學齡前兒童骨密度與血清25-(OH)D水平的相關性
2019-09-07 07:55:51邢存喬陳海瓊曾廣萍
中國醫藥導報
2019年17期
邢存喬 陳海瓊 曾廣萍

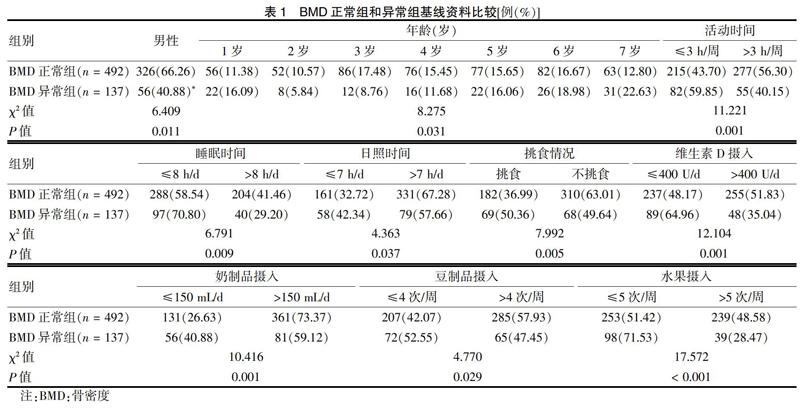
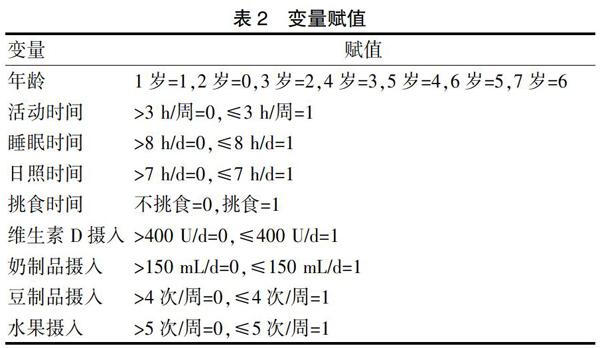
[摘要] 目的 調查學齡前兒童骨密度(BMD)狀況及其與血清25-羥維生素D[25-(OH)D]的關系。 方法 收集2017年3月~2018年3月629例在三亞市婦幼保健院兒童保健科門診體檢行BMD檢查的0~7歲學齡前兒童為研究對象,采用定量超聲儀測量BMD,根據BMD水平將研究對象分為BMD正常組(n = 492)和BMD異常組(n = 137)。采用多因素Logistic回歸分析法分析學齡前兒童BMD的影響因素;采用酶聯免疫吸附法測定25-(OH)水平,比較不同25-(OH)D水平兒童的BMD,并采用Pearson積矩相關分析學齡前兒童BMD與血清25-(OH)D相關性。 結果 學齡前兒童BMD異常率為21.78%。5~7歲兒童BMD異常率較高,1歲兒童其次。女童、1歲及5~7歲兒童BMD異常率高于男童、2~4歲兒童(P < 0.05);活動時間≤3 h/周、睡眠時間≤8 h/d、日照時間≤7 h/d的學齡前兒童BMD異常率高于活動時間>3 h/周、睡眠時間>8 h/d、日照時間>7 h/d兒童(P < 0.05);挑食、維生素D攝入≤400 U/d、奶制品攝入≤150 mL/d、豆制品攝入≤4次/周、水果攝入≤5次/周的學齡前兒童BMD異常率高于不挑食、維生素D攝入>400 U/d、奶制品攝入>150 mL/d、豆制品攝入>4次/周、水果攝入>5次/周兒童(P < 0.05)。與2歲兒童比較,1歲、5~7歲是BMD異常的獨立危險因素(OR = 1.113、1.373、1.433、1.479,P < 0.05),活動時間、睡眠時間、日照時間、挑食情況、維生素D攝入、奶制品攝入、豆制品攝入、水果攝入是學齡前兒童BMD異常的影響因素(OR = 1.377、1.654、1.642、1.525、1.788、1.598、1.384、1.443,P < 0.05)。隨著25-(OH)D水平的降低,SOS值逐漸增大,Z值逐漸減小,BMD異常率逐漸增加(P < 0.05)。學齡前兒童SOS與血清25-(OH)D呈負相關(r = -0.729,P < 0.05),Z值與血清25-(OH)D呈正相關(r = 0.761,P < 0.05)。 結論 學齡前兒童BMD異常率較高,尤其多見于1歲以前及5~7歲兒童,對BMD異常高危兒童應合理補充維生素D和鈣劑,并加強戶外活動,注意飲食均衡。
[關鍵詞] 學齡前兒童;骨密度;25-羥維生素D;相關性
[中圖分類號] R179? ? ? ? ? [文獻標識碼] A? ? ? ? ? [文章編號] 1673-7210(2019)06(b)-0063-05
The correlation between bone mineral density and serum 25-(OH)D level in preschool children
XING Cunqiao? ?CHEN Haiqiong? ?CENG Guangping
Department of Child Health Care, Sanya City Womenfolk and Infant Health Care Hospital, Hainan Province, Sanya? ?572000, China
[Abstract] Objective To investigate the bone mineral density (BMD) in preschool children and its relationship with serum 25-hydroxyvitamin D [25-(OH)D]. Methods From March 2017 to March 2018, 629 preschool children aged 0-7 who underwent BMD examination in the Outpatient Department of Child Health Care of Sanya City Womenfolk and Infant Health Care Hospital were collected as subjects. BMD was measured by quantitative ultrasound, according to BMD level, the subjects were divided into normal BMD group (n = 492) and abnormal BMD group (n = 137). The influencing factor of BMD of preschool children was analyzed by multivariate Logistic regression analysis. The level of 25-(OH) was determined by ELISA, the BMD of children with different 25-(OH)D level was compared. Pearson product moment correlation analysis was used to analyze the correlation between BMD and serum 25-(OH)D in preschool children. Results The abnormal rate of BMD in preschool children was 21.78%, which in children aged 5-7 was higher than that in others, followed by children aged 1. The abnormal rate of BMD in girls, children aged 1-year-old and 5-7-year-old was higher than that in boys and children aged 2-4-year-old (P < 0.05). The abnormal rate of BMD in preschool children with activity time ≤3 h/week, sleeping time ≤8 h/d, sunshine time ≤7 h/d was higher than that of children whose activity time >3 h/week, sleeping time >8 h/d and sunshine time >7 h/d (P < 0.05). The abnormal rate of BMD in preschool children with picky diet, vitamin D intake ≤400 U/d, dairy intake ≤150 mL/d, bean products intake ≤4 times/week, fruit intake ≤5 times/week was higher than those of children without picky diet, vitamin D intake > 400 U/d, dairy intake >150 mL/d, bean products intake > 4 times/week, fruit intake > 5 times/week (P < 0.05). Compared with 2-year-old children, 1-year-old and 5-7-year-old was independent risk factors for abnormal BMD (OR = 1.113, 1.373, 1.433, 1.479, P < 0.05). Activity time, sleeping time, sunshine time, picky diet, vitamin D intake, dairy intake, bean products intake, fruit intake was the influencing factor of abnormal BMD in preschool children (OR = 1.377, 1.654, 1.642, 1.525, 1.788, 1.598, 1.384, 1.443, P < 0.05). With the decrease of 25-(OH)D level, SOS value increased gradually, Z value decreased gradually, and abnormal rate of BMD increased gradually (P < 0.05).There was a negative correlation between SOS and serum 25-(OH) D in preschool children (r = -0.729, P < 0.05), and a positive correlation between Z value and serum 25-(OH) D (r = 0.761, P < 0.05). Conclusion The abnormal rate of BMD in preschool children is higher, especially in children aged 1 and 5-7 years. Vitamin D and calcium should be supplemented reasonably for children at high risk of BMD, outdoor activities should be strengthened, and balanced diet should be paid attention to.
[Key words] Preschool children; Bone mineral density; 25-hydroxyvitamin D; Correlation
學齡前兒童期是機體新陳代謝、生長發育最活躍的階段,也是骨量增長、骨骼發育的時期,定量評估骨量可評估學齡前兒童生長發育進度[1]。骨密度(BMD),即骨骼礦物質密度,是指單位面積內骨礦物質的含量,是一項敏感且特異地反映人體骨營養狀況的指標,也是目前臨床評估骨鈣水平,反映人體骨質量常用的客觀指標[2]。調查發現[3],學齡期兒童BMD異常率可高達20%~30%,BMD降低的兒童更易出現骨折,同時患佝僂病的風險也明顯增加。維生素D參與調節鈣、磷代謝,對促進鈣吸收和重吸收及其在骨骼中的沉積具有重要作用,研究表明[4]。25-羥維生素D [25-(OH)D]是反映機體中維生素D營養狀態的敏感指標,檢測BMD可反映25-(OH)D水平,進而評估機體維生素D水平,但也有研究對此尚存爭議[5]。本研究通過檢測學齡前……
登錄APP查看全文
猜你喜歡
中老年保健(2022年5期)2022-08-24 02:36:04
中老年保健(2021年3期)2021-08-22 06:50:04
當代陜西(2021年12期)2021-08-05 07:45:46
天津醫科大學學報(2021年2期)2021-03-29 05:31:08
現代臨床醫學(2021年1期)2021-01-26 00:56:02
雜文選刊(2016年7期)2016-08-02 08:39:56
冰雪運動(2016年4期)2016-04-16 05:54:56
劍南文學(2015年1期)2015-02-28 01:15:15
現代檢驗醫學雜志(2014年4期)2014-02-02 02:44:59
記者觀察(2010年9期)2010-12-31 00:00:00
