressive therapy when autoimmune features are present[19-22].No studies have been published to date using the highly potent direct acting antivirals that might potentially prove to have even better outcomes with higher rates of viral eradication[23].
The presentations and outcomes of our patients coincide with previously reported observations in the literature of being highly variable.Some patients only manifested in mild elevations in liver function tests while others developed acute liver failure resulting in death or the need for liver transplantation (Table2).Most patients responded well to immunosuppressive therapy that mainly consisted of intravenous hydrocortisone,prednisone,azathioprine and tacrolimus,especially with the presence of autoimmune features.One case (previously published) with PIGCH secondary to AIH complicating ulcerative colitis responded to prednisone with improved liver functions despite worsening ulcerative colitis (the patient ultimately required acolectomy)[12].Several cases of PIGCH associated with chronic lymphocytic leukemia have been reported with largely favorable outcomes after being managed with intravenous immunoglobulins (in the events where immunoglobulins are low),rituximab or steroids[8,13].This is similar to our patient with chronic lymphocytic leukemia who was managed successfully with prednisone but ultimately developed cirrhosis[24].
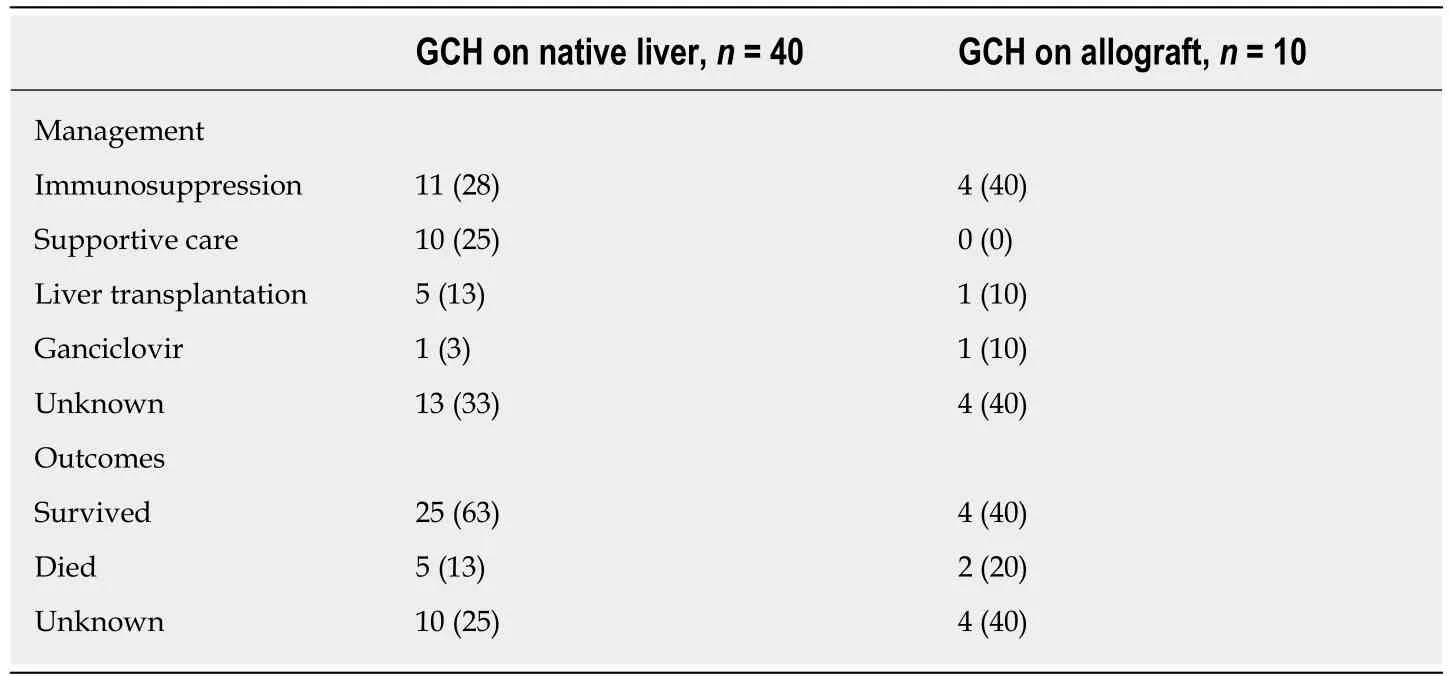
Table4 Management and outcomes,n (%)
Our study has several limitations.It is based on retrospective chart review and is mainly descriptive.That being said,it includes the largest number of unique cases of PIGCH from a single institution included in a single manuscript.
The exact etiology of PIGCH and mechanism of injury remains unknown,and the histological findings are likely related to an idiosyncratic or cytopathic response to various hepatocyte stimuli.Our series suggested an autoimmune cause as the most common association.The diagnosis of PIGCH remains clinically challenging and requires a high index of suspicion as well as a thorough history,physical examination and serological workup,which should include viral,hematologic and autoimmune causes.Ultimately a liver biopsy is required as PICGH remains a purely histomorphological diagnosis.Treatment of the underlying cause (especially if it is autoimmune or viral) can result in clinical stability in a large number of cases.Treatment and monitoring should be done in close association with specialty centers including those capable of liver transplantation.
ARTICLE HIGHLIGHTS
Research background
Giant cell hepatitis in the adult population remains very poorly defined with only 100 case reports published in the literature over the last three decades.Pathological analysis is characterized by the presence of giant multinucleated syncytial hepatocytes.The clinical course of patients with giant cells on histology is widely variable,ranging from minimal symptoms without major clinical implications to acute liver failure that is often times fatal despite standard clinical care.
Research objectives
Our primary objective was to present our center's experience in an attempt to learn about the predisposing factors,outcomes and efficacy of proposed therapeutic interventions for giant cell hepatitis.
Research methods
A retrospective chart review was conducted through the electronic records of the University of Pittsburgh Medical Center.We queried 36726 liver biopsy reports from January 1,1991 to December 6,2016.Our search yielded 50 patients who were identified as carrying a definite diagnosis of post-infantile giant cell hepatitis (PIGCH) by pathology.The data collected included demographic information,laboratory data (liver function tests,autoimmune markers) and transplant status.In order to better analyze patient characteristics and outcomes,subjects were separated into a non-transplant (native) liver group and a post-liver transplant (allograft) group.
Research results
The incidence of PIGCH was approximately 0.14% of all biopsies queried in the 25-year period.The mean age was 48 years with 66% females.Liver function tests were classified as 38.2%cholestatic,35.3% hepatocellular and 26.5% mixed.Autoimmune hepatitis was found to be the most prevalent predisposing factor leading to PIGCH constituting 32% of cases.Management consisted mainly of immunosuppression,viral targeted therapy,supportive care and in six cases liver transplantation.
Research conclusions
The diagnosis of PIGCH remains clinically challenging and requires a high index of suspicion as well as a thorough history,physical examination,serological workup and liver biopsy.Treatment of the underlying cause can result in clinical stability in a large number of cases.
Research perspectives
This study reports our center's experience with PIGCH and the importance of thorough history,physical examination,serologic work up and liver biopsy in its diagnosis.Further research should aim at recognizing risk factors for progression from PIGCH to liver failure and further evaluation of therapeutic interventions (immunosuppressionvsviral targeted therapyvsliver transplantation).
猜你喜歡
美食(2022年2期)2022-04-19 12:56:24
少兒美術(shù)·書法版(2021年10期)2021-10-20 06:14:10
內(nèi)蒙古教育(2021年20期)2021-03-08 01:09:14
計算機教育(2020年5期)2020-07-24 08:53:38
甘肅教育(2020年12期)2020-04-13 06:24:48
家庭影院技術(shù)(2019年11期)2019-12-09 09:14:30
小天使·一年級語數(shù)英綜合(2018年9期)2018-10-16 06:30:16
藝術(shù)啟蒙(2018年7期)2018-08-23 09:14:18
海峽姐妹(2017年7期)2017-07-31 19:08:17
Coco薇(2017年5期)2017-06-05 08:53:16