大鼠腦損傷聯合他克莫司促進坐骨神經再生的效果
2019-11-14 10:13:25何新澤林書卿楊濤王成剛李芹于立志孫金占王培
中國當代醫藥 2019年25期
何新澤 林書卿 楊濤 王成剛 李芹 于立志 孫金占 王培

[摘要]目的 探討大鼠腦損傷聯合他克莫司促進坐骨神經再生的效果。方法 選取180只SD大鼠,隨機分為4組,每組各45只,按照顱腦損傷模型(Feeney法)和坐骨神經損傷模型(Sunderland V型)造模,A1組:顱腦損傷合并坐骨神經損傷聯合應用他克莫司;A2組:顱腦損傷合并坐骨神經損傷聯合應用生理鹽水;B1組:單純坐骨神經損傷聯合應用他克莫司;B2組:單純坐骨神經損傷聯合應用生理鹽水。造模后第4、8、12周,測定坐骨神經指數(SFI)、腓腸肌恢復率,進行神經組織Masson染色;造模后第8、12周觀察脊髓神經元辣根過氧化物(HRP)的逆行示蹤標記。結果 造模后第4周,A1組與A2組、B1組與B2組的SFI比較,差異無統計學意義(P>0.05);造模后第4周,A1、A2組的SFI均優于B1、B2組,差異有統計學意義(P<0.01);造模后第8、12周,A2組與B1組的SFI比較,差異無統計學意義(P>0.05);造模后第8、12周,A1組的SFI優于A2、B1、B2組,A2、B1組的SFI均優于B2組,差異有統計學意義(P<0.01);4周后,各組大鼠的SFI逐漸升高(P<0.01)。造模后第4周,A2、B1、B2組的腓腸肌恢復率比較,差異無統計學意義(P>0.05);A1組造模后第4周的腓腸肌恢復率高于A2、B1、B2組,差異有統計學意義(P<0.01);造模后第8、12周,A1、A2、B1組的腓腸肌恢復率均明顯高于B2組,差異有統計學意義(P<0.01);造模后第8、12周,A1組與A2組的腓腸肌恢復率比較,差異無統計學意義(P>0.05);A1、A2組造模后第8周的腓腸肌恢復率均高于B1組,差異有統計學意義(P<0.01);造模后第12周,A1組的腓腸肌恢復率高于B1組,差異有統計學意義(P<0.01);A2組與B1組造模后第12周的腓腸肌恢復率比較,差異無統計學意義(P>0.05);4周后,各組大鼠的腓腸肌恢復率逐漸升高(P<0.01)。Masson染色觀察造模后第12周A1組膠原纖維均勻分布,并呈波浪形隨神經纖維排列,A2、B1組可見綠染與紅染分布均勻,B2組可見大量膠原纖維,少量再生的軸突。造模后第8周,A1組的HRP標記陽性率高于A2、B1、B2組,A2組的HRP標記陽性率高于B1、B2組,B1組的HRP標記陽性率高于B2組,差異有統計學意義(P<0.01);造模后第12周,A1組的HRP標記陽性率高于A2、B1、B2組,A2、B1組的HRP標記陽性率均高于B2組,差異有統計學意義(P<0.01);A2組造模后第12周的HRP標記陽性率與B1組比較,差異無統計學意義(P>0.05)。結論 腦損傷合并周圍神經損傷聯合應用他克莫司干預可促進神經損傷修復,顱腦損傷與他克莫司作用的機制不完全相同,腦損傷促進周圍神經損傷修復的機制仍需進一步深入研究。
[關鍵詞]顱腦損傷;周圍神經;神經修復與再生;他克莫司
[中圖分類號] R318? ? ? ? ? [文獻標識碼] A? ? ? ? ? [文章編號] 1674-4721(2019)9(a)-0007-06
Effect of rat brain injury combined with Tacrolimus on promoting sciatic nerve regeneration
HE Xin-ze1? ?LIN Shu-qing1? ?YANG Tao1? ?WANG Cheng-gang1? ?LI Qin1? ?YU Li-zhi2? ?SUN Jin-zhan2? ?WANG Pei3
1. Department of Emergency, Binzhou Central Hospital, Shandong Province, Binzhou? ?251700, China; 2. Department of Trauma Orthopedics, Binzhou Central Hospital, Shandong Province, Binzhou? ?251700, China; 3. Department of Hand and Foot Surgery, Affiliated Hospital of Chengde Medical University, Hebei Province, Chengde? ?067000, China
[Abstract] Objective To investigate the effect of rat brain injury combined with Tacrolimus on promoting sciatic nerve regeneration. Methods A total of 180 SD rats were randomly divided into 4 groups with 45 rats in each group and modeled according to the craniocerebral injury model (Feeney method) and the sciatic nerve injury model (Sunderland V type). Group A1: cerebral injury combined with sciatic nerve injury and Tacrolimus; group A2: saline in cerebral injury combined with sciatic nerve injury; group B1: sciatic nerve injury combined with Tacrolimus; group B2: simple sciatic nerve injury combined saline. At the fourth, eighth, and twelfth weeks after modeling, the sciatic nerve function index (SFI) and the gastrocnemius recovery rate were measured, and the tissue was subjected to Masson staining. Retrograde tracer markers of spinal cord neurons horseradish peroxide (HRP) were observed at the eighth and twelfth weeks after modeling. Results At the fourth week after modeling, there was no significant difference in SFI between group A1 and group A2, group B1 and group B2 (P>0.05). At the fourth week after modeling, the SFI of the group A1 and A2 was better than that of the group B1 and B2, and the difference was statistically significant (P<0.01). At the eighth and twelfth weeks after modeling, there was no significant difference in SFI between group A2 and group B1 (P>0.05). At the eighth and twelfth weeks after modeling, the SFI of group A1 was better than that of group A2, B1 and B2, the SFI of group A2 and group B1 was better than that of group B2, and the differences were statistically significant (P<0.01). After 4 weeks, the SFI of each group of rats gradually increased (P<0.01). At the fourth week after modeling, the recovery rate of gastrocnemius muscle in group A2, B1 and B2 was not statistically significant (P>0.05). The recovery rate of gastrocnemius muscle at the fourth week after modeling in group A1 was higher than that in group A2, B1 and B2, and the differences were statistically significant (P<0.01). At the eighth and twelfth weeks after modeling, the recovery rate of gastrocnemius muscle in group A1, A2 and B1 was significantly higher than that in group B2, and the differences were statistically significant (P<0.01). At the eighth and twelfth weeks after modeling, there was no significant difference in the recovery rate of gastrocnemius between group A1 and group A2 (P>0.05). The recovery rate of gastrocnemius muscle in the group A1 and A2 was higher than that in the group B1 at the eighth week after modeling, and the differences were statistically significant (P<0.01). At the twelfth week after modeling, the recovery rate of gastrocnemius muscle in group A1 was higher than that in group B1, and the difference was statistically significant (P<0.01). There was no significant difference in the recovery rate of gastrocnemius muscle between the group A2 and the group B1 at the twelfth week after modeling (P>0.05). After 4 weeks, the recovery rate of gastrocnemius muscle in each group gradually increased (P<0.01). Masson staining showed that the collagen fibers at the twelfth week after modeling in the group A1 were evenly distributed, and they were arranged in a wave shape with nerve fibers, the green staining and red staining distribution were uniform in the group A2 and the group B1, and a large number of collagen fibers were observed in the group B2. At the eighth week after modeling, the positive rate of HRP label in group A1 was higher than that in group A2, B1 and B2, the positive rate of HRP label in group A2 was higher than that in group B1 and group B2, and the positive rate of HRP label in group B1 was higher than that in group B2, with statistically significant differences (P<0.01). At the twelfth week after modeling, the positive rate of HRP label in group A1 was higher than that in group A2, group B1 and group B2, and the positive rate of HRP label in group A2 and group B1 was higher than that in group B2, with statistically significant differences (P<0.01). There was no significant difference in the positive rate of HRP label at the twelfth week after modeling between group A2 and group B1 (P>0.05). Conclusion Brain injury combined with peripheral nerve injury and Tacrolimus intervention can promote the repair of nerve damage. The mechanism of brain injury and Tacrolimus is not exactly the same. The mechanism of brain damage promoting peripheral nerve injury repair needs further study.
[Key words] Craniocerebral injury; Peripheral nerve; Nerve repair and regeneration; Tacrolimus
臨床工作中,顱腦損傷合并周圍神經損傷的患者并不罕見,神經損傷后的恢復具有特殊性,功能恢復不全,致殘率較高[1-5]。Wang等[2-9]研究發現,實驗大鼠在顱腦損傷后合并周圍神經損傷,損傷坐骨神經的修復速度加快,但修復機制尚不清楚。研究發現他克莫司可促進損傷神經修復再生[10-15]。大量的實驗發現,他克莫司促進周圍神經損傷后的再生,主要通過免疫抑制、神經營養來實現[16-22]。本研究擬通過他克莫司促進神經損傷恢復機制,探索顱腦損傷促進神經損傷恢復的機制。
1材料與方法
1.1造模動物與材料
本實驗于2018年10月~2019年2月在濱州市中心醫院完成。
實驗動物:選用SPF級雄性SD大鼠[北京維通利華實驗動物技術有限公司,許可證號:SCXK(京)2012-0001]180只,200~220 g。飼養在晝夜各12 h節律下,實驗室溫度維持在(23±1)℃。將大鼠完全隨機分為4組,每組各45只。本研究經過濱州市中心醫院動物倫理委員會批準,按照國際動物實驗標準執行。
主要設備及試劑:手術顯微鏡(LZL-6A型,鎮江中天公司);光學顯微鏡(BH-3型,Olympus公司);電子分析天平(ESJ200-4±0.0001 g);他克莫司(Tacrolimus)100 mg(Selleck);Masson三色染色試劑盒(標準型,江蘇KeyGEN生物);Peroxidase來源于辣根100 mg(Sigma)。
1.2造模方法
1.2.1造模? 禁食水4 h,術前30 min,肌肉注射頭孢唑啉鈉(魯抗制藥,20180120)10 mg/100 g預防感染,術區備皮剪毛。10%水合氯醛按照0.35 ml/100 g進行腹腔全麻;A1組和A2組:消毒,沿頭部正中矢狀切開,在顱骨冠狀線后1.5 mm、中線偏左5 mm處開直徑5 mm骨窗,撞擊造成中度腦損傷;右側臀部,顯微鏡下完全切斷坐骨神經,9-0無損傷線縫合坐骨神經外膜4~6針[11]。B1組和B2組:大鼠僅于顯微鏡下完全切斷右側坐骨神經,縫合坐骨神經外膜。
1.2.2造模后干預? 分籠飼養在同樣環境中。他克莫司用0.9%氯化鈉稀釋,1 ml 0.9%氯化鈉+1 mg他克莫司,現用現配制,4℃恒溫保存;造模手術12 h后,A1組大鼠給予他克莫司,按1 mg/200 mg腹腔注射;A2組給予生理鹽水,按 1 ml/200 mg腹腔注射;B1組大鼠給予他克莫司,按1 mg/200 mg腹腔注射;B2組大鼠給予生理鹽水,按1 ml/200 mg腹腔注射。1次/d,連續2周。觀察各組大鼠存活情況。
1.3觀察指標
1.3.1坐骨神經指數(sciatic nerve function index,SFI)的測量? 分別于造模后第4、8、12周,各組每次隨機取10只大鼠。根據Schiaveto de Souza A的方法[8],實驗側足3個參數分別為:實驗側足印長度(SPL)、實驗側足趾寬度(STS)、實驗側中間足趾距離(SIT);正常側足3個參數分別為正常側足印長度(ZPL)、正常側足趾寬度(ZTS)、正常側中間足趾距離(ZIT)。SFI=-38.3×(SPL-ZPL)/ZPL+109.5×(STS-ZTS)/ZTS+13.2×(SIT-ZIT)/ZIT-8.8。以SFI值0時為正常,-100時為神經完全斷離。
1.3.2腓腸肌恢復率? 造模后第4、8、12周,各組隨機取5只大鼠,取下完整的雙側腓腸肌,吸取肌肉周圍的血液,雙側腓腸肌在分析天平上稱重。計算腓腸肌的恢復率,推測運動功能恢復的情況。
1.3.3神經Masson染色? 造模后第4、8、12周,各組隨機取5只大鼠,切取吻合口遠、近端0.5 cm坐骨神經,10%甲醛固定,梯度酒精脫水,石蠟包埋,切片厚度5 μm,染色、封片,光學顯微鏡下觀察神經纖維、膠原纖維增生情況。
1.3.4辣根過氧化物酶(HRP)示蹤? 分別于造模后第8、12周,于坐骨神經斷端以遠0.5 cm處,注入30%HRP溶液5 μl。深麻醉下開胸,灌流固定,取坐骨神經相應脊髓節段,橫斷面連續振蕩切片30 μm。光鏡下統計脊髓前角運動神經元中被標記為藍染顆粒的胞體數目。
1.4統計學方法
采用SPSS 19.0統計學軟件進行數據分析,計量資料用均數±標準差(x±s)表示,兩組間比較采用t檢驗,以P<0.05為差異有統計學意義。
2結果
2.1造模后各組大鼠基本生活狀態的觀察
造模后所有動物均存活,未發現切口感染情況。造模手術后5 d,B2組大鼠出現足部紅腫明顯,其他組紅腫較輕;3周后,A2、B1、B2組大鼠足跟出現程度不同的潰瘍面,A1組大鼠足部未見明顯潰瘍;12周時,各組大鼠足部潰瘍基本痊愈,B2組大鼠出現足部的自食現象。
2.2各組大鼠造模后第4、8、12周SFI的比較
暗箱測試結果顯示,造模后第4周,A1組與A2組、B1組與B2組的SFI比較,差異無統計學意義(P>0.05);造模后第4周,A1、A2組的SFI均優于B1、B2組,差異有統計學意義(P<0.01);造模后第8、12周,A2組與B1組的SFI比較,差異無統計學意義(P>0.05);造模后第8、12周,A1組的SFI優于A2、B1、B2組,A2、B1組的SFI均優于B2組,差異有統計學意義(P<0.01);4周后,各組大鼠的SFI逐漸升高(P<0.01)(表1)。
2.3各組大鼠造模后第4、8、12周腓腸肌恢復率的比較
4周后取材可見各組大鼠失神經支配的腓腸肌顏色均較健側蒼白,肌肉明顯萎縮。
造模后第4周,A2、B1、B2組的腓腸肌恢復率比較,差異無統計學意義(P>0.05);A1組造模后第4周的腓腸肌恢復率高于A2、B1、B2組,差異有統計學意義(P<0.01);造模后第8、12周,A1、A2、B1組的腓腸肌恢復率均明顯高于B2組,差異有統計學意義(P<0.01);造模后第8、12周,A1組與A2組的腓腸肌恢復率比較,差異無統計學意義(P>0.05);A1、A2組造模后第8周的腓腸肌恢復率均高于B1組,差異有統計學意義(P<0.01);造模后第12周,A1組的腓腸肌恢復率高于B1組,差異有統計學意義(P<0.01);A2組與B1組造模后第12周的腓腸肌恢復率比較,差異無統計學意義(P>0.05);4周后,各組大鼠的腓腸肌恢復率逐漸升高(P<0.01)(表2)。
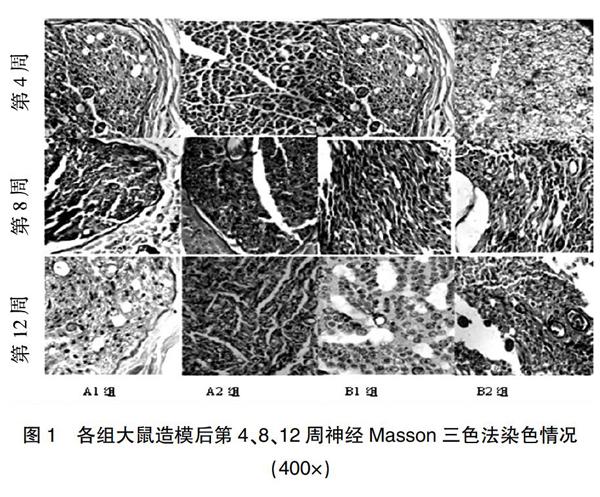
2.4各組大鼠造模后第4、8、12周神經Masson三色法染色情況
造模后第4周,A1、B1組神經纖維紅染較多,綠色纖維較少,A2組綠染與紅染均勻,B2組未見紅染的神經纖維;造模后第8周,A1、A2、B1組可見綠染與紅染均勻分布,B2組可見再生的軸突;造模后第12周,A1組膠原纖維均勻分布,并呈波浪形隨神經纖維排列,A2、B1組可見綠染與紅染分布均勻,B2組可見大量膠原纖維,少量再生的軸突(圖1)。
2.5各組大鼠造模后第8、12周神經元HRP標記情況
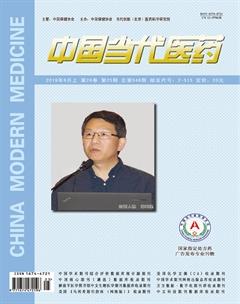
光鏡下,相應脊髓節段的前角神經元細胞胞漿中發現標記成藍黑色的HRP陽性顆粒細胞(圖2)。
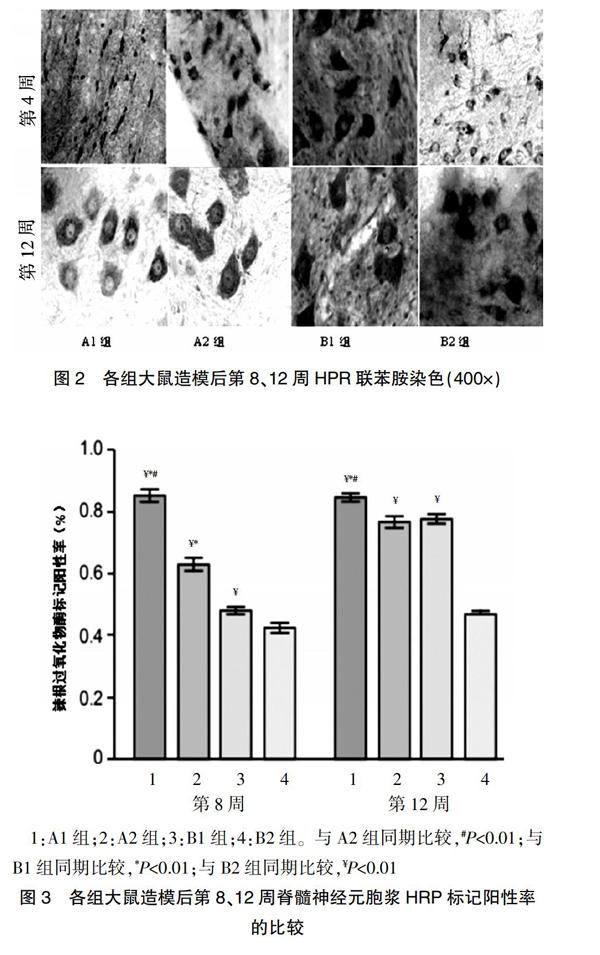
每高倍視野下進行計數,統計分析結果顯示,造模后第8周,A1組的HRP標記陽性率高于A2、B1、B2組,A2組的HRP標記陽性率高于B1、B2組,B1組的HRP標記陽性率高于B2組,差異有統計學意義(P<0.01);造模后第12周,A1組的HRP標記陽性率高于A2、B1、B2組,A2、B1組的HRP標記陽性率均高于B2組,差異有統計學意義(P<0.01);A2組造模后第12周的HRP標記陽性率與B1組比較,差異無統計學意義(P>0.05)(圖3)。
1:A1組;2:A2組;3:B1組;4:B2組。與A2組同期比較,#P<0.01;與B1組同期比較,*P<0.01;與B2組同期比較,¥P<0.01
3討論
何新澤等[1,22-33]動物實驗發現,大鼠腦損傷后對損傷的坐骨神經修復重建有明顯促進作用,但具體修復機制尚不清楚。本研究通過動物實驗比較顱腦損傷聯合應用他克莫司的坐骨神經損傷大鼠,損傷后的坐骨神經損傷恢復的情況。在所有的實驗觀測項目中,顱腦損傷聯合他克莫司(A1組)的坐骨神經修復效果優于其他組(P<0.05),提示顱腦損傷可以與他克莫司協同促進坐骨神經損傷后的修復,其作用機制與他克莫司不完全相同。
在Sunderland V型的外圍神經損傷后,神經損傷切斷了神經內分泌的養分,不能將其輸送到靶子器官上,靶子器官將失去活性和營養的支持。根據目前的他克莫司促進神經機制,促進外圍神經修復相對明確是兩個功能領域,發揮神經營養功能,形成一個FKBP12的綜合體,加入功能地區后表達GAP-43,一個超蛋白質神經生長,并促進形成和擴大神經的生長由神經脈沖生成的生物電能、靶器官,再生軸突的內徑上升,厚厚的神經膜層,作用范圍增加[22-23]。這證實了他克莫司有助于恢復外圍神經的營養功能,萎縮身體的部分看起來更容易潰瘍,顱腦損傷聯合他克莫司組恢復較好,提示促進外形神經損傷的作用,結合功能或復雜的FKBP12地區來促進表達GAP-43。
在外圍神經損傷后,軸突的退化立即發生,軸突碎片是由巨噬細胞吞噬清除,新的軸突、未退化的神經元延伸到由Schwann細胞組成的內膜神經的間隙,靶器官逐漸建立聯系和營養[22-29]。Masson染色、HRP切片神經均顯示,A1組在他克莫司的免疫抑制效果方面優于其他組(P<0.05),他克莫司結合FKBP12,形成鈣復合物抑制堿(CAN),抑制T細胞的衰減,并抑制白介素-2(IL-2)、白介素-3(IL-3)的表達,以生產免疫抑制物被神經接收[6-11]。
周圍神經的損傷伴隨著血液神經屏障的破壞,刺激纖維增生和巨噬細胞的擴散,形成影響神經修復的瘢痕[24-25]。他克莫司可以抑制纖維素的擴散、遷移和生物活性,抑制纖維素的擴散,并通過免疫抑制作用促進神經損傷的重建和修復。Masson染色觀察結果提示,A1組的瘢痕比A2、B1、B2組減少。神經內分泌系統的調節,創造微型環境的因素、Schwann細胞的信號有助于促進軸突再生[28-29]。神經交換的物質是軸漿的運輸器官和再生軸芽器官通過內膜管再生作用于目標器官[25-29]。軸突內物質更好地恢復運輸功能和靶器官的反饋是相互促進的[12-17]。HRP染色結果進一步提示,免疫神經內分泌系統在腦損傷期間有密切的關系[30],自主神經系統的中心結構被摧毀,導致免疫調節紊亂、改變或喪失,功能腦細胞的變性,導致caspase瀑布反應性的激活,導致神經凋亡。
綜上所述,腦損傷伴隨周圍神經損傷動物早期應用他克莫司后,周圍神經修復再生方面較好,腦損傷、他克莫司均可促進周圍神經損傷的修復,并且協同促進神經損傷的修復效果更好,為腦損傷合并周圍神經損傷的患者提供了新的治療思路。但腦損傷促進周圍神經損傷的具體機制仍需進一步深入研究。
[參考文獻]
[1]何新澤,王維,馬建軍,等.顱腦損傷促進的坐骨神經再生[J].中國組織工程研究,2016,20(27):4061-4067.
[2]Wang W,Gao J,Na L,et al.Craniocerebral injury promotes the repair of peripheral nerve injury[J].Neural Regen Res,2014,9(18):1703-1708.
[3]Reeves TM,Trimmer PA,Colley BS,et al.Targeting Kv1.3 channels to reduce white matter pathology after traumatic brain injury[J].Expe Neurol,2016,283(PtA):188-203.
[4]Mohammadi R,Vahabzadeh B,Amini K.Sciatic nerve regeneration induced by transplantation of in vitro bone marrow stromal cells into an inside-out artery graft in rat[J].J Craniomaxillofac Surg,2014,42(7):1389-1396.
[5]Glaus SW,Johnson PJ,Mackinnon SE.Clinical strategies to enhance nerve regeneration in composite tissue allotransplantation[J].Hand Clin,2011,27(4):495-509.
[6]Mekaj AY,Morina AA,Manxhuka-Kerliu S,et al.Electrophysiological and functional evaluation of peroneal nerve regeneration in rabbit following topical hyaluronic acid or tacrolimus application after nerve repair[J].Niger Postgrad Med J,2015,22(3):179-184.
[7]Badavanis G,Pasmatzi E,Monastirli A,et al.Topical imiquimod is an effective and safe drug for molluscum contagiosum in children[J].Acta Dermatovenerol Croat,2017,25(2):164-166.
[8]Phillips BZ,Franco MJ,Yee A,et al.Direct radial to ulnar nerve transfer to restore intrinsic muscle function in combined proximal median and ulnar nerve injury:case report and surgical technique[J].J Hand Surg Am,2014,39(7):1358-1362.
[9]Zhao J,Zheng X,Fu C,et al.FK506-loaded chitosan conduit promotes the regeneration of injured sciatic nerves in the rat through the upregulation of brain-derived neurotrophic factor and TrkB[J].J Neurol Sci,2014,344(1-2):20-26.
[10]Gaudier-Diaz MM,Haines AH,Zhang N,et al.Social influences on microglial reactivity and neuronal damage after cardiac arrest/cardiopulmonary resuscitation[J].Physiol Behav,2018,194:437-449.
[11]Cheng XL,Wang P,Sun B,et al.The longitudinal epineural incision and complete nerve transection method for sciatic nerve injury[J].Neural Regen Res,2015,10(10):1663-1668.
[12]Dai Y,Wang C,Chiu LY,et al.Application of bioconjugation chemistry on biosensor fabrication for detection of TAR-DNA binding protein 43[J].Biosens Bioelectron,2018,117:60-67.
[13]何新澤,王成剛,于立志,等.他克莫司促進周圍神經再生的研究進展[J].轉化醫學電子雜志,2018,5(12):102-104.
[14]He L,Yadgarov A,Sharif S,et al.Aging profoundly delays functional recovery from gustatory nerve injury[J].Neuroscience,2012,209:208-218.
[15]Huang CC,Yang W,Guo C,et al.Anatomical and functional dichotomy of ocular itch and pain[J].Nat Med,2018,24(8):1268-1276.
[16]何新澤,于立志,王成剛,等.跟腓韌帶損傷的診療進展[J].足踝外科電子雜志,2018,5(2):59-61.
[17]Saeman MR,DeSpain K,Liu MM,et al.Effects of exercise on soleus in severe burn and muscle disuse atrophy[J].J Surg Res,2015,198(1):19-26.
[18]Shu B,Xie JL,Xu YB,et al.Effects of skin-derived precursors on wound healing of denervated skin in a nude mouse model[J].Int J Clin Exp Pathol,2015,8(3):2660-2669.
[19]Dong HY,Jiang XM,Niu CB,et al.Cerebrolysin improves sciatic nerve dysfunction in a mouse model of diabetic peripheral neuropathy[J].Neural Regen Res,2016,11(1):156-162.
[20]Khosravi A,Sharifi I,Tavakkoli H,et al.Embryonic toxico-pathological effects of meglumine antimoniate using a chick embryo model[J].PLoS One,2018,13(5):e0196424.
[21]Lin Q,Wesson RN,Maeda H,et al.Pharmacological mobilization of endogenous stem cells significantly promotes skin regeneration after full-thickness excision:the synergistic activity of AMD3100 and tacrolimus[J].J Invest Dermatol,2014,134(9):2458-2468.
[22]Florio F,Ferri C,Scapin C,et al.Sustained expression of negative regulators of myelination protects schwann cells from dysmyelination in a charcot-marie-tooth 1B mouse model[J].J Neurosci,2018,38(18):4275-4287.
[23]Croaker A,King GJ,Pyne JH,et al.Assessing the risk of epidemic dropsy from black salve use[J].J Appl Toxicol,2018, 38(10):1274-1281.
[24]Roque JS,Pomini KT,Buchaim RL,et al.Inside-out and standard vein grafts associated with platelet-rich plasma(PRP)in sciatic nerve repair.A histomorphometric study[J].Acta Cir Bras,2017,32(8):617-625.
[25]Ganguly S,Das P,Maity PP,et al.Green reduced graphene oxide toughened semi-IPN monolith hydrogel as dual responsive drug release system:rheological,physicomechanical,and electrical evaluations[J].J Phys Chem B,2018,122(29):7201-7218.
[26]Liu C,Yang H,Shi W,et al.MicroRNA-mediated regulation of Th17/Treg balance in autoimmune disease[J].Immunology,2018,155(4):427-434.
[27]Starr A,Sattler R.Synaptic dysfunction and altered excitability in C9ORF72 ALS/FTD[J].Brain Res,2018,1693(PtA):98-108.
[28]Quan Wang J,Di Yang M,Chen X,et al.Discovery of new chromen-4-one derivatives as telomerase inhibitors through regulating expression of dyskerin[J].J Enzyme Inhib Med Chem,2018,33(1):1199-1211.
[29]Liu S,Wu N,Miao J,et al.Protective effect of morin on myocardial ischemia reperfusion injury in rats[J].Int J Mol Med,2018,42(3):1379-1390.
[30]Kentner AC,Khan U,MacRae M,et al.The effect of antibiotics on social aversion following early life inflammation[J].Physiol Behav,2018,194:311-318.
[31]馬建軍,何新澤,王浩琪,等.不同位置腦損傷模型大鼠坐骨神經的再生[J].中國組織工程研究,2017,21(36):5806-5811.
[32]He XZ,Ma JJ,Wang HQ,et al.Brain injury in combination with tacrolimus promotes the regeneration of injured peripheral nerves[J].Neural Regen Res,2017,12(6):987-994.
[33]何新澤,王維,呼鐵民,等.周圍神經損傷的修復:理論研究與技術應用[J].中國組織工程研究,2016,20(7):1044-1050.
(收稿日期:2019-03-29? 本文編輯:任秀蘭)