肘關節“恐怖三聯征”的手術治療:附14例報告
2015-06-27 00:50:51孟亞軻劉巖葉添文歐陽躍平陳愛民郭永飛
中華肩肘外科電子雜志 2015年3期
孟亞軻 劉巖 葉添文 歐陽躍平 陳愛民 郭永飛
?
肘關節“恐怖三聯征”的手術治療:附14例報告
孟亞軻 劉巖 葉添文 歐陽躍平 陳愛民 郭永飛
目的 回顧分析手術治療肘關節“恐怖三聯征”的療效及策略。方法 我院骨科從2010年7月至2013年10月手術治療并完整隨訪的14例肘關節“恐怖三聯征”患者,其中尺骨冠突骨折按照Regan-Morrey分型:Ⅰ型2例,Ⅱ型10例,Ⅲ型2例;橈骨頭骨折按照Mason 分型:Ⅰ型4例,Ⅱ型7例,Ⅲ型3例;本組病例中均合并有肘關節內、外側副韌帶的損傷。采取常規肘關節內、外側聯合入路,給予患肘關節復位,然后由深至淺依次固定冠狀突骨折和橈骨頭骨折,修復外側副韌帶。冠狀突骨折采用微型鋼板、拉力螺釘、縫合錨釘及套索縫合技術固定;橈骨頭骨折采用克氏針、微型螺釘或微型鋼板固定;所有患者給予編織非吸收性縫線縫合或錨釘修復外側副韌帶(lateral collateral ligaments,LCL),2例使用非吸收性編織縫線縫合、錨釘修復內側副韌帶(medical collateral ligaments,MCL),1例放置外側鉸鏈式外固定支架,余13例患者術后給予肘關節屈曲90°、前臂中立位石膏固定,術后積極進行康復功能鍛煉。結果 平均隨訪18個月(10~37個月)。所有病例實現骨折愈合,平均愈合時間為12.4周。術后6個月,肘關節屈位(0°~20°),伸位(130°~145°),平均活動范圍為116.5°;旋前(60°~85°),旋后(45°~75°),平均旋轉范圍為126°。1例患者出現肘關節僵硬;2例患者術后6個月在影像學上出現異位骨化,但不影響肘關節功能。結論 肘關節“恐怖三聯征”通過積極有效的手術治療,大多患者能夠得到滿意的結果。對于該類損傷,我們應盡可能通過有效的內固定重建骨及韌帶的穩定結構,恢復肘關節的穩定性,及早配合正規的功能鍛煉,最大程度恢復肘關節的功能。
肘關節;恐怖三聯征;骨折;脫位;固定
肘關節“恐怖三聯征”是指肘關節后脫位合并尺骨冠狀突骨折和橈骨頭骨折,常伴有肘關節內、外側副韌帶的損傷。軸向應力作用于前臂旋后、肘關節外展產生的壓縮剪切力是主要的損傷機制[1]。我科自2010年7月至2013年10月手術治療并完整隨訪了14例肘關節“恐怖三聯征”患者,治療效果較好,現報道如下。
資 料 與 方 法
一、一般資料
本組患者14例,男性11例,女性3例,年齡23~48歲,平均35.4歲。左側5例,右側9例,均為閉合性損傷。無相關神經血管損傷。致傷原因:高處墜落5例,交通事故3例,跌倒損傷4例,運動損傷2例。入院后常規行肘關節X線正側位片、肘關節CT掃描及三維重建以判斷骨折的類型及移位情況(圖1、2)。尺骨冠突骨折Regan-Morrey分型[2],Ⅰ型2例,Ⅱ型10例,Ⅲ型2例;橈骨頭骨折按照Mason 分型[3],Ⅰ型4例,Ⅱ型7例,Ⅲ型3例;其中1例合并有同側橈骨遠端骨折,1 例合并有同側尺骨干骨折;本組病例均合并有肘內、外側副韌帶的損傷。
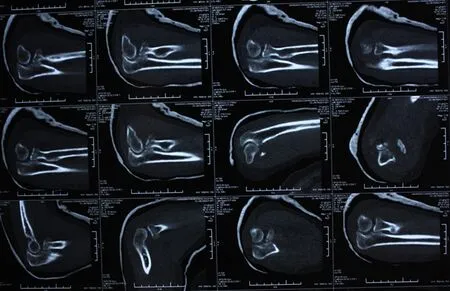
圖2 肘關節CT平掃
二、手術方法
患者平臥于手術臺上,患肢近端上充氣性止血帶。在臂叢神經阻滯麻醉下,常規使用肘關節內、外側聯合入路,給予患肘關節復位,然后由深至淺依次修復冠狀突骨折,前關節囊,橈骨頭骨折,外側副韌帶,伸肌總腱起點。冠狀突骨折采用微型鋼板、拉力螺釘、縫合錨釘或套索縫合技術固定;橈骨小頭骨折采用克氏針、微型螺釘、微型鋼板固定;所有患者使用非吸收性編織縫線縫合或錨釘給予修復外側副韌帶(lateral collateral ligaments,LCL)。閉合切口前行肘關節伸直位內外翻試驗及外翻過載試驗判斷肘關節穩定性的恢復情況。其中3例肘關節被動屈曲過程中同心圓穩定性欠佳,其中2例使用非吸收性編織縫線縫合、錨釘修復內側副韌帶(medical collateral ligaments,MCL),1例放置外側鉸鏈式外固定支架,術中保持肘關節屈曲90°固定鉸鏈,另12例穩定性尚可維持。術后13例患者給予肘關節屈曲90°、前臂中立位石膏固定。

圖1 術前肘關節正側位X線片
三、功能鍛煉及隨訪
13例石膏固定患者做手指活動及肱二頭肌、肱三頭肌等長收縮訓練;術后48 h開始進行肘關節被動屈伸活動,及前臂旋轉活動。1例輔以外固定架固定的患者術后1~2周開始進行功能鍛煉,術后第1周,調整鉸鏈支架中心的旋鈕,指導患肘做屈伸功能鍛煉,術后6~8周拆除外固定支架。康復過程中避免肘關節過伸。 術后分別于第1天, 2周,1、3、6、12個月隨訪時拍攝患肘關節正側位X線片。術后2個月肘關節正側位X線片見圖3。觀察骨折塊愈合及異位骨化、骨關節炎等術后并發癥的發生情況;了解肘關節功能改善情況,指導患者進行功能鍛煉。隨訪結束時按Mayo肘關節功能評分標準進行療效評價。
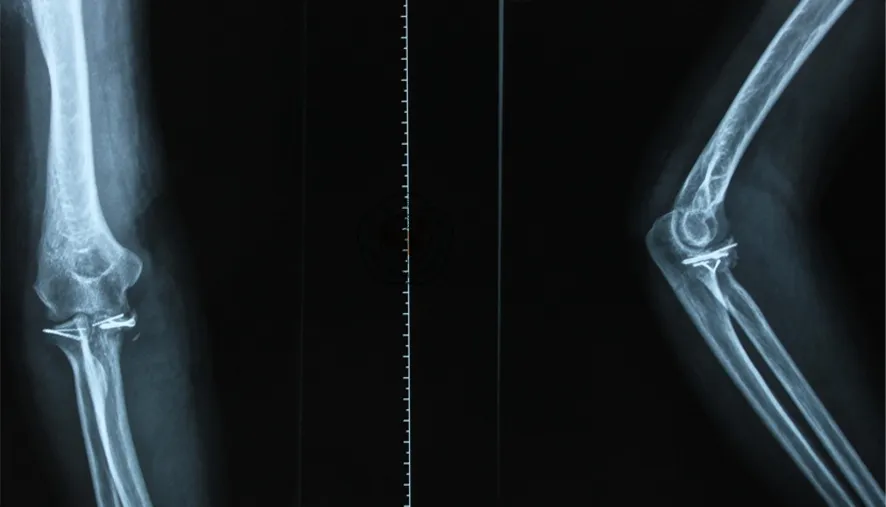
圖3 術后2個月肘關節正側位X線片
結 果
本組隨訪14例,平均隨訪18個月(10~37個月)。骨折達臨床愈合時間為術后10~15周,平均12.4周。術后6個月,肘關節屈位(0°~20°),伸位(130°~145°),平均活動范圍為116.5°;旋前(60°~85°),旋后(45°~75°),平均旋轉范圍為126°。1例出現肘關節僵硬;2例患者術后6個月在影像學上出現異位骨化,但不影響肘關節功能。Mayo評分標準評價:優6例,良4例,一般2例,差1例。
討 論
1996年Hotchkiss[4]首次將肘關節后脫位合并尺骨冠突和橈骨頭骨折命名為肘關節“恐怖三聯征”,該類患者多合并有周圍韌帶的損傷,屬于嚴重類型的肘關節損傷。肘關節三維結構復雜,治療不當會導致疼痛、僵硬、異位骨化、創傷性關節炎等并發癥。肘關節“恐怖三聯征”的主要治療目標[5]是重建重要的骨性關節及軟組織結構,恢復運動關節的穩定性,為術后早期功能鍛煉提供條件。大多數學者[6]建議對所有骨折的橈骨頭和冠突給予牢固固定,修復外側副韌帶,實現肘關節的解剖穩定性。在少數情況下,對于殘存的不穩定性可通過修復內側副韌帶或加用鉸鏈式外固定架固定治療。
目前肘關節“恐怖三聯征”常用的手術入路有外側入路、外內側聯合入路和后側入路。國內林國葉等[7]學者使用肘關節后方尺骨鷹嘴截骨入路治療了8例肘關節“恐怖三聯征”患者,該手術入路擴大了手術視野,減少了對正常組織的進一步損傷,可完成尺骨冠狀突骨折、橈骨小頭骨折及肘關節內外側軟組織的修復。
尺骨冠突是尺骨近端干骺部向前方的延伸部分,具有維持肘關節軸向穩定,后內側、后外側旋轉穩定及防止肘內翻的重要作用,是維持肘關節前方穩定性最主要的骨性阻擋結構,也是防止肘關節后脫位、后外側半脫位的第一位因素[8]。冠突骨折主要的手術固定方法有套索縫合技術、微型螺釘、微型鋼板、錨釘等,具體的治療方案要根據骨折塊的大小、骨折類型及醫師的偏好來決定。Garrigues等[9]發現在冠突骨折中,經骨套索縫合固定技術優于螺釘或錨釘固定,其治療效果佳且并發癥少。Jeon等[10]尸檢發現在橈骨頭及韌帶完整的情況下(尤其是橈骨頭)冠突缺少40%(Ⅱ型骨折)不會發生肘關節不穩定,認為Ⅱ型冠突骨折屬于穩定性骨折。最近, Papatheodorou等[11]治療了12例冠突Ⅰ型和Ⅱ型的肘關節“恐怖三聯征”患者,所有患者給予肱尺關節復位,橈骨頭的修復或假體置換,修復外側副韌帶,但冠突及前側關節囊未予修復處理,術中所有病例獲得穩定,未修復內側副韌帶及使用外固定架,術后患者患肢結構及功能恢復良好。此外,Alolabi等[12]在缺少40%的冠突骨折的尸體模型中,發現同側尺骨鷹嘴尖部取骨植骨是重建冠突恢復正常運動力學的有效的方法,雖然這項技術僅適用于單純性冠突骨折,且還處于研究階段,但論證了冠突骨折缺損導致肘關節的不穩定。毫無疑問,冠突在肘關節穩定性中發揮關鍵性作用,我們建議對冠突骨折給予積極的內固定治療,尤其是骨折塊較大的Ⅱ型、Ⅲ型骨折(Regan-Morrey),而有些可能引起肘關節不穩定的Ⅰ型骨折也應該給予有效的內固定治療。
橈骨頭具有維持肘關節軸向及內外翻穩定的作用,在MCL損傷情況下其抗外翻作用尤為重要,在運動中可通過拉緊LCL間接提供抗內翻阻力。在肘關節“恐怖三聯征”中,橈骨頭骨折可使用鋼板固定或橈骨頭置換進行治療。使用鋼板固定骨折塊時,需注意鋼板應放置在“安全區”-橈骨頭的非關節面,以防術后影響前臂的旋轉功能[13]。橈骨頭置換在橈骨頭骨折中(尤其是在存在復雜類型的肘關節損傷中如:肘關節“恐怖三聯征”)的應用一直是研究的熱點。Watters等[14]發現在肘關節“恐怖三聯征”中,與切開復位內固定病例組相比,橈骨頭置換病例組患者的術中、術后及短期隨訪中肘關節的穩定性優于內固定治療組,但橈骨頭置換組的術后關節炎發生率高于內固定組。Ring 等也推薦肘關節“恐怖三聯征”患者采用橈骨頭置換治療。此外,Acevedo等[3]認為當尺骨冠突骨折<50%時,肘關節“恐怖三聯征”可以通過單純的橈骨頭關節置換和外側尺骨副韌帶修復手術進行治療。也有學者認為Mason Ⅲ型的橈骨頭骨折是無法重建的。因此,可對其進行橈骨頭切除加橈骨頭置換[15]。盡管橈骨頭置換在材料、類型及技術方面都得到了快速的發展,但橈骨頭置換之后帶來的并發癥及遠期療效仍然困擾著眾多學者,其中假體松動作為橈骨頭置換的一個遠期并發癥,是令眾多學者擔憂的問題,尤其是青年患者[13]。在我們的病例治療組中,大多數橈骨頭骨折能夠通過內固定獲得治療,橈骨頭置換不僅增加了患者的經濟負擔,而且遠期療效不明。因此,我們不主張進行橈骨頭置換。
外側副韌帶是抗內翻應力的主要穩定結構,有利于支撐橈骨頭、防止肘關節發生半脫位。在肘關節“恐怖三聯征”中外側副韌帶復合體,通常自肱骨遠端的起點處發生撕脫,可用不可吸收縫線或以帶線“錨釘”縫合固定在肱骨遠端,此時檢查肘關節的穩定性,肘關節由伸直位到屈曲位,如果屈曲未達30°~40°時即發生脫位,可以運用同樣的方法修復損傷的內側副韌帶[16]。 一直以來對于“恐怖三聯征”中肘關節內側副韌帶損傷的處理存在著爭議,有學者認為在治療后殘存不穩定的患者可給予修復內側副韌帶,也有學者認為修補內側韌帶結構是手術程序中的重要環節一,仲飆等[17]認為術前應通過MRI檢查予充分評估肘關節內側軟組織損傷情況,對于前束輕度撕裂而完整性存在者無需處理,但對于嚴重的起、止點撕脫或體部斷裂者,應常規采用內側入路探查修補。外側副韌帶是維持肘關節穩定性的重要結構之一,可能是肘關節脫位時是第一個被破壞的結構[1],因此我們應對所有的外側副韌帶給予積極有效的修復治療,同時也應重視內側副韌帶的損傷情況,做出恰當的處理。
隨著人們對肘關節“恐怖三聯征”認識的加深及內固定技術的發展,鉸鏈式外固定架的運用相對減少,但有限內固定結合鉸鏈支架治療肘關節“恐怖三聯征”既能保持肘關節的穩定性,又能早期進行功能鍛煉,減少并發癥的發生[18]。
總之, 肘關節“恐怖三聯征”通過積極有效的手術治療,大多數患者能夠得到滿意的結果。對于該類損傷,我們應盡可能通過有效的內固定重建骨及韌帶的穩定結構,恢復肘關節的穩定性,及早配合正規的功能鍛煉,最大程度恢復肘關節的功能。
[2] Butler DP, Alsousou J, Keys R. Isolated anterolateral fracture of the coronoid process of the ulna: a case report[J]. J Shoulder Elbow Surg, 2011, 20(2): e1-e4.
[3] Acevedo DC, Paxton ES, Kukelyansky I, et al. Radial head arthroplasty: state of the art[J]. J Am Acad Orthop Surg, 2014, 22(10): 633-642.
[4] Hotchkiss RN. Fractures and dislocations of the elbow//Rockwood CA Jr, Green DP, Bucholz RW, et al. Rockwood and Green′s Fractures in Adults[M].4th ed. Philadelphia, PA: Lippincott-Raven, 199:929-1024.
[5] Pugh DM, Wild LM, Schemitsch EH, et al. Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures[J]. J Bone Joint Surg Am, 2004, 86-A(6): 1122-1130.
[6] Zeiders GJ, Patel MK. Management of unstable elbows following complex fracture-dislocations—the terrible triad′ injury[J]. J Bone Joint Surg Am, 2008,90(Suppl 4):75-84.
[7] 林國葉,劉航濤,黃玉棟,等.肘關節后方+尺骨鷹嘴截骨入路治療肘關節恐怖三聯癥[J].中國傷殘醫學,2014,22(2):58-60.
[8] Manidakis N, Sperelakis I, Hackney R, et al. Fractures of the ulnar coronoid process[J]. Injury, 2012, 43(7): 989-998.
[9] Garrigues GE, Wray WH, Lindenhovius AL, et al. Fixation of the coronoid process in elbow fracture-dislocations[J]. J Bone Joint Surg Am, 2011, 93(20): 1873-1881.
[10] Jeon IH, Sanchez-Sotelo J, Zhao K, et al. The contribution of the coronoid and radial head to the stability of the elbow[J]. J Bone Joint Surg Br, 2012, 94(1): 86-92.
[11] Papatheodorou LK, Rubright JH, Heim KA,et al.Terrible triad injuries of the elbow: does the coronoid always need to be fixed? [J].Clin Orthop Relat Res,2014 ,472(7):2084-2091.
[12] Alolabi B, Gray A, Ferreira LM, et al. Reconstruction of the coronoid process using the tip of the ipsilateral olecranon[J]. J Bone Joint Surg Am, 2014, 96(7): 590-596.
[13] Bohn K, Ipaktchi K, Livermore M, et al. Current treatment concepts for"terrible triad. injuries of the elbow[J].Orthopedics, 2014, 37(12): 831-837.
[14] Watters TS, Garrigues GE, Ring D, et al. Fixation versus replacement of radial head in terrible triad: is there a difference in elbow stability and prognosis?[J]. Clin Orthop Relat Res, 2014, 472(7): 2128-2135.
[15] El Sallakh S. Radial head replacement for radial head fractures[J]. J Orthop Trauma, 2013, 27(6): e137-e140.
[16] 陳輝,郭慶山,劉華渝,等. 肘關節“恐怖三聯征”的診斷和治療[J].創傷外科雜志,2014,16(3):222-225.
[17] 仲飆,張弛,羅從風,等.肘關節“恐怖三聯征”中內側副韌帶及合并損傷的治療策略[J].中華骨科雜志,2013, 33(5):534-540.
[18] 溫曉東,李玉茂,張玉九.有限內固定結合鉸鏈式外固定架治療肘關節[J].疑難病雜志,2013,(8):627-629.
(本文編輯:胡桂英)
孟亞軻,劉巖,葉添文,等.肘關節“恐怖三聯征”的手術治療:附14例報告[J/CD]. 中華肩肘外科電子雜志,2015,3(3):151-155.
Operative treatment of elbow joint "terrible triad":attached with report on 14 cases
MengYake,LiuYan,YeTianwen,OuyangYueping,ChenAimin,GuoYongfei.
DepartmentofOrthopaedics,theSecondMilitaryUniversityAffiliatedChangzhengHospital,Shanghai200003,China
GuoYongfei,Email:cz-gyf@163.com
Background Elbow joint "terrible triad" refers to posterior dislocation of elbow joint combined with ulna coracoid process fracture and radius head fracture, often accompanied with injuries of medial collateral ligament and/or lateral collateral ligament of elbow joint. Distal clavicular fracture combined with coracoclavicular ligament rupture frequently behave as unstable fracture, with the opportunity for fracture non-union in conservative therapy being as high as 21%. During the period from July 2010 to October 2013, our department performed operative treatment for 14 cases of elbow joint "terrible triad" with complete follow-up, and achieved satisfactory therapeutic effects. The specific process is hereby reported as follows.Method I. General materials:This group includes 14 cases (11 male cases and 3 female cases), aged 23-48 years, with an average age of 35.4 years; 5 cases in the left side, 9 cases in the right side, all suffer from closed injury. No one case suffers from related neurovascular injury. Injury causes: High falling accident 5 cases, traffic accident 3 cases, falling injury 4 cases and sport injury 2 cases. After hospital admission, according to the routine procedure, we performed elbow joint X-ray anterioposterior and lateral film, elbow joint CT scanning and three-dimensional reconstruction to judge the type of fracture and the fracture displacement condition. Ulna coronoid fracture Regan-Morrey typing , 10 cases of type Ⅲ, and 2 cases of type Ⅲ; According to Mason typing of radius head fracture, 7 cases of type Ⅲ, and 3 cases of type Ⅲ, of which 1 case is combined with ipsilateral distal radius fracture,And 1 case is combined with ipsilateral ulnar fracture; All the cases in this group are combined with injuries of medial collateral ligament and/or lateral collateral ligament of elbow joint.Ⅱ. Operative method:Allow the patient to lie flat on operating table, and place inflatable tourniquets on the proximal ends of affected limbs. Under brachial plexus block anesthesia, conventionally use elbow joint medial and lateral combined approaches, perform reduction of affected elbow joint, then in the sequence from the shallower to the deeper repair the ulna coracoid process fracture, the anterior joint capsule, the radius head fracture, the lateral collateral ligament and the starting point of common extensor tendon. The ulna coracoid process fracture is fixed by using mini-plate, lag screw, stitching anchor or rope stitching technique; radial head fracture is fixed by using kirschner wire, mini-screw and mini-plate; For all the cases, we use non-absorbable braided suture or anchor to repair their lateral collateral ligaments (LCL). Prior to incision closure, perform varus-valgus rotation test on straight position of elbow joint and cubitus valgus overload test to judge the recovery of elbow joint stability. In the process of passive flexion of elbow joint, 3 cases show poor concentric circle stability, for 2 cases of them, we use non-absorbable braided suture and anchor to repair their medial collateral ligaments (MCL); For 1 case, place lateral articulated type external fixation support, and keep elbow joint flexion 90°fixed hinge during operation; the other 12 cases can still maintain stability. After operation, 13 cases are provided with elbow joint flexion 90°and plaster fixation at neutral position of fore arms.Ⅲ. Functional exercise and follow-up:13 cases in plaster fixation perform finger movement as well as Biceps brachii muscle/Triceps brachii muscle isometric contraction training; At postoperative 48h, start passive elbow joint flexion and extension activity as well as fore arm rotation activity. At operative 1-2 week, 1 case assisted with external fixation started functional exercise; in the 1st week post operation, adjust the knob at the center of hinge support, instruct the affected elbows to perform flexion and extension function exercise; At post-operative 6th-8thweek, remove external fixation support. In the process of rehabilitation, avoid hyperextension of elbow joint. After operation, respectively in the follow-up on the 1stday, at the 2ndweek, 1stmonth, 3rdmonth, 6thmonth and 12thmonth, take X-ray anterioposterior and lateral film of affected elbow joints. Observe the healing condition of fracture fragments as well a s the occurrence of postoperative complications such as heterotopic ossification and Osteoarthritis; Investigate the improvements in elbow joint function, and instruct the patients to perform functional exercise. Upon completion of follow-up, perform evaluation of therapeutic effect according to Mayo elbow joint function scoring standard.Results 14 cases in this group obtained follow-up, with an average follow-up time of 18 months (10-37 months). The clinical fracture union time is postoperative 10-15 weeks, with an average time of 12.4 weeks. In postoperative 6 months, elbow joint flexion position (0°-20°), extension position (130°-145 °), with an average range of joint motion being 116.5°; pronation (60°-85°)supination (45°-75°), with an average rotation range of 126°. 1 case has stiff elbow joint; 2 cases show heterotopic ossification in imageological examination at the 6thmonth after operation, which, however do not affect the functions of elbow joint. Evaluation according to Mayo scoring standard: Excellent 6 case, good 4 cases, general 2 cases and poor 1 case.Conclusion Through active and effective operative treatment for elbow joint "terrible triad", most of the patients can obtain satisfactory results. For such type of injuries, we should make every effort to reconstruct stable structure of bone and ligament through effective internal fixation and recover the stability of elbow joint in combination with timely and normal functional exercise, so as to recover the functions of elbow joint to the maximum extent.
Elbow joint;Terrible triad;Fracture;Dislocation;Fixation
10.3877/cma.j.issn.2095-5790.2015.03.005
國家自然基金青年項目(31100988)
200003上海,第二軍醫大學附屬長征醫院骨科
郭永飛,Email:cz-gyf@163.com
2015-01-01)
猜你喜歡
中華詩詞(2022年6期)2022-12-31 06:41:24
昆明醫科大學學報(2021年2期)2021-03-29 07:42:46
河北畫報(2020年10期)2020-11-26 07:20:50
中國科技論壇(2017年7期)2017-07-25 08:49:53
媽媽寶寶(2017年2期)2017-02-21 01:21:24
國際漢語學報(2016年1期)2017-01-20 08:21:20
中國衛生標準管理(2015年3期)2016-01-14 03:41:47
西南軍醫(2014年5期)2014-04-25 07:42:48
中國中醫藥現代遠程教育(2014年22期)2014-03-01 04:32:55
中國中醫藥現代遠程教育(2014年16期)2014-03-01 04:28:54