診療流程的優化在改善缺血性腦卒中醫療質量中的作用
2019-07-31 02:50:12程景麗史樹海薛鐳
中國衛生產業 2019年12期
程景麗 史樹海 薛鐳
[摘要] 目的 急性缺血性腦卒中的治療有嚴格的時間窗限制,療效與開始溶栓治療的時間密切相關。該研究旨在通過優化診療流程方案,縮短診治時間,觀察該方案在急性缺血性腦卒中診療中的作用。方法 連續收集2017年3月—2018年5月就診的急性缺血性腦卒中患者,其中,2017年3—9月間的患者采用常規診療方案,2017年10月—2018年5月間的患者采用急診與病房聯動診療方案,比較兩組患者的一般情況、卒中相關危險因素、發病到入院時間(onset to door time, ODT)、入院到CT檢查時間(door to imaging time, DIT)、入院到溶栓治療時間(door to needle time,DNT)、發病到溶栓治療時間(onset to needle time, ONT)、靜脈溶栓率和治療結局的差異。結果 共納入急性缺血性腦卒中患者137例,其中,常規組65例,急診與病房聯動組72例。在診療時效性上,急診與病房聯動組與常規組相比,DIT、DNT、ONT時間明顯縮短(P<0.05);在溶栓率和預后方面比較,常規組靜脈溶栓10例(15.4%),預后良好9例(13.8%);急診與病房聯動組72例,靜脈溶栓23例(31.9%),預后良好20例(27.8%),兩組相比,急診與病房聯動組靜脈溶栓率、預后良好率均高于常規組(P<0.05)。結論 通過優化診療流程可以縮短急性缺血性腦卒中患者的DIT、DNT、ONT時間,增高溶栓比率,改善患者的預后,提高醫療質量。
[關鍵詞] 優化診療流程;缺血性腦卒中;醫療質量;急診與病房聯動診療
[Abstract] Objective The treatment of acute ischemic stroke has strict time window limitation, and the curative effect is closely related to the time of starting thrombolytic therapy. The aim of this study was to optimize the diagnosis and treatment process, shorten the time of diagnosis and treatment, and observe the role of this program in the diagnosis and treatment of acute ischemic stroke. Methods Continuous collection of patients with acute ischemic stroke from March 2017 to May 2018. Patients between March and September 2017 were treated with routine treatment, Octeber 2017 to May 2018. The patients were treated with emergency and ward linkage diagnosis and treatment, comparing the general conditions of the two groups, risk factors related to stroke, onset to door time (ODT), and admission to CT time(door to imaging time, DIT), admission to thrombotherapy time(DNT), onset to needle time(ONT), intravenous thrombolysis rate and treatment outcome differences. Results A total of 137 patients with acute ischemic stroke were enrolled, including 65 in the conventional group and 72 in the emergency and ward linkage group. In the timeliness of diagnosis and treatment, the DIT, DNT and ONT time were significantly shorter in the emergency department and the ward linkage group than in the conventional group(P<0.05). In the conventional group, 10 cases(15.4%) were compared in the thrombolysis rate and prognosis. The prognosis was good in 9 cases(13.8%); 72 cases in emergency department and ward linkage group, 23 cases (31.9%) with intravenous thrombolysis, and 20 cases(27.8%)with good prognosis. Compared with the two groups, the emergency and ward linkage group was intravenously dissolved. The rate of thrombus and good prognosis were higher than the conventional group (P<0.05). Conclusion By optimizing the diagnosis and treatment process, the DIT, DNT and ONT time of patients with acute ischemic stroke can be shortened, the thrombolytic ratio can be increased, the prognosis of patients can be improved, and the quality of medical care can be improved.
[Key words] Optimized diagnosis and treatment procedures; Ischemic stroke; Medical quality; Emergency and ward linkage diagnosis and treatment
腦卒中是一種急性的腦血管疾病,包括缺血性腦卒中和出血性腦卒中,其中缺血性腦卒中在腦卒中的占比高達70%。缺血性腦卒中是由于各種原因所致部分腦組織血流量減少,最終導致相應區域腦組織損害,出現腦功能喪失的一組疾病。它是臨床中的常見病,具有發病率高、死亡率高、致殘率高的特點,在我們國家,腦卒中的發病率大約為236.2/10萬人,已成為我國首位死亡原因,也是造成我國減壽年數的首位病因。
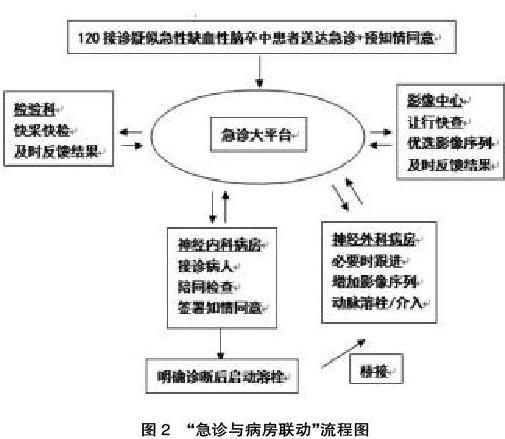
靜脈溶栓是急性缺血性腦卒中早期最有效的治療方法,可以快速恢復患者的腦血流灌注、挽救缺血半暗帶,有效減輕患者的神經功能缺損癥狀。但是受到治療時間窗的限制,急性缺血性腦卒中從發病到入院時間(關乎公眾健康教育、院前轉運等因素)相對不可控,那么在院內盡可能快而準確地評估病情并順利實施靜脈溶栓就成為急性缺血性腦卒中院內救治的最關鍵階段;腦卒中治療的時效性因此也就成為關乎提升腦卒中診療質量和改善患者預后的重中之重。急性缺血性腦卒中常規診療方案,各科室部門相對獨立、各司其職,診療流程相對耗時;“急診與病房的聯動”是在急診大平臺上,以患者為中心,通過120救護車、急診科、神經內科、神經外科、檢驗科、影像中心、急診藥房均高效聯動,優化診療流程實現縮短診治時間,改善急性缺血性腦卒中的診療質量。該研究以2017年3月—2018年5月收治的137例急性缺血性腦卒中患者為研究對象,驗證“急診與病房的聯動”方案是否可以縮短急性缺血性腦卒中治療的院內診治時間,是否可以改善醫療質量和改善預后。
1? 對象與方法
1.1? 研究對象
納入連續收集的2017年3月—2018年5月于包頭醫學院第一附屬醫院就診的急性缺血性腦卒中患者,其中,2017年3—9月間的患者進入常規組,2017年10月—2018年5月間的患者進入急診與病房聯動組。納入標準:①年齡≥40歲;②符合《中國急性缺血性腦卒中診治指南2014》[8]中急性缺血性腦卒中的診斷標準;③發病(出現腦卒中的癥狀)4.5 h內到達醫院;④適合靜脈溶栓的患者。排除標準:①發病時間無法確定的患者;②顱腦外傷、腫瘤和其他疾病引起的腦卒中患者。
1.2? 研究方法
記錄患者的一般情況,包括年齡、性別、既往病史及卒中相關危險因素(高血壓、糖尿病、房顫、冠心病、既往卒中史等);采集患者診療過程中在院內診療的時間節點及治療結局(治療后3個月隨訪改良Rankin量表(modified Rankin Scale,mRS)評分)等。
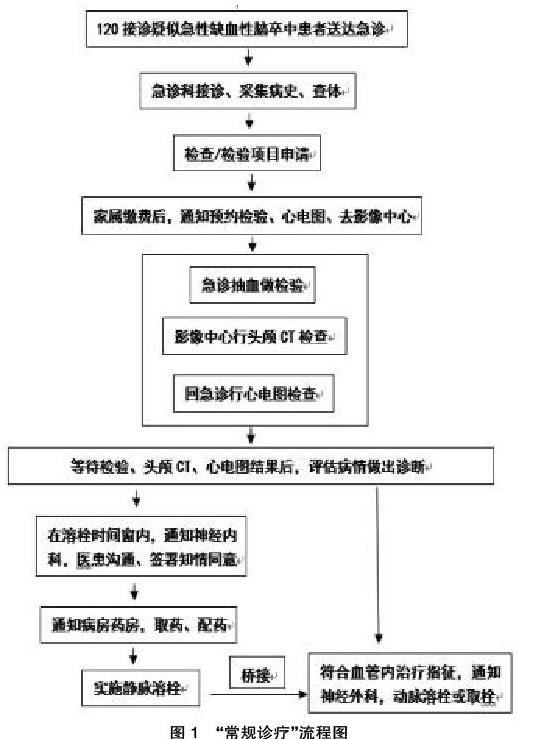
針對于區域腦卒中診療質量現狀,在《中國卒中中心建設指南》[9]建設標準的基礎上,結合醫院實際情況進一步優化腦卒中診療流程,于2017年3—9月間的患者采用常規診療方案(具體流程,見圖1),于2017年10月探索性啟動“急診與病房聯動”的醫院管理醫療質控措施(具體流程,見圖2)。時間節點追蹤主要包括發病到入院時間(ODT)、入院到CT檢查時間(DIT)、入院到溶栓治療時間(DNT)、發病到溶栓治療時間(ONT),并對患者的預后進行隨訪。
預后良好的判斷標準:治療后3個月隨訪患者的mRS評分,以mRS評分≤2分定義為預后良好。
1.3? 統計方法
應用SPSS 19.0統計學軟件分析數據,正態分布的計量資料以(x±s)表示,采用單因素方差分析;計數資料以率或構成比表示,組間比較采用χ2檢驗;P<0.05為差異有統計學意義。
2? 結果
2.1? 一般情況
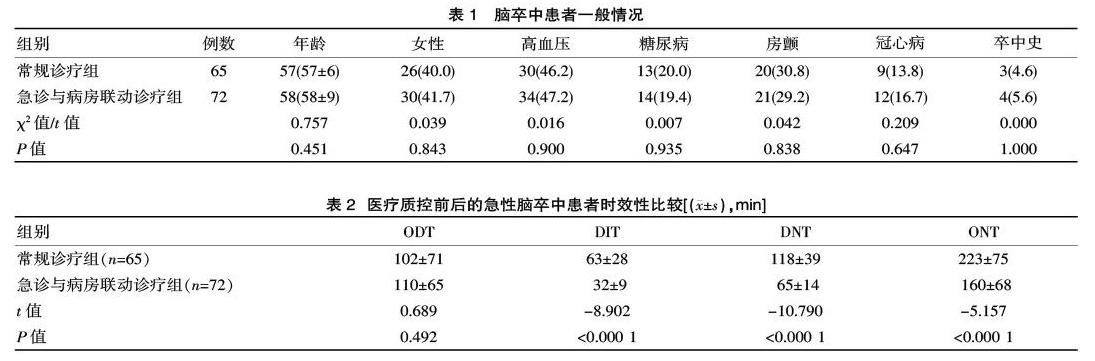
共納入急性缺血性腦卒中患者137例,2017年10月開始啟動“急診與病房聯動”的腦卒中醫療質控措施,2017年3—9月的65例患者是常規診療組,其中男39例,女26例,年齡為40~65歲,平均(57±6)歲;2017年10月—2018年5月的72例患者是急診與病房聯動診療組,其中男42例,女30例,年齡為41~69歲,平均(58±9)歲,兩組患者的年齡和性別差異無統計學意義(P>0.05)。常規組和急診與病房聯動組在卒中相關危險因素方面,既往糖尿病、高血壓病、房顫、冠心病、卒中史,兩組間比例的差異無統計學意義(P>0.05)。
2.2? 時間節點追蹤
該研究中,時間節點追蹤記錄,急診與病房聯動組同常規組相比,DIT、DNT、ONT時間明顯縮短,兩組差異有統計學意義(P<0.05);ODT時間未縮短,兩組間的差異無統計學意義(P>0.05)。
2.3? 預后結果
該研究中,按照診療過程記錄了患者是否予以實施靜脈溶栓,以及治療后3個月隨訪患者的mRS評分,判定預后情況。137例患者中共有33例實施了靜脈溶栓治療,3個月隨訪為預后良好的患者29例。在常規組,實施靜脈溶栓10例(15.4%),預后良好9例(13.8%);急診與病房聯動組,實施靜脈溶栓23例(31.9%),預后良好20例(27.8%)。急診與病房聯動組在靜脈溶栓的診療比例、預后良好占比均優于常規組,差異有統計學意義(P<0.05)。
該研究中,啟動“急診與病房聯動”醫療質量控制后,針對于急性缺血性腦卒中患者在發病4.5 h內實施靜脈溶栓的比例更高。在常規組中,腦卒中發病時間窗內溶栓患者占比為15.4%;這與我們國家十一五期間國家卒中登記的平均數據基本一致,也有研究表明,在我國急性缺血性腦卒中的治療中,與國外發達國家相比,靜脈溶栓的比例明顯偏低。該研究提示,在“優化診療流程”的醫院管理質控下,腦卒中患者的接受靜脈溶栓診療患者明顯提高,靜脈溶栓比例達31.9%;但是研究結果與國外卒中項目溶栓率達71.6%的數據還是有不小的距離,這也正是需要在腦卒中的管理上通過不斷優化流程、加強質控所努力的目標。另外,關于預后,該研究中常規組的預后良好率為13.8%,急診與病房聯動組的預后良好率為27.8%,靜脈溶栓比例更高的急診與病房聯動組預后良好率優于常規組,這與國內其他研究的結論基本一致,經過靜脈溶栓治療的腦卒中患者是會明顯獲益的,預后更好。
我們知道,延誤靜脈溶栓的因素包括兩類:一類是院外因素,另一類是院內因素。該研究結果顯示,ODT時間未縮短,兩組間的差異無統計學意義。ODT是發病到入院時間,這一時間的長短與否是和發生院外延遲影響溶栓治療的院外因素密切相關,因此,在院內的質量控制環節實施流程優化并不能引起ODT時間的縮短。該研究中,通過采取急診與病房聯動的醫院管理方案,明顯縮短了DIT、DNT、ONT時間。急性缺血性腦卒中患者的診療時效性,主要與影像檢查是否及時、快速評估病情后實施靜脈溶栓用藥是否及時等診療節點有關,DIT、DNT、ONT時間很好地起到了評價腦卒中靜脈溶栓院內延誤與否的作用。國際上有些研究嘗試通過各種醫院管理的質控方案來提高急性缺血性腦卒中的溶栓率和縮短DNT時間;并且隨著腦卒中診療技術的進步,在靜脈溶栓的基礎上,動脈溶栓、血管內介入等技術使用的也越來越多,也使得更多的患者獲益。有研究數據顯示,我國從獲得影像學檢查結果至開始使用溶栓藥的平均時間為85 min,這也是我國當前腦卒中診療時效性較歐美其他國家顯著延長的主要原因[17]。該研究中通過優化診療流程縮短了DIT、DNT、ONT時間,也證實了急診與病房聯動的醫院質量管理方案在急性缺血性腦卒中質控管理中的有效性。
綜上所述,通過優化診療流程,采用急診與病房聯動的措施,可以提高靜脈溶栓比率、縮短診治時間、改善患者的預后,從而提升急性缺血性腦卒中的醫療質量。
[參考文獻]
[1]? 王隴德,毛群安,張宗久.中國腦卒中防治報告(2018)[M].北京:人民衛生出版社,2018.
[2]? Xu G,Ma M,Liu X,Hankey GJ.Is there a stroke belt in China and why Stroke,2013(44):1775-83.
[3]? Zhou M,Wang H,Zhu J,et al.Cause-specific mortality for 240 causes in China during 1990-2013: a systematic subnational analysis for the Global Burden of Disease Study 2013[J].Lancet, 2016(387):251-72.
[4]? Devos D,Sevin M,De GS,et al.Management of ischemic stroke in the hyperacute phase[J].Panminerva Medica,2013,55(1):59-78.
[5]? Sillanpaa N,Saarinen JT,Rusanen H,et al.The clot burden score, the Boston Acute Stroke Imaging Scale, the cerebral blood volume ASPECTS, and two novel imaging parameters in the prediction of clinical outcome of ischemic stroke patients receiving intravenous thrombolytic therapy[J].Neuroradiology,2012,54(7): 663-672.
[6]? 徐安定,丁燕,李牧.中國缺血性卒中早期靜脈溶栓的現狀、阻礙因素及改進策略[J].中國卒中雜志,2014,9(6):522-528.
[7]? Fonarow GC,Zhao X,Smith EE,et al.Door-to-Needle Times for Tissue Plasminogen Activator Administration and Clinical Outcomes in Acute Ischemic Stroke Before and After a Quality Improvement Initiative[J].Jama,2014,311(16):1632-1640.
[8]? 中華醫學會神經病學分會,中華醫學會神經病學分會腦血管病學組.中國急性缺血性腦卒中診治指南2014[J].中華神經科雜志,2015,48(4):246-257.
[9]? 國家衛生和計劃生育委員會神經內科醫療質量控制中心.中國卒中中心建設指南[J].中國卒中雜志,2015,10(6):499-507.
[10]? Wang Y,Liao X,Zhao X,et al.Using recombinant tissue plasminogen activator to treat acute ischemic stroke in China:analysis of the results from the Chinese National Stroke Registry(CNSR) [J].Stroke,2011,42(6):1658-1664.
[11]? Fonarow GC,Reeves MJ,Smith EE,et al.Characteristics, performance measures, and in-hospital outcomes of the first one million stroke and transient ischemic attack admissions in get with the guidelines-stroke[J].Circ Cardiovasc Qual Outcomes,2010,3(3):291-302.
[12]? Gisele Sampaio Silva,Lee H,Schwamm.Review of Stroke Center Effectiveness and Other Get with the Guidelines Data[J].Cardiovascular Disease and Stroke,27 July,2013:373.
[13]? Christine Lu-Emerson, David Likosky, Alpesh Amin, David Tirschwell, MScManagement of ischemic stroke: Part 2. The inpatient stay[J].J. Hosp. Med,2010,5(2):88-93.
[14]? Rostanski SK,Stillman JI,Schaff LR,et al. E-Mail Is an Effective Tool for Rapid Feedback in Acute Stroke[J].Neurohospitalist,2017,7(4):159-163.
[15]? Meretoja A,Strbian D,Mustanoja S,et al.Reducing in-hospital delay to 20 minutes instroke thrombolysis[J].Neurology,2012,79(4):306-313.
[16]? 張美霞,陳智才,張睿婷,等.院前預通知流程改善急性缺血性卒中患者血管內治療的預后[J].中國卒中雜志,2018, 13(2):114-121.
[17]? Song D,Tanaka E,Lee K,et al.Factorsassociated with early hospital arrival in patientswith acute ischemic stroke[J].J Stroke, 2015,17(2):159-167.
(收稿日期:2019-01-25)
