De Winter syndrome and ST-segment elevation myocardial infarction can evolve into one another:Report of two cases
2019-04-18 07:23:18YangYiLinYuDanWenGuoLinWuXiangDongXu
World Journal of Clinical Cases 2019年20期
Yang-Yi Lin,Yu-Dan Wen,Guo-Lin Wu,Xiang-Dong Xu
Yang-Yi Lin,Guo-Lin Wu,Xiang-Dong Xu,Department of Cardiology,Jiading District Central Hospital Affiliated Shanghai University of Medical and Health Sciences,Shanghai 201800,China
Yu-Dan Wen,Department of Electrocardiology,the Third Affiliated Hospital of Wenzhou Medical University,Wenzhou 325200,Zhejiang Province,China
Abstract
Key words:De Winter syndrome;ST-segment upsloping depression;Dynamic;Case report
INTRODUCTION
The de Winter electrocardiography(ECG)pattern is a sign that implies proximal left anterior descending coronary artery occlusion in patients with chest pain.The previous view was that the de Winter ECG pattern is static.We show that de Winter and ST-segment elevation myocardial infarction can evolve into one another.
CASE PRESENTATION
Chief complaints
Case 1:A 65-year-old man presented with sudden chest pain at rest associated with diaphoresis.He had no complaint of abdominal pain,bloody stools,or weight loss.
Case 2:A 50-year-old man presented with sudden-onset,severe,substernal crushing chest pain radiating to the left shoulder and back,accompanied by diaphoresis.He had no complaint of bloody stools,cough,or hemoptysis.
History of present illness
Case 1:The patient’s symptoms started 55 min ago and did not alleviate throughout the course of the disease.
Case 2:The patient’s symptoms started 1 h ago,when he was referred to our Emergency Department,and alleviated,but chest pain recurred after 81 min.
History of past illness
Case 1:He has a history of hypertension for 26 years and diabetes for 12 years.
Case 2:He has a history of hyperlipidemia for 4 years.
Physical examination
Case 1:The patient’s temperature was 36.7 °C,heart rate was 80 bpm,respiratory rate was 14 breaths per minute,blood pressure was 111/75 mmHg,and the oxygen saturation was 98% while the patient was breathing ambient air.The S1 and S2 were normal and there was no evidence of a heart murmur on cardiac examination.
Case 2:The patient’s temperature was 37.4 °C,heart rate was 96 bpm,respiratory rate was 20 breaths per minute,blood pressure was 103/85 mmHg,and oxygen saturation was 98% on ambient air.The S1 and S2 heart sounds were normal and there was no murmur on cardiac auscultation.
Laboratory examinations
Case 1:His troponin T level was 0.049 ng/mL(normal value:0.010-0.023),myoglobin level was 45 μg/L(normal value:20-80),pro-BNP was 94 μg/L(normal value:< 300),CK-MB was 3.4ng/L(normal value:0- 7.2),and D-dimer was 338 μg/L(normal value:< 500).
Case 2:His troponin I level was 20.93 ng/mL(normal value:0.000-0.080),myoglobin level was 5520.2 ng/mL(normal value:0-154.9),BNP was 75.5 pg/mL(normal value:< 100),CK-MB was 146.7 ng/mL(normal value:0-7.2),D-dimer was 5.14 μg/mL(normal value:0.00-0.55).
Imaging examinations
Case 1:The first ECG(Figure 1A),performed immediately in the emergency department,showed only T-wave inversion in the III and aVF leads.Another ECG(Figure 1B)was performed at the 100thminute,showing upsloping ST segments depressed by > 0.1 mV in the V1-V6 leads,with tall and symmetrical T waves in the precordial leads;the J point was raised by 0.1 mV in the aVR lead,and there was a loss of precordial R-wave progression.A third ECG,performed at hospital arrival(Figure 1C),showed ST segment elevation by 0.2 mV in the I and aVL leads.The emergency coronary angiography revealed multi-vessel disease and complete proximal left anterior descending coronary(LAD)occlusion(Figure 2).The postprocedural ECG is shown in Figure 1D.
Case 2:The first ECG showed ST-segment elevation(0.1-1.7 mV)in I,aVL,and precordial leads(Figure 3A).The second ECG showed that the ST-segments had significantly fallen back(Figure 3B).The patient experienced chest pain recurrence after 81 min,and ECG showed a typical de Winter pattern(Figure 3C).The preemergency coronary angiography ECG is shown in Figure 3D.Coronary angiography revealed 99% stenosis of the middle LAD(Figure 4).
FINAL DIAGNOSIS
Case 1
According to the symptoms and the electrocardiograms and coronary angiograms,this patient was diagnosed with de Winter syndrome at first,which then evolved to ST-segment elevation myocardial infarction(STEMI).
Case 2
According to the symptoms and the electrocardiograms and coronary angiograms,this patient was diagnosed with STEMI at first,which then evolved to de Winter syndrome.
TREATMENT
Case 1
The patient underwent percutaneous coronary intervention in the LAD using a 3.0 mm × 38 mm stent.
Case 2
The lesion was treated with a drug-eluting stent(3.5 mm × 18 mm).
OUTCOME AND FOLLOW-UP
Case 1
No complications occurred in hospital,and the patient was discharged free of chest pain 5 d later.During outpatient follow-up,he had no characteristic clinical symptoms.No evidence of myocardial ischemia was noted in the routine examinations.
Case 2
No complications developed during hospitalization,and the patient was discharged on the ninth day of hospitalization.During outpatient follow-up,he had no characteristic clinical symptoms.No evidence of myocardial ischemia was noticed in the routine examinations.

Figure 1 Electrocardiography examinations(Case 1).
DISCUSSION
The de Winter ECG pattern(ST-segment upsloping depression and tall,positive symmetrical T waves;ST-elevation(1-2 mm)in lead aVR;a loss of precordial R-wave progression;and QRS complexes not widened or slightly widened)was first described by de Winter in 2008[1].The key diagnostic features of the de Winter ECG pattern include the follow two points:(A)ST-segment upsloping depression > 1 mm with tall and positive symmetrical T waves in the precordial leads;and(B)STsegment elevation in the aVR lead[2-4].The previous view of this ECG pattern was that it is static and indicates complete proximal LAD occlusion[1,4].However,our two cases demonstrate that the ECG pattern of de Winter syndrome and STEMI can evolve into one another.The first patient evolved from de Winter syndrome to STEMI after 72 min,and coronary angiography revealed complete proximal LAD occlusion.The second patient transformed from STEMI to de Winter syndrome after 2 h,and a 99%middle LAD stenosis was confirmed by coronary angiography.Goebelet al[5]reported a case of de Winter pattern progressing to STEMI within several hours and Lamet al[6]described a patient who spontaneously transformed from STEMI to de Winter pattern before emergency angiography and reperfusion therapy,which are similar to our present cases.Therefore,we believe that the de Winter ECG pattern reflects a coronary thrombus in formation which,however,has not completely occluded the coronary arteries.The ECG pattern of STEMI changes to the de Winter syndrome owing to autolysis of the intracoronary thrombus.Therefore,we believe the de Winter ECG pattern is transient,and either progresses to STEMI when the thrombus continues to form and completely occludes the coronary arteries,or the thrombus autolyzes and the ECG tends to become normal.Zhaoet al[7]also showed spontaneous recanalization of the thrombus in a patient with de Winter syndrome.Picaet al[8]reported a case of acute stent thrombosis with de Winter ECG pattern,after thrombectomy and ballooning,the de Winter ECG pattern with typical ECG evolution as STEMI.What’s more,our second patient showed an elevated D-dimer value of 5.14 ug/mL,which reflected autolysis of the intracoronary thrombus.In essence,deWinter syndrome may be a thrombotic disease.The two patients with de Winter syndrome reported by Raoet al[9]and Pranataet al[10],who were treated successfully with thrombolytic therapy,support this opinion.
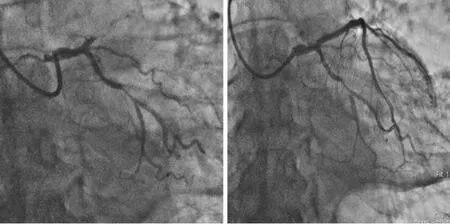
Figure 2 Coronary angiogram showing complete occlusion of the proximal left anterior descending coronary and a 90% stenosis of the middle of the left circumflex arteries(left)and that after drug-eluting stent placement(right).
CONCLUSION
The de Winter ECG pattern is transient and dynamic,and it reflects proximal or mid-LAD subtotal occlusion rather than total occlusion.Physicians and others who attend patients with chest pain should be able to early recognize this STEMI-equivalent ECG pattern and need to perform urgent angiography and reperfusion therapy to improve the clinical outcomes of these patients.
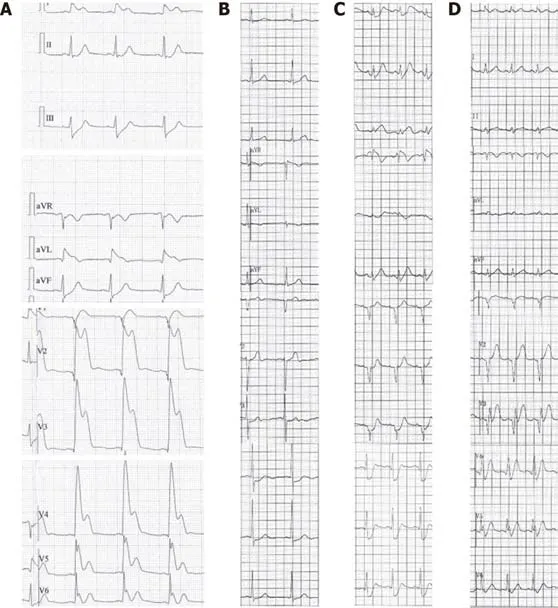
Figure 3 Electrocardiography examinations(Case 2).

Figure 4 Coronary angiogram showing a 99% stenosis of the middle left anterior descending artery(left)and that after drug-eluting stent placement(right).
 World Journal of Clinical Cases2019年20期
World Journal of Clinical Cases2019年20期
- World Journal of Clinical Cases的其它文章
- Rh-incompatible hemolytic disease of the newborn in Hefei
- Ureteral Ewing’s sarcoma in an elderly woman:A case report
- Anaplastic lymphoma kinase-negative anaplastic large cell lymphoma masquerading as Behcet's disease:A case report and review of literature
- Synchronous quadruple primary malignancies of the cervix,endometrium,ovary,and stomach in a single patient:A case report and review of literature
- Sister Mary Joseph’s nodule in endometrial carcinoma:A case report
- Alternative technique to save ischemic bowel segment in management of neonatal short bowel syndrome:A case report