Analysis of spectrum and drug sensitivity of bacteria in the aqueous humor or vitreous of patients at an early stage of penetrating ocular trauma
2016-05-17 03:32:16YanFenHuNiTianYueZhenGuoHuiYingLi
國際眼科雜志 2016年5期
Yan-Fen Hu, Ni Tian, Yue-Zhen Guo, Hui-Ying Li
Foundation items:Nansha District, Guangzhou City People’s Livelihood Project (2014-MS-03); the Medicine Strong Province Project, Guangdong Province Administration of Traditional Chinese Medicine (20132004)
1Department of Ophthalmology, the Sixth Hospital of Nansha District, Guangzhou 511470, Guangdong Province, China
2Department of Ophthalmology, the First Affiliated Hospital of Guangzhou University of Traditional Chinese Medicine, Guangzhou 511470, Guangdong Province, China
Correspondence to:Ni Tian. Department of Ophthalmology, the First Affiliated Hospital of Guangzhou University of Traditional Chinese Medicine, Guangzhou 510405, Guangdong Province, China. tianni213@126.com
Received: 2015-07-20 Accepted: 2016-02-22
眼球穿孔傷患者早期前房房水或玻璃體細菌學培養(yǎng)分析
胡燕芬1,田 妮2,郭月珍1,李慧英1
(作者單位:1511470 中國廣東省廣州市,南沙區(qū)第六人民醫(yī)院眼科;2511470 中國廣東省廣州市,廣州中醫(yī)藥大學第一附屬醫(yī)院眼科)
?
Analysis of spectrum and drug sensitivity of bacteria in the aqueous humor or vitreous of patients at an early stage of penetrating ocular trauma
Yan-Fen Hu1, Ni Tian2, Yue-Zhen Guo1, Hui-Ying Li1
Foundation items:Nansha District, Guangzhou City People’s Livelihood Project (2014-MS-03); the Medicine Strong Province Project, Guangdong Province Administration of Traditional Chinese Medicine (20132004)
1Department of Ophthalmology, the Sixth Hospital of Nansha District, Guangzhou 511470, Guangdong Province, China
2Department of Ophthalmology, the First Affiliated Hospital of Guangzhou University of Traditional Chinese Medicine, Guangzhou 511470, Guangdong Province, China
Correspondence to:Ni Tian. Department of Ophthalmology, the First Affiliated Hospital of Guangzhou University of Traditional Chinese Medicine, Guangzhou 510405, Guangdong Province, China. tianni213@126.com
Received: 2015-07-20Accepted: 2016-02-22
眼球穿孔傷患者早期前房房水或玻璃體細菌學培養(yǎng)分析
胡燕芬1,田妮2,郭月珍1,李慧英1
(作者單位:1511470 中國廣東省廣州市,南沙區(qū)第六人民醫(yī)院眼科;2511470 中國廣東省廣州市,廣州中醫(yī)藥大學第一附屬醫(yī)院眼科)
Abstract
?AIM:To analyze the spectrum and antibiotic sensitivity of bacteria in the aqueous humor and vitreous immediately following the occurrence of penetrating ocular trauma.
?METHODS: Aqueous humor or vitreous specimens were collected from 45 eyes of 45 patients with penetrating ocular trauma before operations. The specimens were prepared for bacterial culture and the associated sensitivity tests to several commonly used antibiotics.
?RESULTS: Fifteen eyes of all the patients were found to be positive with bacterial infection, and the most frequently identified bacteria was staphylococcus epidermidis, which accounted for 67.7% (10/15) of all identified cases. All identified bacteria were sensitive to ciprofloxacin and ofloxacin, and less sensitive to cefoperazone. Most of them were resistant to gentamycin, rifampin and chloramphenicol. Accompanying intraocular foreign body or sclera wound were associated with positive bacterial cultures (χ12=6.544,P1=0.016;χ22=4.5,P2=0.034). Causes of injury(χ2=1.667,P=0.197), lens rupture (χ2=1.125,P=0.352) or locations where the specimen was collected (χ2=1.667,P=0.197) did not contribute to the difference in the positive rates of bacterial cultures.
?CONCLUSION:In patients with penetrating ocular trauma, the major bacteria entering into the eye was staphylococcus epidermidis. Fluro-Quinolones can be used as the first-line antibiotics for prophylactic treatment. Cefoperazone can be taken as a second choice.
KEYWORDS:?penetrating ocular trauma; bacterial culture; aqueous humor; vitreous
Citation:Hu YF, Tian N, Gue YZ, Li HY. Analysis of spectrum and drug sensitivity of bacteria in the aqueous humor or vitreous of patients at an early stage of penetrating ocular trauma.GuojiYankeZazhi(IntEyeSci) 2016;16(5):818-821
INTRODUCTION
Penetrating ocular trauma is a commonly seen type of ocular trauma, which is often complicated by bacterial infection. Bacterial infections can be very harmful to the traumatized eye and even can sometimes destroy the whole eye. It can be of great clinical significance to have a deep insight into the spectrum and drug sensitivity of commonly seen pathogenic bacteria in eyes at an early stage of the penetrating ocular trauma. In this study, we collected samples from 45 patients (45 eyes) of penetrating ocular trauma who were sent to our hospital within 24h after trauma. We analyzed the spectrum and drug sensitivity of bacteria in the aqueous humor or the vitreous.
SUBJECTS AND METHODS
The study was approved by our ethics committee. Written informed consent was obtained from all participating patients, and the principles of the Declaration of Helsinki were followed. Forty-five eyes of 45 patients with penetrating ocular trauma, received treatment in our hospital within 24h after a penetrating ocular trauma. None of the study subject received any treatment prior to being sent to our hospital. Thirty-one of the subjects were male and 14 were female. They were aged from 4 to 50y and the average age was 20.8y. Among the 45 eyes, 27 were hurt by metal objects. The remaining 18 were hurt by non-metal objects.
We collected the aqueous humor and vitreous before cleaning the eye and performing the operation. The conjunctival sac was not rinsed with mercury bichloride or antibiotics before the operation. Only gentle eyelid and face hygiene were performed. Aqueous humor samples were collected from eyes with existing anterior chamber and penetrating corneal wounds. For those with penetrating scleral wounds and flat anterior chambers, the vitreous body was selected for sample collection. The samples were injected into the culture tubes immediately after collection and then sent to the laboratory for bacterial culture. The aqueous humor was collected with the following method: If the cornea was intact, we entered the anterior chamber at the limbus with an 1 mL disposable syringe and drew 0.1 mL of aqueous humor in. If the cornea was penetrated, the anterior chamber was then entered through the corneal wound. The method for vitreous collection was if the wounded eye was aphakic with ruptured posterior capsule, the anterior chamber was entered at the limbus with a 2 mL disposable syringe. The needle of the syringe was then passed through the pupil into the vitreous cavity. About 0.2-0.3 mL of vitreous was then drawn into the syringe. For the eyes with intact lens or IOLs, the vitreous samples were collected through the pars plana.
The aqueous humor or vitreous samples were placed into the both culture tubes or blood agar plates, and underwent bacterial culture. Drug sensitivity tests were performed using the disk diffusion method for samples with positive bacterial cultures. The paper discs used in the drug sensitivity tests were provided by the Beijing Tiantan Biotechnology Corporation. Each paper disc contains: cefoperazone 75 μg, ofloxacin 5 μg, ciprofloxacin 5 μg, gentamycin 10 μg, chloramphenicol 30 μg, rifampicin 5 μg and tobramycin 10 μg. Sensitivity to each type of antibiotic drug was rated as resistant, moderately sensitive and sensitive.
Chi-square tests were performed using the SPSS 13.0 statistic software (SPSS Inc., USA). The correlations were analyzed between bacterial culture results and cause of trauma, wound locations, intraocular foreign body, damages to the lens and the location of sample collection.
RESULTS
Eighteen vitreous and 27 aqueous samples were sent for bacterial culture and drug sensitivity tests.
Results of Bacterial Culture and Drug Sensitivity TestsBacterial cultures were positive in 15 samples (8 vitreous and 7 aqueous humor) and negative in the remaining 30. The positive rate was 33.3%. Among the positive results, 12 were Gram positive and 3 were Gram negative. The pathogenic bacterium was identified to be staphylococcus epidermidis (67.7%) in 10 of the 12 Gram positive cases and other species in the remaining 2. Drug sensitivity test showed that: In the 10 cases of staphylococcus epidermidis infection, 5 were sensitive to all tested antibiotics; 2 were resistant to gentamycin and tobramycin while being sensitive to the other drugs. On the whole, both Gram positive and Gram negative bacteria were resistant to gentamycin, tobramycin, chloramphenicol and rifampicin, moderately sensitive to cefoperazone and sensitive to ciprofloxacin and ofloxacin.
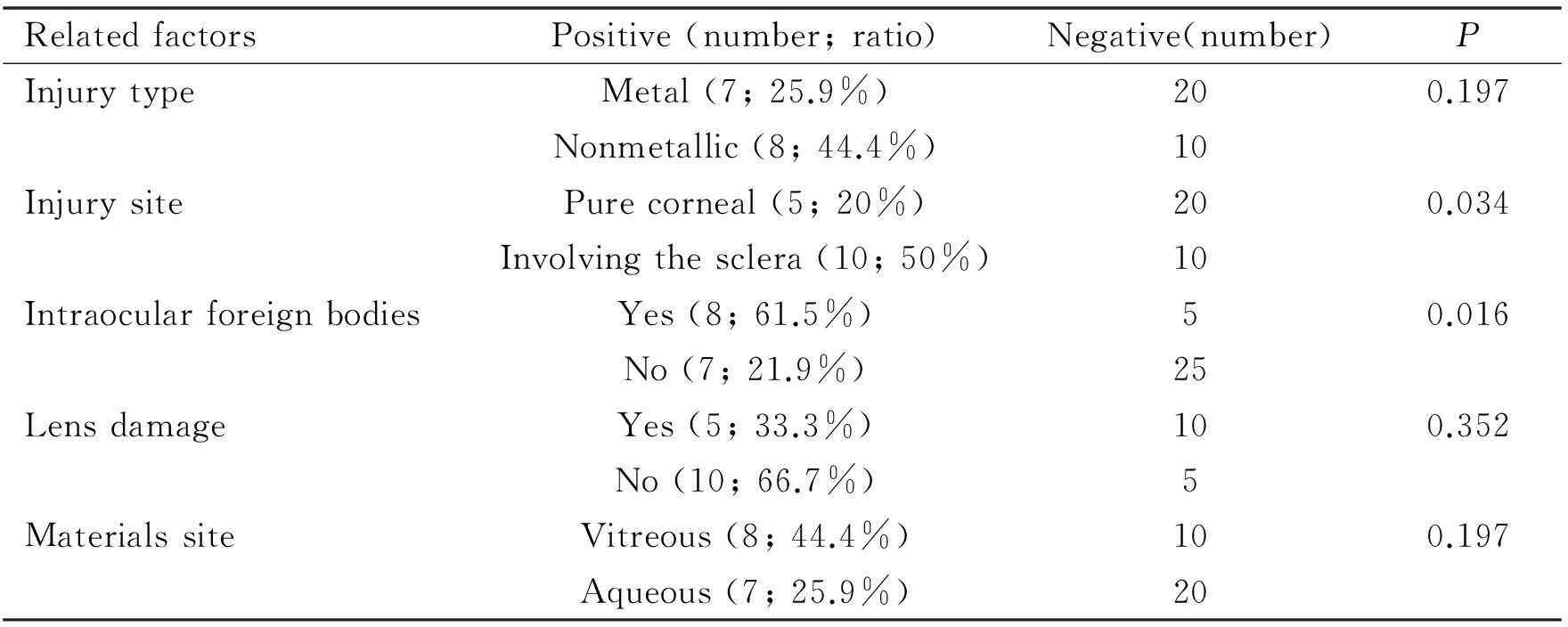
Effects of Correlative Factors on Bacterial CultureType of instruments that cause the ocular trauma were: metal in 27 eyes, among which 7 (25.9%) were positive in bacterial cultures; nonmetal in 18 eyes, 8 of which (44.4%) had positive bacterial cultures. No significant difference was found in the bacterial infection rate between traumas caused by metal and nonmetal instruments (χ2=1.667,P=0.197) (Table 1).
Locations of the penetrating wounds:In the 25 eyes of simple cornea wounds, 5 (20%) had positive bacterial cultures; in the 20 eyes complicated by scleral perforation, 10 (50%) had positive in bacterial cultures. Eyes complicated by scleral perforation had significantly higher positive rate of positive bacterial culture (χ2=4.5,P=0.034) (Table 1).
Intraocular foreign body: Intraocular foreign body were found in 13 eyes, in which 8 (61.5%) had positive bacterial cultures including 5 positive for staphylococcus epidermidis, 3 for Gram negative bacilli. Only 7 of the 32 eye without intraocular foreign bodies had positive bacterial cultures, 5 of which were positive for staphylococcus epidermidis, 2 for Gram positive cocci. The positive rate of bacterial culture was significantly higher in eyes with intraocular foreign bodies than those without (χ2=6.544,P=0.016) (Table 1).
Lens damage: among the 15 eyes complicated by lens damage, 5(33.3%) were positive in bacterial cultures. However, in those without, 10 of the 15 eyes (66.7%) had positive bacterial cultures. Comparing the positive rates of bacterial cultures between eye with and without lens damage,no difference was found to be statistically significant (χ2=1.125,P=0.352) (Table 1).
Table 1The correlation factors to affect the results of the bacteria cultures
RelatedfactorsPositive(number;ratio)Negative(number)PInjurytypeMetal(7;25.9%)200.197Nonmetallic(8;44.4%)10InjurysitePurecorneal(5;20%)200.034Involvingthesclera(10;50%)10IntraocularforeignbodiesYes(8;61.5%)50.016No(7;21.9%)25LensdamageYes(5;33.3%)100.352No(10;66.7%)5MaterialssiteVitreous(8;44.4%)100.197Aqueous(7;25.9%)20
Locations of sample collection:samples were collected from the vitreous cavity in 18 eyes, among which 8 (44.4%) had positive bacterial cultures. The bacterial cultures were positive in 7 of the 27 eyes with samples collected from the anterior chambers. No significant difference in the positive rate of bacterial culture was found between samples collected from vitreous cavities and the anterior chambers (χ2=1.667,P=0.197) (Table 1).
DISCUSSION
Bacterial endophthalmitis is an serious complication of the penetrating ocular trauma[1-5]. It usually occurs within the first 24 to 48h after the trauma[6-12]. Recent studies have shown that staphylococcus epidermidis is a major pathogenic bacterium that causes bacterial endophthalmitis[13-19]. Our study also showed that staphylococcus epidermidis was the main factor (67.7%) invading the eye after the trauma. It can be assumed that there must be a strong correlation between bacteria existing in the eye after the trauma and the pathogens of bacterial endophthalmitis.
The result of our study showed that the positive rates of bacterial cultures in eyes with intraocular foreign bodies and complicated scleral wounds were significantly higher than those without foreign bodies and with simple corneal wounds. However, no correlation was found between bacterial culture results and the type of instruments that caused the traumas or the locations of sample collection. In a penetrated eye, the integrity of the eye ball was damaged. Pathogenic bacteria can enter the eye with foreign bodies. Even normal flora of the conjunctival sac and eyelid skin can invade the eye through the penetrating ocular wounds or with intraocular foreign bodies. Since most foreign bodies can carry bacteria, the rate of existence of bacteria in the eye is apparently higher in eyes with ocular foreign bodies. The higher positive rate in eyes with complicated scleral wounds might associate with the extension of the ocular wounds, which is easier for invasion of the pathogenic bacteria.
Investigators has proposed assumptions in previous publications that the exposed lens cortex can probably provide essential nutrients for the growth of pathogenic bacteria[20]. Moreover, the diffusion of lens cortex into the aqueous humor can compromise the elimination of bacteria by normal clearance of aqueous humor. In that case, the positive rate of bacterial culture should be higher in eyes with lens damage. However, this assumption is not supported by our results (χ2=1.125,P=0.352). One possible reason might be that in our case series, most of the cases without lens damage had intraocular foreign bodies, which can raise the positive rate of bacterial cultures. It has been anecdotal recognition that the positive rate of bacterial cultures for vitreous should be higher than that of the aqueous humor. However, our study showed that the locations of sample collection has no significant association with the results of bacterial cultures (χ2=1.667,P=0.197). The altered intraocular environment caused by the penetrating ocular trauma.
According to the drug sensitivity tests in our study, all the detected bacteria were sensitive to ciprofloxacin and ofloxacin. Most of the bacteria were resistant to chloramphenicol. The drug resistance to gentamycin and tobramycin was also pretty high. From this, it can be seen that although chloramphenicol was ever regarded as a first-line antibiotic drug, the drug resistance to chloramphenicol has been raised due to abusive use of this drug in the clinical practice in China during the past several decades. Consequently, we should avoid using chloromycetin in the treatment of penetrating ocular trauma for fear of failure in the efforts of preventing secondary infection. Gentamycin and tobramycin, recently being widely used in clinical practice, were also shown in our study to have high drug resistance. Caution should be taken when considering the use of these drugs. In contract, our study also showed that both Gram positive cocci and Gram negative bacilli were sensitive to ciprofloxacin and ofloxacin. Accord to this finding, we suggest that the generally used second-generation quinolones can be considered as first-line antibiotics for the prophylactic anti-infective treatment of penetrating ocular trauma. It is worth attention that extra caution is needed for the systemic application of quinolones in children since this species of antibiotic drugs can exert adverse influence on the development of cartilage in children’s bodies. As to cefoperazone, since most of the pathogenic bacteria are sensitive to it in our study, it can be chosen a second-line antibiotic agent. In addition, we suggest that a comprehensive analysis of commonly seen pathogenic bacteria and their drug sensitivities should be performed every 2-3y so as to provide basis to evidence-based clinical practice.
REFERENCES
1 Asencio MA, Huertas M, Carranza R, Tenías JM, Celis J, González-Del Valle F. Microbiological study of infectious endophthalmitis with positive culture within a 13 year-period.RevEspQuimioter2014;27(1):22-27
2 Long C, Liu B, Xu C, Jing Y, Yuan Z, Lin X. Causative organisms of post-traumatic endophthalmitis: a 20-year retrospective study.BMCOphthalmol2014;14:34
3 Durand ML. Endophthalmitis.ClinMicrobiolInfect2013;19(3):227-234
4 Bhala S, Narang S, Sood S, Mithal C, Arya SK, Gupta V. Microbial contamination in open globe injury.NepalJOphthalmol2012;4(1):84-89
5 T?lu S, Bembea D, Sebestyen E, Toader L, Shah H. Traumatic endophthalmitis--terapeutical indications and results.Ophthalmologia2010;54(4):103-108
6.Zhang XF, Yang JX.Eyetrauma. Henan medical university Press. 1997;41
7 Kernt M, Kampik A. Endophthalmitis: Pathogenesis, clinical presentation, management, and perspectives.ClinOphthalmol2010;4:121-135
8 Safneck JR. Endophthalmitis: A review of recent trends.SaudiJOphthalmol2012;26(2):181-189
9 Jaramillo S, Varon CL. Curvularia lunata endophthalmitis after penetrating ocular trauma.RetinCasesBriefRep2013;7(4):315-318
10 Berbel RF, Casella AM, de Freitas D, H?fling-Lima AL. Curvularia lunata endophthalmitis.JOculPharmacolTher2011;27(5):535-537
11 Ahmed Y, Schimel AM, Pathengay A, Colyer MH, Flynn HW Jr. Endophthalmitis following open-globe injuries.Eye(Lond) 2012;26(2):212-217
12 Jaramillo S, Varon CL. Curvularia lunata endophthalmitis after penetrating ocular trauma.RetinCasesBriefRep2013;7(4):315-318
13 Sabaci G, Bayer A, Mutlu FM, Karagül S, Yildirim E. Endophthalmitis after deadly-weapon-related open-globe injuries: risk factors, value of prophylactic antibiotics, and visual outcomes.AmJOphthalmol2002;133(1):62-69
14 Parke DW 3rd, Pathengay A, Flynn HW Jr, Albini T, Schwartz SG. Risk factors for endophthalmitis and retinal detachment with retained intraocular foreign bodies.JOphthalmol2012;2012:758526
15 Nicoar? SD, Irimescu I, C?linici T, Cristian C. Outcome and prognostic factors for traumatic endophthalmitis over a 5-year period.JOphthalmol2014;2014:747015
16 Xiao QG, Liang D, Liu ZG, Wang ZF. The results of 127 patients exogenous endophthalmitis about pathogens and drug susceptibility.ChineseJournalofPracticalOpthalmology2003;21(4):299-302
17 Duch-Samper AM, Menezo JL, Hurtado-Sarrió M. Endophthalmitis following penetrating eye injuries.ActaOphthalmolScand1997;75(1):104-106
18 Dave SB, Toma HS, Kim SJ. Ophthalmic antibiotic use and multidrug-resistant staphylococcus epidermidis: a controlled, longitudinal study.Ophthalmology2011;118(10):2035-2040
19 Thompson WS, Rubsamen PE, Flynn HW Jr, Schiffman J, Cousins SW. Endophthalmitis after penetrating trauma. Risk factors and visual acuity outcomes.Ophthalmology1995;102(11):1696-1701
20 Shailaja S, Kamath Y, Hazarika M, Vishwanath S. Acute post-traumatic endophthalmitis secondary to Propionibacterium acnes.BMJCaseRep2013;2013
摘要
關鍵詞:眼球穿孔傷;細菌培養(yǎng);房水;玻璃體
DOI:10.3980/j.issn.1672-5123.2016.5.06
通訊作者:田妮,中山眼科中心,博士研究生,主任醫(yī)師(教授),碩士研究生導師,研究方向:白內障、眼整形、眼外傷、眼底病. tianni213@126.com
作者簡介:胡燕芬,廣州醫(yī)學院,本科,主管護師,研究方向:醫(yī)院感染管理。
基金項目:廣州市南沙區(qū)民生項目 (2014-MS-03);廣東省中醫(yī)藥管理局中醫(yī)強省項目 (20132004)
目的:了解眼球穿通傷患者早期眼內組織細菌學培養(yǎng)及藥物敏感情況。
方法:對本院2003-07/09收治的受傷時間在24h以內的45例45眼眼球穿通傷患者的前房水或玻璃體進行細菌培養(yǎng)及藥敏實驗,并對其結果進行分析。
結果:共15例(33.3%)(玻璃體培養(yǎng)8例、房水培養(yǎng)7例)細菌培養(yǎng)結果陽性,其中10例為表皮葡萄球菌(67.7%)。所有細菌均對環(huán)丙沙星、氧氟沙星敏感,對頭孢哌酮較為敏感,大部分對慶大霉素、氯霉素、利福平耐藥。球內有異物存留(χ2=6.544,P=0.016)、傷口累及鞏膜(χ2=4.5,P=0.034)者細菌培養(yǎng)結果陽性率高,而致傷物類型(χ2=1.667,P=0.197)、有無合并晶狀體損傷(χ2=1.125,P=0.352)、取材部位(χ2=1.667,P=0.197)對細菌培養(yǎng)結果無明顯影響。
結論:表皮葡萄球菌是眼球穿通傷后進入眼內的主要細菌。對眼球穿通傷患者預防性用藥可首選喹諾酮類藥物,次選頭孢哌酮。
引用:胡燕芬,田妮,郭月珍,李慧英. 眼球穿孔傷患者早期前房房水或玻璃體細菌學培養(yǎng)分析.國際眼科雜志2016;16(5):818-821
·Original article·
