Synchronous quadruple primary malignancies of the cervix,endometrium,ovary,and stomach in a single patient:A case report and review of literature
2019-04-18 07:23:22DanDanWangQingYang
World Journal of Clinical Cases 2019年20期
Dan-Dan Wang,Qing Yang
Dan-Dan Wang,Qing Yang,Department of Obstetrics and Gynecology,Shengjing Hospital of China Medical University,Shenyang 110004,Liaoning Province,China
Abstract
Key words:Quadruple primary malignancy;Synchronous;Surgery;Case report
INTRODUCTION
Multiple primary malignancy(MPM)is defined as two or more malignant tumors with distinct histology occurring at different locations.Depending on the time of diagnosis at each primary site,MPMs can be classified as either synchronous or metachronous[1,2].In the literature,the prevalence of MPM is estimated to be in the range of 2%-17%[2].It is rare,and most cases involve two sites.The occurrence of three or more primary tumors in a single patient has rarely been described.Herein we report an exceptional case of a 56-year-old woman who was successfully treated for endocervical adenocarcinoma,endometrial endometrioid adenocarcinoma,endometrioid ovarian carcinoma,and gastric adenocarcinoma via surgery at the Shengjing Hospital of China Medical University,in conjunction with a brief review of related literature.
CASE PRESENTATION
Chief complaints
A 56-year-old postmenopausal woman who was 160 cm in height and weighed 67.1 kg(body mass index 26.2)came to our institute with a 1-mo history of vaginal bleeding with no associated abdominal pain.
Medical history
The patient has been treated for diabetes mellitus for the past 8 years.She had no history of hypertension and reported did not use tobacco or alcohol.She had no history of exposure to oral estrogen,and her family history was unremarkable.
Physical examination upon admission
Gynecologic examination revealed an enlarged smooth-faced cervix and decreased mobility of the uterus,but no gross lesion.
Laboratory examinations
Serum carbohydrate antigen(CA)-199 was 85 U/mL(normal range 0-35 U/mL),and carcinoembryonic antigen(CEA),CA-125,and CA-724 were normal.Human papillomavirus(HPV)DNA testing was negative.
Biopsy and imaging examinations
Biopsy of fractional curettage resulted in the diagnosis of endocervical poorly differentiated adenocarcinoma,and endometrial endometrioid adenocarcinoma,in conjunction with atypical hyperplasia.Pelvic magnetic resonance imaging(MRI)depicted a solid mass of 4.3 cm × 3.3 cm located in the cervical canal of the uterus that was indistinct from the anterior rectum wall,thickened and distorted endometrium and small cystic lesions of bilateral adnexa(left 1.6 cm × 0.8 cm,right 1.8 cm × 1.2 cm)(Figure 1A).Contrast computed tomography(CT)scanning depicted thickening of the wall of the greater curvature of the stomach with enlarged perigastric lymph nodes,and suspected malignancy(Figure 1B).Whole-body positron emission topography(PET)/CT with 18-fluorodeoxy-glucose(FDG)scanning revealed abnormal FDGuptake in the cervix,uterine cavity,right adnexa,and stomach(Figure 1C).Further esophagogastroduodenoscopy examination revealed multiple ulcerative lesions in the gastric angle and antrum.Biopsy results revealed gastric intraepithelial neoplasia with focal intramucosal cancerization.
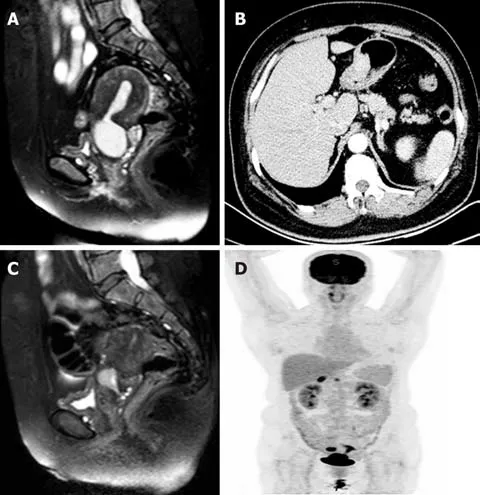
Figure 1 lmaging findings of the patient.
FINAL DIAGNOSIS
The patient was diagnosed with MPMs including endocervical adenocarcinoma,endometrial endometrioid adenocarcinoma,gastric carcinoma and suspected ovarian carcinoma.
TREATMENT
Neoadjuvant chemotherapy was administered first,aimed at reducing the tumor load.After two courses of taxol(175 mg/m2)/oxaliplatin(130 mg/m2)chemotherapy,MRI was performed again and depicted a significantly decrescent cervical solid mass of approximately 1.7 cm × 2.2 cm(Figure 1D).After comprehensive multidisciplinary consultation and informing the patient of the challenges and uncertainties involved,a combined surgery was planned.For genital tract carcinoma transabdominal radical hysterectomy and bilateral oophorosalpingectomy were performed with pelvic and para-aortic lymph node dissection.For the gastric lesion radical distal gastrectomy,gastrojejunostomy and omentectomy were performed with perigastric lymph node dissection.During the exploratory laparotomy a solid mass was observed on the anterior wall of the rectus approximately 3 cm above the rectouterus reflexes peritoneum which was considered to be a metastasis of endocervical cancer.Partial rectectomy was synchronously performed.The entire operation lasted 8 h.There were no major complications during the operation.
Pathological findings
Histopathological examination of the surgical specimens with immunohistochemistry confirmed the diagnosis of MPMs,with observations including:(1)Poorly differentiated endocervical adenocarcinoma admixed with partial neuroendocrine changes,deep stromal invasion and rectal involvement,Ki67 and MOC-31 positively,partial positively for cytokeratin(CK),CK8/18,thyroid transcription factor-1and synaptophysin and negatively for vimentin,CEA,CD56,P63,P40,and chromogranin(Figure 2A,B and C);(2)Diffuse endometrial atypical hyperplasia combined with localized highly differentiated endometrioid adenocarcinoma without myometrialinvasion,and tumor cells positive for estrogen receptor(ER)and progesterone receptor(PR)(Figure 2D and E);(3)Localized right ovarian endometrioid adenocarcinoma,and tumor cells positive for ER,PR,and CK7 but negative for CK20(Figure 2F);and(4)Moderately to highly differentiated gastric adenocarcinoma with deep muscular infiltration and perigastric lymph node metastasis,tumor cells positive for human epidermal growth factor receptor 2(Figure 2G,H and I).
OUTCOME AND FOLLOW-UP
The patient recovered smoothly but deep vein thrombosis(DVT)of the left lower leg was detected 15 d after surgery.For personal reason the patient declined thrombolytic therapy in our hospital and requested a referral to a local center.During the follow-up period she was cured of the DVT by approximately 2 mo after surgery at that local center.The patient declined subsequent adjuvant radio-chemotherapy and was lost to follow-up 1 year after surgery.Despite the potential informative value that it may have had,the expression of the genetic panel in this patient lacks of mean(data not displayed).
DISCUSSION
The most widely accepted criteria for the diagnosis of MPMs was proposed by Warren and Gates[1],and it requires that(1)each tumor is malignant;(2)each tumor has its own pathological features;(3)tumors occur in different parts of the organs,and are not continuous with each other;and(4)each tumor has its own metastatic pathway and the diagnosis of metastatic or recurrent tumors can be excluded.MPMs are known to be more commonly encountered in the gynecologic and gastrointestinal tracts most likely because they are derived from the same embryonic layer or tissue and in the case of gynecologic malignancies,responsive to the same hormones[3].
Notably there was some debate about the pathological diagnosis of primary ovarian cancer in the present case.Tumor cell morphology and immunohistochemistry markers suggested that the type of cancer in the right ovary was endometrioid adenocarcinoma which could easily have been mistaken for an endometrial cancer metastasis.Pathology results indicated that it was a focal highly differentiated endometrioid adenocarcinoma without myometrial or lympho-vascular space invasion,as well as a unilateral localized ovarian endometrioid cancer.Synchronous endometrial and ovarian cancer(SEOC)has been a matter of dispute in the past,because of the difficulties in differential diagnosis between two independent primary tumors and metastasis from one site to the other in this context,especially when the histologic types are concordant.Traditionally,the Ulbright and Roth criteria[4]followed by the Scully criteria[5]have been utilized to distinguish SEOC from metastatic endometrial or ovarian cancer.In endometrial tumors the criteria include the size of the tumor and depth of invasion,direct extension to the adnexa,lympho vascular space invasion,the presence of atypical hyperplasia in the surrounding endometrium,and grading.In ovarian tumors the criteria include the the presence of endometriosis,size and laterality of the tumor,surface implants,hilar location,lympho vascular space invasion,and multinodularity.SEOC is ordinarily more likely to be stage I disease with endometrioid histology[6,7].In the present case we ultimately considered both to be primary carcinomas in the uterus corpus and ovary.
Factors contributing the increasing frequency of MPM diagnoses include improved living standards,advances in diagnostic testing modalities,the development of more sophisticated treatments,and improved cancer screening and surveillance procedures[2,8].Metachronous MPMs are more common than synchronous malignancies with a ratio 2.7:1[3,9].Most cases of MPMs involve two primary neoplasm,whereas triple,and quadruple primary neoplasms are exceedingly rare.The incidence of quadruple cancers has been reported to be less than 0.1%[10].During the generation of this current report a PubMed-indexed English literature search yielded 9 reported cases of quadruple synchronous neoplasms[3,11-18](Table 1).To our knowledge,to date the combination of triple synchronous neoplasms of the female genital system(cervix,endometrium,and ovary)in conjunction with one primary digestive tract cancer has never been reported.
Although the underlying mechanisms responsible for the development of MPM are yet to be fully elucidated,frequently implicated factors can been collated into three broadly defined categories[2].First,host factors include genetic susceptibility,immune status,hormonal usage and a history of chemo -and/or radiotherapy for the treatment of cancer.For example,Lynch syndrome patients are susceptible to colorectal cancers,endometrial cancers,and other malignancies[19].Hereditary breast and ovarian cancer syndrome is a highly-penetrant,autosomal-dominant breast and ovarian cancer predisposition caused by germline mutations in theBRCA1andBRCA2genes[20].Long-term non-resistant estrogen exposure is a major risk factor for endometrial cancer[21].As well as congenital genetic mutations,somatically acquired genetic abnormalities such as punctiform mutations,loss of heterozygosity and microsatellite instability can also contribute to carcinogenesis[2].Hájkováet al[7]conducted comprehensive molecular analysis in 22 SEOC patients and reported that clonal origin was confirmed in all of them by way of at least one shared mutation in PTEN,AKT1,PIK3CA,KRAS,TP53,or ARID1A.Microsatellite instability phenotypes were detected in 5/22(22.7%)SEOC of the patients.Secondly,lifestyle factors include such things as alcohol,and tobacco usage.A third is exposure to infectious environmental influences and occupational hazards.Helicobacter pylori and Epstein-Barr virus infection as well as behavioral factors such as alcohol consumption,and cigarette smoking are reportedly associated with a higher risk of developing gastric cancer[18].HPV is an obligate component of most cervical cancers.In a multicenter epidemiological study,high-risk HPV DNA was detected in 94% of adenocarcinomas in situ,85% of adenosquamous carcinomas,and 76% of adenocarcinomas[22].The present patient had no family history of colon,gastric,breast or gynecological cancer,and no history of non-resistant estrogen usage,no alcohol consumption,or cigarette smoking.Genetic sequencing was performed but results lack of mean.It is unlikely that patients with synchronous primary cancers have hereditary cancer syndromes.Though a history of diabetes mellitus and being overweight may be relevant in the development of MPMs in the present patient,an unidentified mutation or other factors may exist.
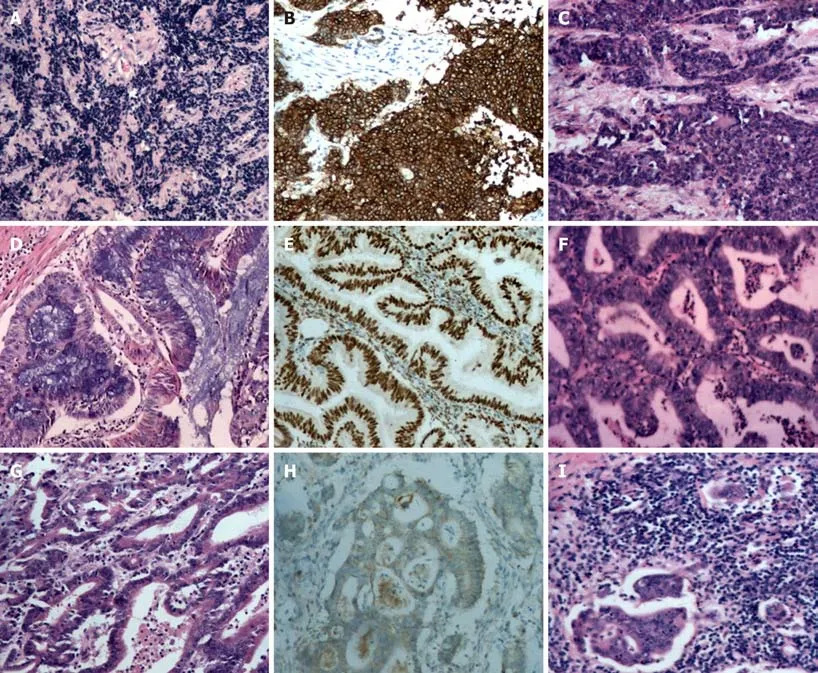
Figure 2 Histopathological and immunohistochemical staining findings.
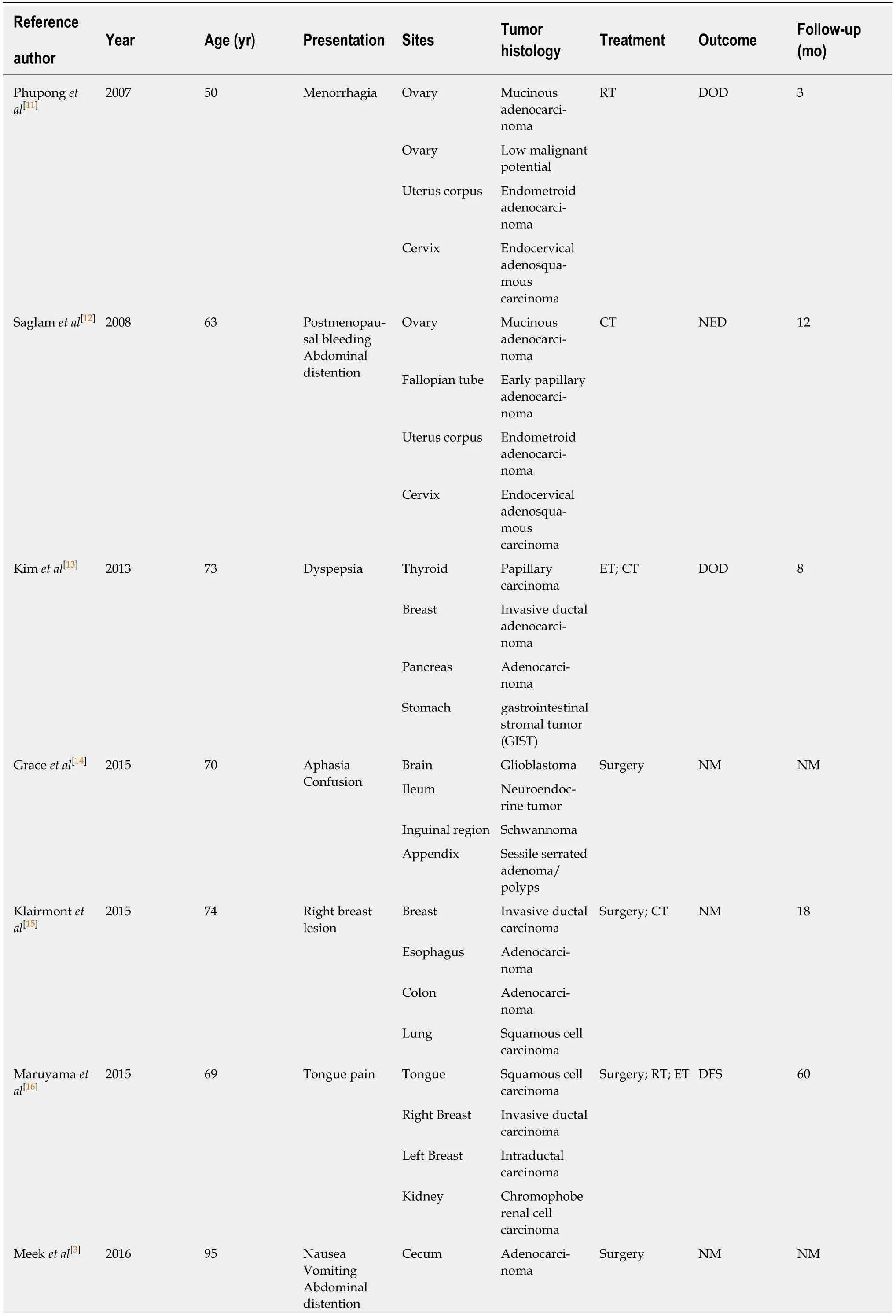
Table 1 Summary of all existing cases of quadruple synchronous primary malignancies in the English literature(n = 9)
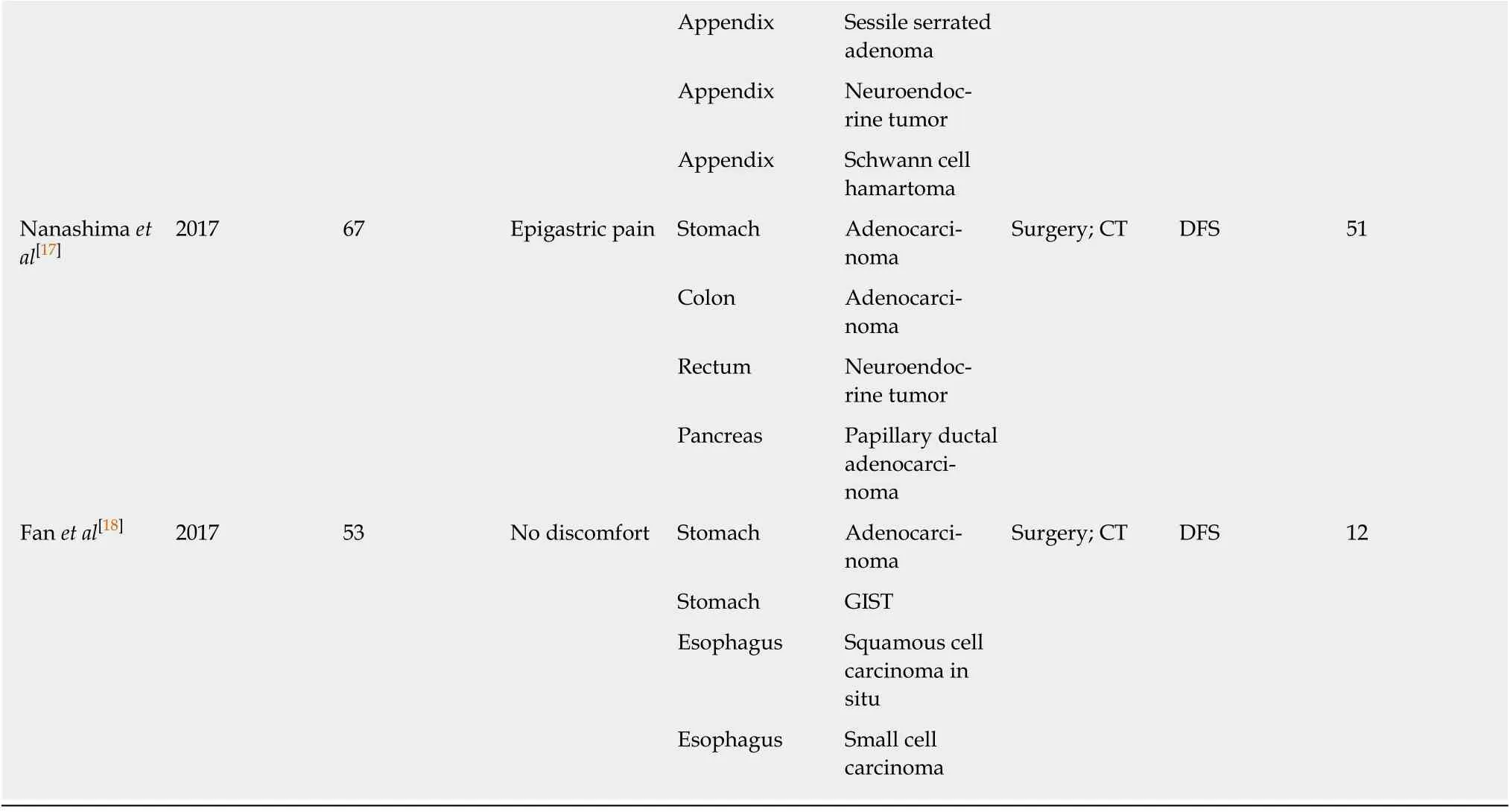
ET:Endocrinotherapy;CT:Chemotherapy;RT:Radiotherapy;DOD:Died of disease;NED:No evidence of disease;NM:Not mentioned;DFS:Disease free.
Currently,several types of examinations can help to prevent overlooking synchronous MPMs,including contrast CT,MRI,and PET/CT,as well as various endoscopic examinations.In one retrospective study it was reported that PET/CT had higher sensitivity with regard to the detection of synchronous cancers in patients with head and neck squamous cell carcinoma than conventional work-up with CT,barium swallow esophagram and panendoscopy(88.2%vs52.9%)[23];however,PET/CT is an expensive examination and sometimes identifies false-positive lesions.Rapid development of endoscopic techniques is facilitating enhanced-visualization of lesion morphology and more accurate localization,particularly in the context of the diagnosis of cavitary organ lesions[24,25].
Currently there are no definitive guidelines for the management of MPMs involving separate organ.Synchronous MPMs should be discussed by a multidisciplinary team,and a treatment consensus is best devised via input from surgeons,oncologists,radiation oncologists,radiologists,pathologists,and the patient.In general,surgical interventions should initially aim to exclude the presence of metastatic disease.The present patient underwent combined radical resection of all tumors,which entailed a long operation under general anesthesia.Unfortunately she also suffered from postoperative DVT,which might could have been fatal[26].In such cases,a balance must be met between providing effective treatment while preserving quality of life,and minimizing the morbidity of what is often a highly complex,protracted,and potentially toxic treatment course.
CONCLUSION
Synchronous primary quadruple malignancy is an extremely rare event.In this report,the clinical and pathologic details of the case of a 56-year-old female patient with synchronous with four synchronous primary tumors including poorly-differentiated endocervical adenocarcinoma,highly-differentiated endometrial endometrioid adenocarcinoma,endometrioid ovarian carcinoma,and moderately to highly differentiated gastric adenocarcinoma are presented for the first time.The etiology and mechanisms of MPM remain controversial,and further research is needed to explain these simultaneous cancers.
 World Journal of Clinical Cases2019年20期
World Journal of Clinical Cases2019年20期
- World Journal of Clinical Cases的其它文章
- Rh-incompatible hemolytic disease of the newborn in Hefei
- Ureteral Ewing’s sarcoma in an elderly woman:A case report
- Anaplastic lymphoma kinase-negative anaplastic large cell lymphoma masquerading as Behcet's disease:A case report and review of literature
- Sister Mary Joseph’s nodule in endometrial carcinoma:A case report
- Alternative technique to save ischemic bowel segment in management of neonatal short bowel syndrome:A case report
- Ureter - an unusual site of breast cancer metastasis:A case report