兩種治療方案對支架內再狹窄患者冠脈造影效果及臨床事件發生風險的影響
2019-11-09 20:27:48余小妹楊棟周莉陳宇凱王明偉
中國現代醫生 2019年23期
余小妹 楊棟 周莉 陳宇凱 王明偉
[摘要] 目的 探討藥物洗脫球囊和藥物洗脫支架對支架內再狹窄患者冠脈造影效果及臨床事件發生風險的影響。方法 選取我院2015年1月~2016年12月收治支架內再狹窄患者共100例為研究對象,根據治療方案差異隨機分為A組(50例)和B組(50例),A組患者采用藥物洗脫支架治療,B組患者采用藥物洗脫球囊方案治療;比較兩組患者術后隨訪晚期管腔丟失量、二次再狹窄率、Mehran再狹窄分型及臨床事件發生率。 結果 兩組患者晚期管腔丟失量比較,B組晚期管腔丟失量較A組更少(P<0.05),兩組二次再狹窄率比較,差異無統計學意義(P>0.05);兩組患者Mehran再狹窄分型情況比較,差異無統計學意義(P>0.05);兩組患者臨床事件發生率比較,差異無統計學意義(P>0.05)。 結論 藥物洗脫球囊治療支架內再狹窄總體療效不遜于藥物洗脫支架,具有臨床應用價值。
[關鍵詞] 藥物洗脫球囊;藥物洗脫支架;支架內再狹窄;冠脈造影效果;臨床事件
[中圖分類號] R543? ? ? ? ? [文獻標識碼] A? ? ? ? ? [文章編號] 1673-9701(2019)23-0015-04
[Abstract] Objective To investigate the effects of drug-eluting balloon and drug-eluting stent on coronary angiography and risk of clinical events in patients with in-stent restenosis. Methods A total of 100 patients with in-stent restenosis were enrolled in our hospital from January 2015 to December 2016. They were randomly divided into group A (50 cases) and group B(50 cases) according to the treatment plan, and the group A was treated with eluting stents, the group B was treated with drug-eluting balloon. The late lumen loss, secondary restenosis rate, Mehran restenosis classification, and clinical event rate were compared between the two groups during the postoperative follow-up. Results The amount of late luminal loss in group B was significantly less than that in the group A(P<0.05). There was no significant difference in the rate of secondary restenosis between the two groups(P>0.05).There was no significant difference in the classification of Mehran restenosis between the two groups(P>0.05). There was no significant difference in the incidence of clinical events between the two groups(P>0.05). Conclusion The drug-eluting balloon is not inferior to the drug-eluting stent in the treatment of in-stent restenosis, and has clinical application value.
[Key words] Drug-eluting balloon; Drug-eluting stent; In-stent restenosis; Coronary angiography effect; Clinical event
支架內再狹窄是行經皮冠脈介入治療術(percutaneous coronary intervention,PCI)后亟需解決問題之一,近年來研究顯示,藥物洗脫球囊通過將球囊成形和藥物洗脫技術相結合,輸送球囊導管達病變血管壁內,可達到抑制平滑肌增生和降低狹窄程度的目的[1-2]。但對于支架內再狹窄防治藥物洗脫球囊應用仍存在一定爭議,不同回顧性研究間結論存在較大差異;部分學者報道其與藥物洗脫支架應用比較具有相近臨床療效[3];而另一項研究則表明藥物洗脫支架應用在治療支架內再狹窄方面更具優勢[4]。本文旨在探討藥物洗脫球囊和藥物洗脫支架對支架內再狹窄患者冠脈造影效果及臨床事件發生風險的影響,為治療方案選擇提供相應循證依據,現報道如下。
1 資料與方法
1.1 一般資料
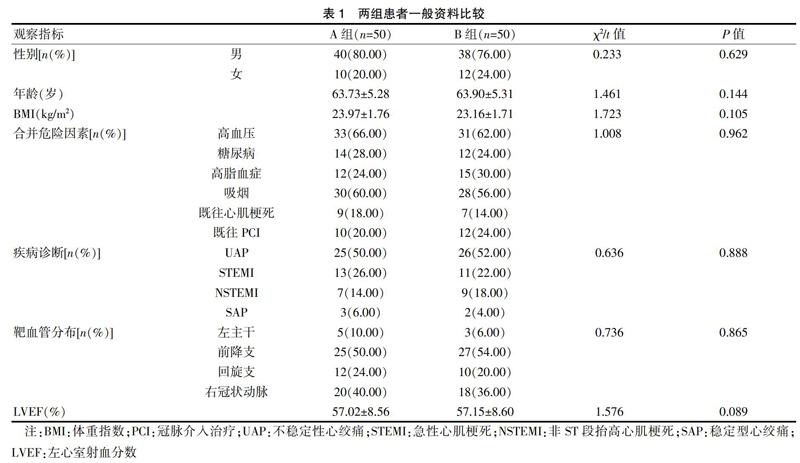
選取我院2015年1月~2016年12月收治的支架內再狹窄患者共100例為研究對象,根據治療方案差異分為A組(藥物洗脫支架組)和B組(藥物洗脫球囊組),每組50例;兩組患者一般資料比較,差異無統計學意義(P>0.05)。見表1。
1.2 納入標準
①既往行裸金屬支(bare metal stent,BMS)或藥物洗脫支架(drug-eluting stent,DES)治療,復查見單支血管再狹窄;②年齡≥18歲;③符合球囊和支架置入適應證;④方案經醫院倫理委員會批準,且患者及家屬知情同意。
1.3 排除標準
①急性心肌梗死病程<48 h;②腎小球濾過率(GFR)<30 mL/min;③心力衰竭分級(New York Heart Association分級,NYHA分級)Ⅳ級;④研究藥物過敏;⑤凝血功能障礙、外周動脈疾病及腦卒中;⑥臨床資料不全。
1.4 治療方法
全部患者術前3 d給予阿司匹林(拜耳醫藥,100 mg,J20080078)100 mg/d,氯吡格雷(賽諾菲制藥,75 mg,J20130083)75 mg/d,口服;術中給予肝素(北京賽生藥業,1.25萬單位/支,H11020362)80~100 U/kg靜脈滴注,保證活化凝血時間維持在200~250 s;根據治療方法的不同隨機分為A組和B組。
A組患者采用DES治療,支架為美敦力醫療器械有限公司生產。DES治療方法:造影明確狹窄部位后,工作角度下首先使用普通冠脈球囊預擴張,冠脈球囊直徑一般小于狹窄兩端正常血管直徑0.5 mm,長度應該完全覆蓋狹窄段;DES一般與狹窄兩端正常血管直徑相同,長度應超出狹窄兩端1~2 mm,支架球囊充盈30 s。B組患者則采用藥物洗脫球囊(drug-eluting balloon,DEB)治療,DEB德國貝朗醫療有限公司生產,紫杉醇載藥量3 μg/mm2。DEB治療方法:使用普通冠脈球囊進行預擴張,球囊與狹窄兩端正常血管直徑比率0.8~1.0;普通球囊擴張后使用DEB進行擴張,一般DEB直徑與普通冠脈球囊相同,長度要比狹窄兩端各長1~2 mm,并且要完全覆蓋狹窄段,一般DEB貼壁擴張持續30~60 s,擴張后再次造影觀察狹窄解除情況。
1.5 觀察指標
①術后6個月行冠狀動脈造影記錄晚期管腔丟失量,計算平均值。②記錄患者術后6個月二次再狹窄例數,計算百分比。③根據Mehran分型,將支架內再狹窄分為4型[5]:Ⅰ型為局部型,支架內狹窄長度≤10 mm;Ⅱ型為彌漫型,支架內狹窄長度>10 mm;Ⅲ型為增生型,支架內狹窄長度>10 mm并超過支架邊緣;Ⅳ型為閉塞型,即支架內完全閉塞。④記錄患者術后隨訪心源性死亡、心肌梗死、靶血管血運重建、靶病變血運重建及主要不良心臟事件(major adverse cardiac events,MACE)例數,計算百分比。
1.6 統計學方法
數據分析選擇SPSS18.0軟件,計量資料采用t檢驗,進行檢驗前先進行正態性檢驗及方差齊性檢驗,若非正態分布或方差不齊,則采用秩和檢驗;計數資料采用χ2檢驗或精確概率法檢驗;等級資料采用秩和檢驗;P<0.05為差異有統計學意義。
2 結果
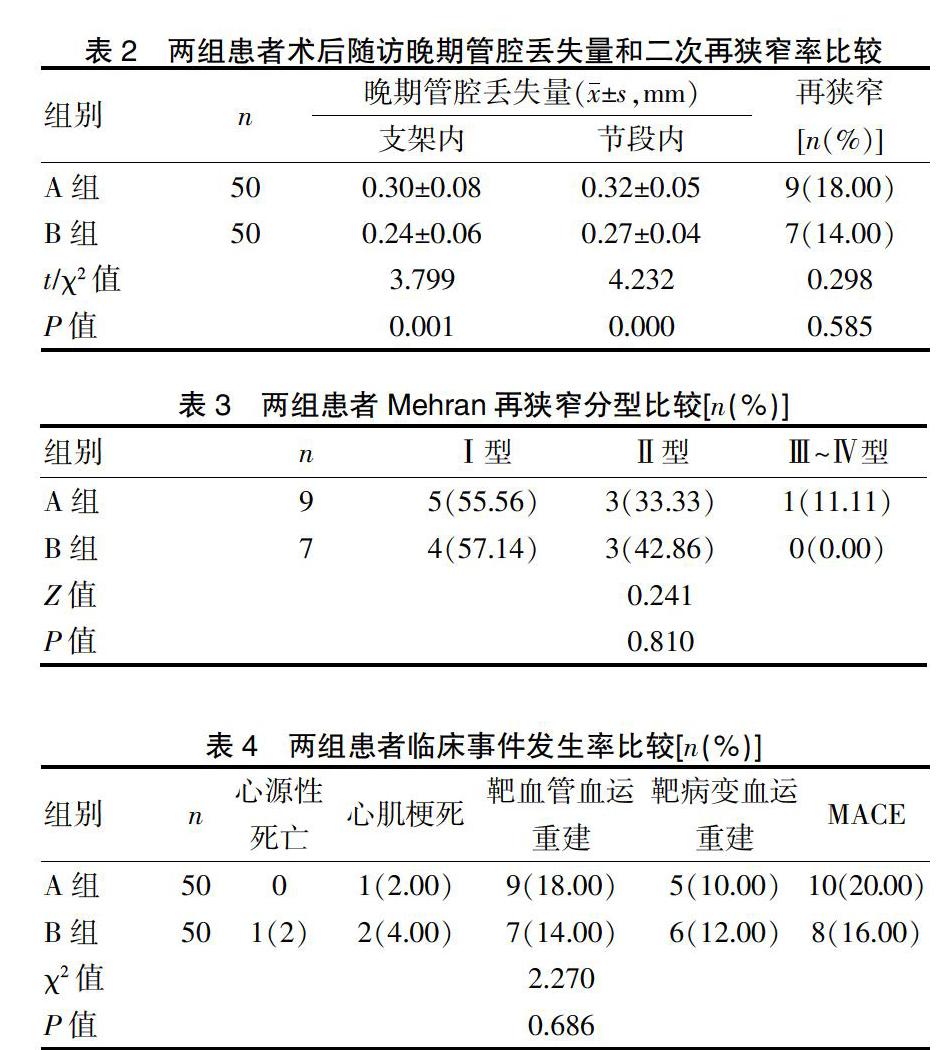
2.1 兩組患者術后隨訪晚期管腔丟失量和二次再狹窄率比較
兩組患者晚期管腔丟失量比較,無論是支架內還是節段內,B組晚期管腔丟失量較A組更少(P<0.05);但兩組二次再狹窄率比較,差異無統計學意義(P>0.05)。見表2。
2.2 兩組患者Mehran再狹窄分型比較
兩組患者Mehran再狹窄分型情況比較,差異無統計學意義(P>0.05)。見表3。
2.3 兩組患者臨床事件發生率比較
兩組患者臨床事件發生率比較,差異無統計學意義(P>0.05)。見表4。
3 討論
PCI術是急性冠脈綜合征患者首選治療方案之一,在延長生存時間的同時亦顯著提高生活質量;但大量隨訪報道顯示,患者術后極易出現支架再狹窄問題,嚴重影響遠期預后改善[6]。目前醫學界研究顯示,支架內在狹窄發生機制較為復雜,可能原因包括[7-8]:①支架置入時對血管內膜造成損傷,部分中膜撕裂后可暴露內皮下組織,誘導血小板局部吸附聚集及血栓形成,而此類血栓可通過后續基質和膠原合成,加快新生內膜形成速率,最終導致支架內再狹窄發生;②支架置入導致的血管損傷還可激活外周循環中有絲分裂原,提高血小板功能,刺激平滑肌細胞增殖,而平滑肌細胞過度增殖已被證實是導致支架內再狹窄發生的關鍵原因;③支架進入人體后異物刺激可加重局部血管炎性反應,引起巨噬細胞聚集和內皮損傷進展。國外學者研究顯示,前降支支架植入后較其他血管更易誘發再狹窄發生,這可能與血管解剖結構、血流與血管壁間剪切力形成等密切相關[9]。
目前臨床對于支架再狹窄患者治療方案選擇尚存在較大爭議,藥物洗脫球囊應用能否達到藥物洗脫支架相近或者更加良好的臨床療效并無明確定論。紫杉醇DEB含有紫杉醇混合對比劑,可通過攜帶的紫杉醇藥物抑制血管內膜增生,減少ISR 發生率[10]。藥物球囊藥物洗脫球囊近年來被逐漸應用于支架內再狹窄治療,并取得令人滿意效果[11];其中含有紫杉醇藥物成分能夠有效抑制血管內膜增生,降低再狹窄發生風險;同時其還能夠解決支架置入后膨脹不良所引起再狹窄問題,避免多層重疊支架植入[12];此外相較于藥物洗脫支架,藥物洗脫球囊應用后能夠預防因支架藥物不均勻可能誘發內皮化延遲和晚期血栓發生。但藥物洗脫球囊難以解決急性期病變血管彈性回縮、置入后嚴重夾層形成可能等問題[13]。
國外學者研究顯示[14],藥物洗脫球囊治療支架內再狹窄患者總體療效優于普通球囊,隨訪6個月后晚期管腔丟失量更少;而另一項前瞻性研究則提示[15],藥物洗脫球囊與藥物洗脫支架在晚期管腔丟失控制方面效果相當。Habara S等[16]最新注冊研究結果提示,治療DES植入術后ISR 晚期管腔丟失明顯優于DES 組;兩組術后1 年MACE 發生率差異無統計學意義。國內學者在對比藥物球囊和藥物洗脫支架在治療支架內狹窄的中心臨床試驗中顯示,臨床隨訪1年和2年的臨床事件發生率均較藥物洗脫支架低[17-19]。本研究結果中,兩組患者二次再狹窄率比較,差異無統計學意義(P>0.05);兩組患者Mehran再狹窄分型情況比較,差異無統計學意義(P>0.05),證實與藥物洗脫支架相比,藥物洗脫球囊治療支架內再狹窄在避免再次狹窄和促進血管再通方面效果接近;同時兩組患者臨床事件發生率比較,差異無統計學意義(P>0.05),表明藥物洗脫球囊用于支架內再狹窄患者治療安全性值得認可,與以往報道結果相一致[20]。
本研究顯示,藥物洗脫球囊治療支架內再狹窄總體療效不遜于藥物洗脫支架,具有臨床應用價值。當然,本研究為單中心研究,并且樣本量較小,需要更大樣本量的多中心研究才能取得更可靠的結果。
[參考文獻]
[1] Han Y,Xu B,Jing Q,et al. A randomized comparison of novel biodegradable polymer-and durable polymer-coated cobaltchromium sirolimus-eluting stents[J]. JACC Cardiovasc Interv,2014,7(12):1352-1360.
[2] Zhu L,Lv YN,Wang LY. Stent thrombosis with biodegradable polymer drug-eluting stents versus durable polymer sirolimus-eluting stents:an update meta-analysis[J]. Cardiology,2015,130(2):96-105.
[3] De la Torre Hernandez JM,Alfonso F,Sanchez Recalde A,et al. Comparison of paclitaxel-eluting stents (Taxus) and everolimus-eluting stents(Xience) in left main coronary artery disease with 3 years follow-up (from the ESTROFA-LM registry)[J]. Am J Cardiol,2013,111(4):676-683.
[4] Conrotto F,Scacciatella P,D'Ascenzo F,et al. Long-term outcomes of percutaneous coronary interventions or coronary artery bypass grafting for left main coronary artery disease in octogenarians(from a drug-eluting stent for left main artery registry substudy)[J]. Am J Cardiol,2014,113(4):2007-2012.
[5] Mehran R,Dangas G,Abizaid A,et al. Angiographic Patterns of In-Stent Restenosis:Classification and Implications for Long-Term Outcome[J]. Circulation,1999,100(18):1872-1878.
[6] Naganuma T,Chieffo A,Takagi K,et al. First generation versus new generation drug-eluting stents for the treatment of ostial/midshaft lesions in unprotected left main coronary artery:The Milan and New-Tokyo(MITO)registry[J]. Catheter Cardiovasc Interv,2015,85(3):E63-E69.
[7] Athappan G,Patvardhan E,Tuzcu ME,et al. Left main coronary artery stenosis: a meta-analysis of drug-eluting stents versus coronary artery bypass grafting[J]. JACC Cardiovasc Interv,2013,33(6):1219-1230.
[8] Tada T,Byrne RA,Cassese S,et al. Comparative efficacy of 2 zotarolimus-eluting stent generations: resolute versus endeavor stents in patients with coronary artery disease[J]. Am Heart J,2013,165(4):80-86.
[9] Sen H,Lam MK,Tandjung K,et al. Complex patients treated with zotarolimus-eluting resolute and everolimus-eluting xience V stents in the randomized TWENTE trial:Comparison of 2-year clinical outcome[J]. Catheter Cardiovasc Interv,2015,85(4):74-81.
[10] 張文俐,杜潤,朱政斌,等.藥物洗脫球囊抑制下肢動脈狹窄性病變的實驗研究[J].介入放射學雜志,2014,23(5):423-426.
[11] Lee JM,Park KW,Han JK,et al. Three-year patient-related and stent-related outcomes of second-generation everolimus-eluting Xience V stents versus zotarolimus-eluting resolute stents in real-world practice(from the Multicenter Prospective EXCELLENT and RESOLUTE-Korea Registries)[J]. Am J Cardiol,2014,114(6):1329-1338.
[12] Cho SC,Jeong MH,Kim W,et al. Clinical outcomes of everolimus-and zotarolimus-eluting stents in patients with acute myocardial infarction for small coronary artery disease[J]. J Cardiol,2014,63(3):409-417.
[13] Bernelli C. Drug-eluting stents in unprotected left main coronary artery disease[J]. Expert Rev Cardiovasc Ther,2014,12(5):1349-1368.
[14] Buszman PP,Orlik B,Trela B,et al. Comparable clinical safety and efficacy of biodegradable versus durable polymer paclitaxel eluting stents despite shorter dual antiplatelet therapy:insights from a multicenter, propensity score-matched registry[J]. Catheter Cardiovasc Interv,2013,82(3):155-162.
[15] Serruys PW,Farooq V,Kalesan B,et al. Improved safety and reduction in stent thrombosis asociated with biodegradable polymer-based biolimus-eluting stents versus durable polymer-based sirolimus-eluting stents in patients with coronary artery disease:final 5-year report of the LEADERS(Limus Eluted From A Durable Versus ERodable Stent Coating)randomized,noninferiority trial[J].JACC Cardiovasc Interv,2013,6(7):777-789.
[16] Habara S,Kadota K,Kanazawa T,et al. Paclitaxel-coated balloon catheter compared with drug-eluting stent for drug-eluting stent restenosis in routine clinical practice[J].Euro Intervention,2016,11(10):1098-1105.
[17] Xu B,Gao R,Wang J,et al. A prospective,multicenter,randomized trial of paclitaxel-coated balloon versus paclitaxel-eluting stent for the treatment of drug-eluting stent in-stent restenosis:results from the PEPCAD China ISR trial[J]. JACC Cardiovasc Interv,2014,7(2):204-211.
[18] 崔孔勇,呂樹錚,柳弘,等.紫杉醇藥物洗脫球囊與西羅莫司藥物洗脫支架治療再狹窄的比較[J]. 心肺血管病雜志,2016,35(7):499-504.
[19] 曾書燚,王正東,陳堅,等.藥物洗脫球囊與藥物洗脫支架治療支架內再狹窄療效比較[J].介入放射學雜志,2017, 26(9):839-842.
[20] 曾書■,王正東,陳堅,等.藥物洗脫球囊與藥物洗脫支架治療支架內再狹窄療效比較[J].介入放射學雜志,2017,26(9):839-842.
(收稿日期:2018-10-25)
