Removal of refractory thrombus by 5F child catheter in patients with subacute myocardial infarction
2019-03-22 09:09:54LiSHENGJianQiangLIDangHuiSUNYongTaiGONGJingYiXUEYueLI
Journal of Geriatric Cardiology
2019年2期
Li SHENG, Jian-Qiang LI, Dang-Hui SUN, Yong-Tai GONG, Jing-Yi XUE, Yue LI
Department of Cardiology, the First Affiliated Hospital of Harbin Medical University, Harbin, China
Keywords: Percutaneous coronary intervention; Refractory thrombus; Subacute myocardial infarction;Thrombus aspiration
No-reflow phenomenon is common in patients with acute coronary syndrome (ACS) after percutaneous coronary intervention (PCI), and it is strongly associated with adverse clinical prognosis. Previous studies have shown that heavy thrombus burden could predict the development of no-reflow in PCI.[1,2]Manual and mechanical thrombus aspiration catheters are widely used; however, there is still residual refractory thrombus left after the routine use of thrombectomy, especially in patients with subacute myocardial infarction (SMI).[3–6]In our practice, child catheter aspiration has been used as a safe and effective approach to solve the residual thrombus in SMI patients. We described this technique in detail by a series of cases.
The child catheter aspiration was first performed in a SMI patient who failed in the use of Thrombuster II aspiration catheter for the removal of thrombus. A 48-year-old woman presented with recurrent chest pain for seven days.Electrocardiogram showed pathological Q waves in V1-5 leads. Cardiac Troponin I was elevated to a value of 1.124 ng/mL, CK-MB was back to normal already, and therefore a diagnosis of SMI was made. Angiography revealed a total occlusion at the proximal left anterior descending (LAD)with thrombus grade 5 and TIMI 0 flow (Figure 1A). A 6 Fr JL4.0 guiding catheter (Terumo, Tokyo, Japan) was advanced to the left coronary artery (LCA) ostium via right radial access. Runthrough NS guidewire (Terumo, Tokyo,Japan) was passed through the lesion. Angiography showed a refractory thrombus with TIMI 2 flow (Figure 1B). A Thrombuster II extraction catheter (Terumo, Tokyo, Japan)was attempted a few times (Figure 1C). However, there was still refractory thrombus with TIMI 2 flow (Figure 1D).Then a Heartrail II 5F child catheter (Terumo, Tokyo, Japan)was advanced into the proximal LAD for aspiration (Figure 1E). Angiography showed the TIMI 3 flow of LAD, a severe stenosis at the proximal LAD and no remained thrombus burden. A 3.5 mm × 24 mm Nano stent (Lepumedical,China) was implanted successfully (Figure 1F).
Under certain conditions, thrombus aspiration by the child catheter could be a reasonable option if both manual and mechanical thrombus aspiration devices fail. A 49-yearold man had typical angina during exercise for ten days which worsened for three days. Electrocardiogram indicated pathological Q waves and inverted T waves in II, III and aVF leads. Cardiac Troponin I was 4.971 ng/mL. The above data supported the diagnosis of SMI. Angiography revealed a total occlusion in the proximal part of right coronary artery (RCA) (Figure 2A), the collateral circulation from LCA,and non-significant lesions in left coronary system (Figure 2B). A 6 Fr Judkins Left 3.5 guiding catheter (Terumo, Tokyo, Japan) was advanced to the RCA ostium via right radial access. Runthrough NS guidewire (Terumo, Tokyo,Japan) was passed through the lesion. Angiography showed heavy thrombus burden with TIMI 0 flow (Figure 2C). A Thrombuster II aspiration catheter (Terumo, Tokyo, Japan)(Figure 2D) and an Angiojet mechanical aspiration catheter(Possis, Minneapolis, MN, USA) (Figure 2E) were attempted for thrombus aspiration. Unfortunately, there was still residual refractory thrombus with TIMI 0 flow (Figure 2F). Then a Heartrail II 5F child catheter (Terumo, Tokyo,Japan) was advanced into the mid part of RCA for aspiration (Figure 2G). The following angiography showed that the flow of RCA was TIMI 3, thrombus burden was lessened significantly, and there were severe stenoses at proximal and distal RCA (Figure 2H). We implanted Helios 3.0 mm × 38 mm (Kinhely Medical Co., China) and Firehawk 4.0 mm × 33 mm (MicroPort Medical Co., China) drugeluting stents. The final angiography showed that there was no thrombus burden with TIMI 3 flow and no residual stenosis (Figure 2I).
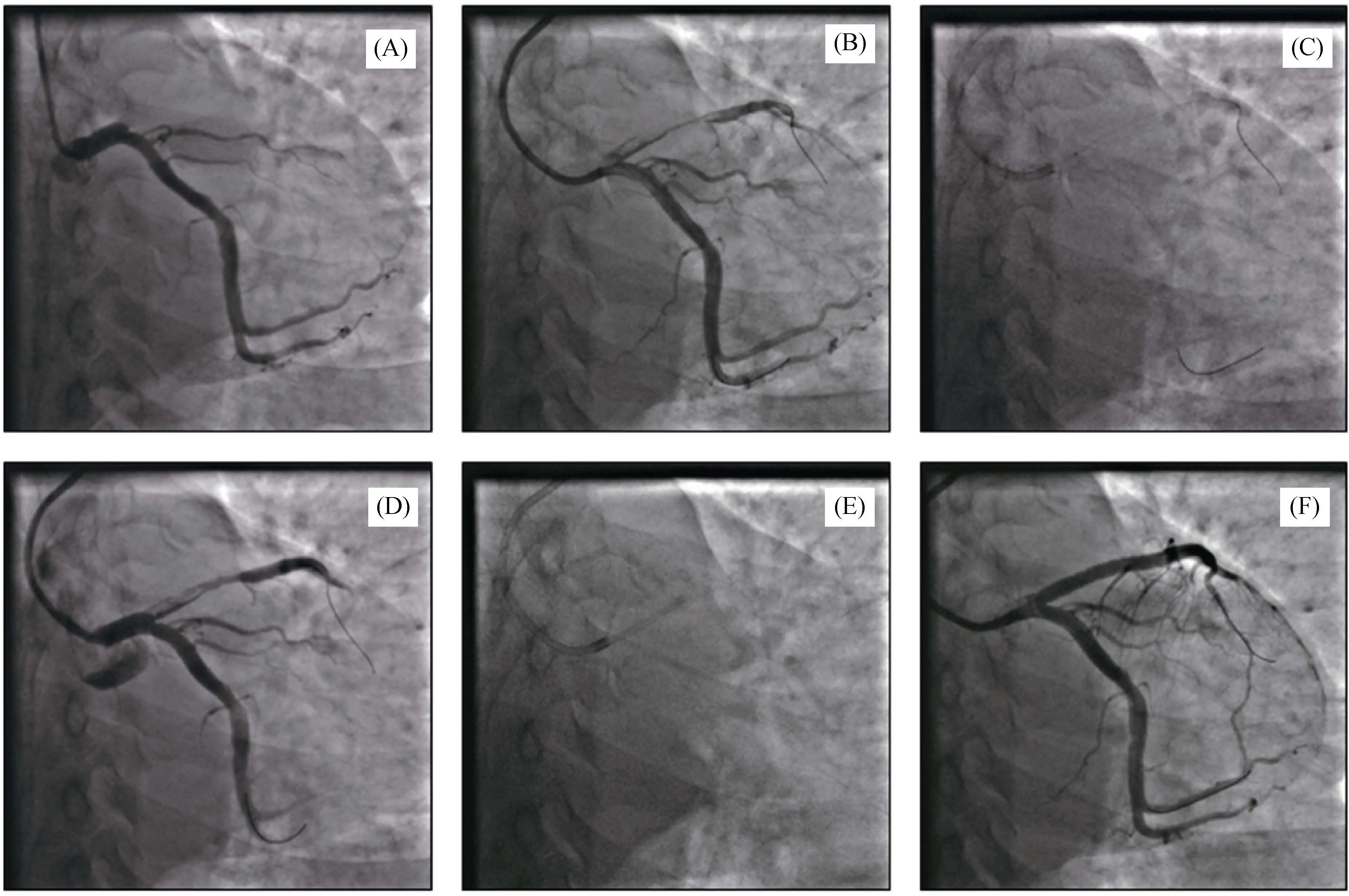
Figure 1. Application of the child catheter aspiration after the Thrombuster II aspiration catheter failure in a SMI patient. (A): A total occlusion at the proximal LAD with thrombus grade 5 and TIMI 0 flow; (B): a refractory thrombus with TIMI 2 flow; (C): aspiration with thrombuster II aspiration catheter; (D): a refractory thrombus after aspiration; (E): aspiration with Heartrail II 5F child catheter; (F): a TIMI 3 flow and no thrombus burden in LAD after stenting. LAD: left anterior descending; SMI: subacute myocardial infarction; TIMI:thrombolysis in myocardial infarction.
Additionally, the child catheter is also worth a try if the Export thrombus aspiration catheter is ineffective in extracting the refractory thrombus. A 39-year-old man presented with typical angina for one week. Electrocardiogram showed pathological Q waves in II, III and aVF leads. The cardiac enzyme was normal. Angiography revealed a total occlusion at the mid RCA with thrombus grade 5 and TIMI 0 flow (Figure 3A). A 7 Fr AL1.0 guiding catheter (Terumo,Tokyo, Japan) was advanced to the RCA ostium via right femoral access. Runthrough NS guidewire (Terumo, Tokyo,Japan) was passed through the lesion. An Export AP aspiration catheter (Medtronic Inc.) was used for thrombus aspiration (Figure 3B). Angiography showed there was still refractory thrombus with TIMI 2 flow (Figure 3C). Then, a Heartrail II 5F child catheter (Terumo, Tokyo, Japan) was advanced into the mid and distal part of RCA for aspiration using distal anchoring balloon (Figures 3D&3E). The following angiography showed TIMI 3 flow in RCA, significantly decreased thrombus burden and no apparent stenosis at the mid RCA (Figure 3F).
Residual refractory thrombus is related to a higher occurrence of the no-reflow phenomenon.[7]Previous studies have revealed that the application of routine thrombus aspiration devices could not achieve the superiority compared with conventional PCI for STEMI patients. In TAPAS trial,effective thrombus aspiration was achieved in only 73% of STEMI patients assigned to routine thrombus aspiration.[8]The main reason was that current devices for thrombus aspiration could not be completely effective in removing the residual thrombus.
Patients with SMI may display heavy thrombus burden.Thrombus dislodgment and thrombus composition are the two major factors that influence the efficiency of conventional thrombectomy. Mechanical thrombus movement may lead to distal embolization and subsequently cause microvascular injury and enlarge the necrotic area.[5,6]In addition, thrombus composition is another major factor. In the stage of evolving infarction, thrombotic material is full of fibrin content with less platelet content, and the thrombotic material is possibly less suited for aspiration.
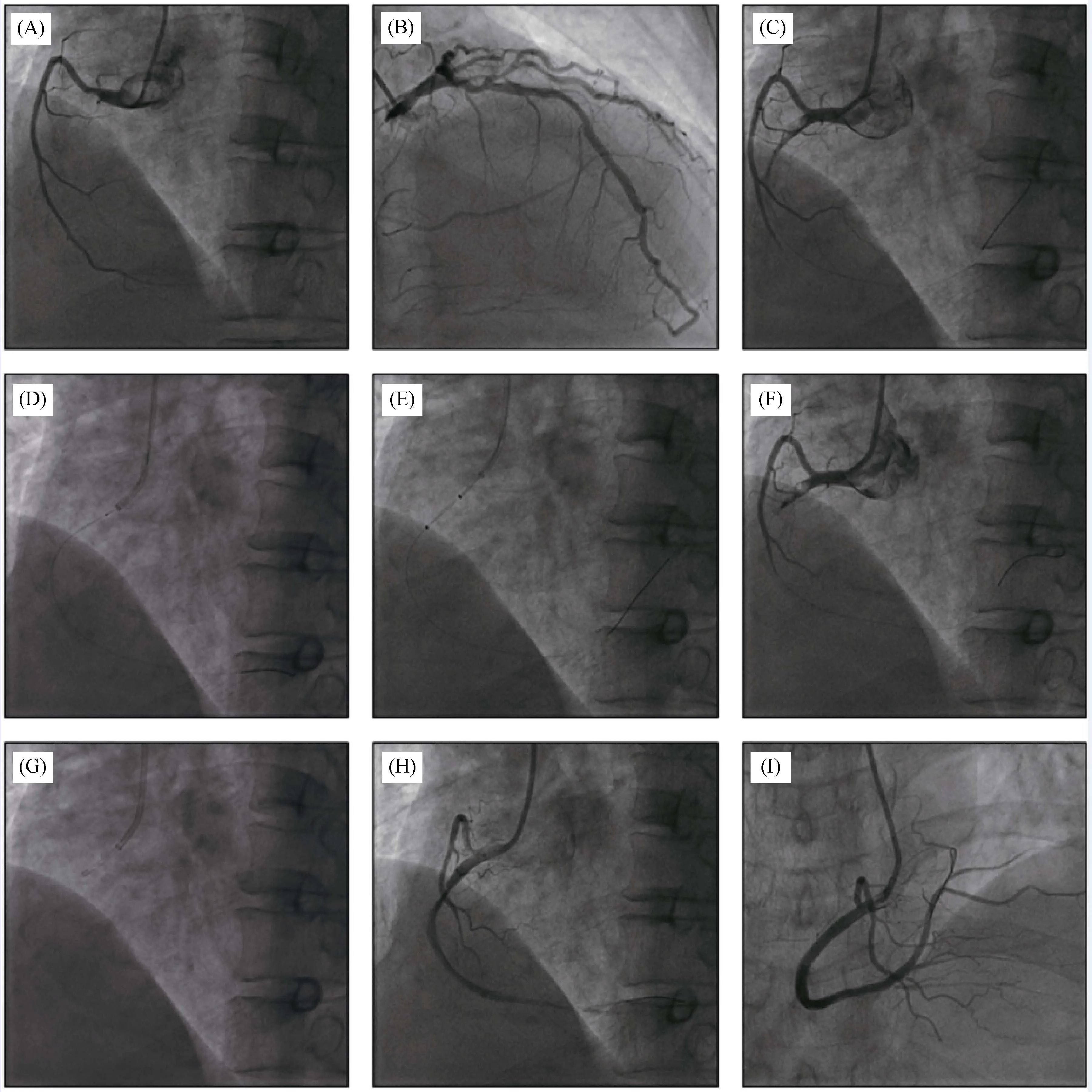
Figure 2. Application of the child catheter aspiration after the Thrombuster II and the Angiojet mechanical aspiration catheters failure in a SMI patient. (A): A total occlusion in the proximal part of RCA; (B): a non-significant lesions in LCA and the collateral circulation from LCA to distal RCA; (C): heavy thrombus burden with TIMI 0 flow; (D): Thrombuster II aspiration catheter aspiration; (E): Angiojet mechanic catheter aspiration; (F): a residual refractory thrombus with TIMI 0 flow; (G): aspiration with Heartrail II 5F child catheter;(H): TIMI 3 flow in RCA, significantly lessened thrombus burden and severe stenosis at proximal and distal RCA; (I): final result. LCA: left coronary artery; RCA: right coronary artery; SMI: subacute myocardial infarction; TIMI: thrombolysis in myocardial infarction.
There are many methods of dealing with the problem, but they are not fully effective. Although the Rheolytic thrombectomy has been found useful, a recent meta-analysis has related them to a neutral impact on survival and a significant increase in mortality.[9]A previous study suggested that the 5F child catheter aspiration could significantly reduce thrombus burden and improve the coronary flow in patients presenting with AMI.[10]In vitro, the thrombus is semisolid;and therefore lumen morphology of thrombus aspiration catheter is one of the important factors to determine the efficiency of thrombus aspiration. Theoretically, catheters with a circular lumen are superior to those with a semilunar lumen in terms of thrombus aspiration ability. The 5F child catheter has a circular lumen, and it is considered to possess better aspiration capacity. In addition, according to Poiseuille's Law, blood flow in the catheter is proportional to the fourth power of its radius. The lumen diameter of the 5F child catheter is 0.059 inch, whereas the lumen diameter of an 6F Export thrombus aspiration catheter is 0.043 inch.So the aspiration ability of the 5F child catheter is about 3.5 times better than the 6F Export catheter. The 5F child catheter may be a more effective device to treat the refractory thrombus in SMI patients.
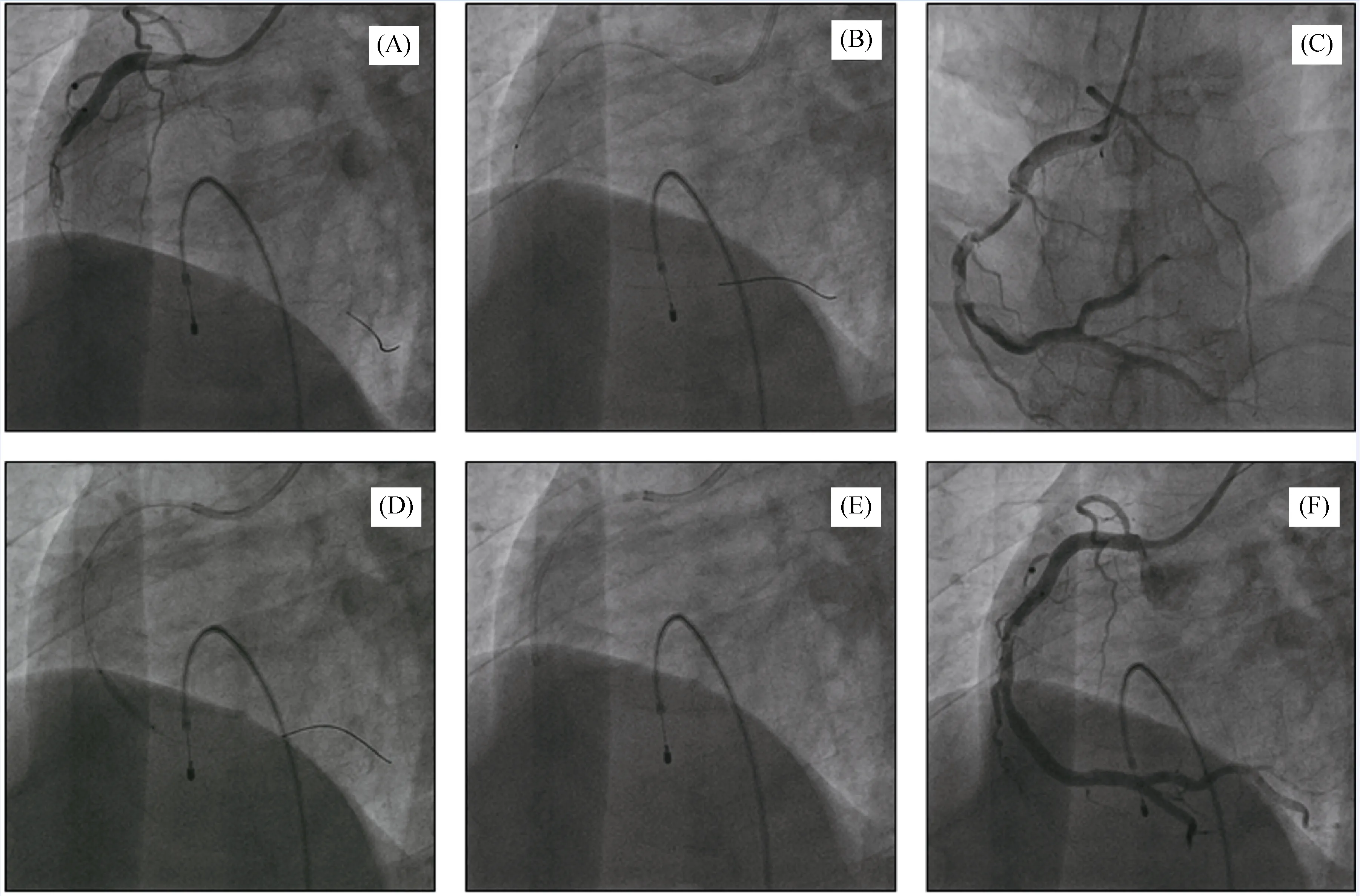
Figure 3. Application of the child catheter aspiration after the Export aspiration catheter failure in a SMI patient. (A): A total occlusion at the mid RCA with thrombus grade 5 and TIMI 0 flow; (B): export AP catheter aspiration; (C): a refractory thrombus with TIMI 2 flow; (D): aspiration with Heartrail II 5F child catheter in mid part of RCA by aiding of distal anchoring balloon; (E): aspiration with Heartrail II 5F child catheter in distal part of RCA; (F): TIMI 3 flow in RCA, decreased thrombus burden, and no apparent stenosis at mid of RCA.RCA: right coronary artery; SMI: subacute myocardial infarction; TIMI: thrombolysis in myocardial infarction.
In this report, the 5F child catheter was successfully used to remove the refractory thrombus in three patients with SMI. All these patients experienced the failed thrombectomy by routine thrombus aspiration devices, while after being retrieved by the 5F child catheter, the refractory thrombus was lessened completely or significantly. There were no peri-procedural complications or post-procedural complications such as distal embolization and no-reflow in these three patients. We recommend that the 5F child catheter is suitable for removing residual refractory thrombus after the routine thrombus aspiration failure in SMI patients.Of note, this technique should be avoided in the proximal part of the target vessel with tortuosity, calcification or severe angels and in vessels with diameters less than 2.5 mm as well. Anchoring balloon technique can help the child catheter advance to the distal part of coronary arteries.
In conclusion, SMI patients usually have high thrombus burden and sometimes the removal of thrombus could be very challenging. We described a safe and effective approach to remove the residual refractory thrombus in patients with SMI using the 5F child catheter, which may provide a reasonable option when the conventional thrombus aspiration devices fail.
Acknowledgments
The authors declare that there is no conflict of interest.
登錄APP查看全文
 Journal of Geriatric Cardiology
2019年2期
Journal of Geriatric Cardiology
2019年2期
- Journal of Geriatric Cardiology的其它文章
- A rare case of primary well-differentiated angiosarcoma of the right atrium
- Impact of main vessel calcification on procedural and clinical outcomes of bifurcation lesion undergoing provisional single-stenting intervention:a multicenter, prospective, observational study
- Bleeding risk assessment in elderly patients with acute coronary syndrome
- Frailty and acute coronary syndrome: does gender matter?
- Frailty in patients admitted to hospital for acute coronary syndrome: when,how and why?
- Clinical and prognostic implications of delirium in elderly patients with non–ST-segment elevation acute coronary syndromes