Observation on therapeutic effects of acupuncture plus Chinese herbs for sudden deafness
2015-05-18 09:01:35WangHuanren王環仁MengFanrui孟凡銳ChiXiaowei遲曉偉DingJian丁見
關鍵詞:針刺
Wang Huan-ren (王環仁), Meng Fan-rui (孟凡銳), Chi Xiao-wei (遲曉偉), Ding Jian (丁見)
Traditional Chinese Medicine Hospital of Huangdao District, Qingdao, Shandong 266000, China
Observation on therapeutic effects of acupuncture plus Chinese herbs for sudden deafness
Wang Huan-ren (王環仁), Meng Fan-rui (孟凡銳), Chi Xiao-wei (遲曉偉), Ding Jian (丁見)
Traditional Chinese Medicine Hospital of Huangdao District, Qingdao, Shandong 266000, China
Objective:To observe the clinical effect of wind-expelling method of acupuncture and Chinese herbs for sudden deafness.Methods:A total of 90 cases with sudden deafness were randomly divided into three groups based upon their visit order and random digital table, an acupuncture plus Chinese herbs (APCH) group, an acupuncture group, and a Western medication (WM) group, 30 cases in each group. The APCH group was treated by puncturing Fengchi (GB 20), Fengfu (GV 16) and Fengmen (BL 12), without retaining the needles, and then by puncturing Zhongwan (CV 12), Guanyuan (CV 4), Qihai (CV 6) and Tianshu (ST 25) with reinforcing technique after arrival of the needling sensation, and the needles were retained for 30 min, plus oral administration of wind-expelling Chinese herbs. The acupuncture group was treated with the acupoints selected by syndrome differentiation in reference to the textbook of Acupuncture and Moxibustion Science. The WM group was treated by intravenous infusion of Alprostadil injection, Adenosine Disodium Triphosphate and Coenzyme A and muscular injection of Vitamin B12and Vitamin B1. The decibel values of hearing loss before and after treatment were respectively recorded and analyzed comparatively.
Acupuncture Therapy; Acupuncture Medication Combined; Drugs, Chinese Herbal; Hearing Loss, Sudden; Deafness
Sudden deafness refers to sudden onset of unexplained hearing loss. The hearing loss is characterized by sensorineural deafness. The patient’s hearing ability can decline to the lowest point within minutes, hours or days, simultaneously accompanied by tinnitus, obstructive sensation in the ear, dizziness, nausea and vomiting, seriously influencing the patient’s life, work and study. We started to treat sudden deafness by wind-expelling method in the Acupuncture Department and ENT Department of our hospital from 2008. In order to enhance the therapeutic effects and further promote standard operation, we conducted the clinical study on treatment of sudden deafness by wind-expelling method of acupuncture and Chineseherbs. Now, the report on the research findings is given as follows.
1 Clinical Materials
1.1 Diagnostic criteria
The diagnostic criteria in this study were stipulated based upon theClinical Diagnostic and Therapeutic Guidelines: Volume of Otolaryngology, Head and Neck Surgery[1]and theDiagnostic and Therapeutic Guidelines for Sudden Deafness[2]: sudden occurrence within minutes, hours or over a period of up to three days, non-fluctuant sensorineural hearing loss, that can be mild, moderate or severe, even complete deafness, mostly affects only one ear, occasionally affects both ears at the same time or in succession, with unknown factors (without any precise general or local factor), accompanied by dizziness, nausea, and vomiting in infrequent attackts. Except the eighth cranial nerve, there was no any symptom of cranial nerve lesion.
1.2 Inclusion criteria
In conformity with the above diagnostic criteria; both genders; with the age between 10 and 80 years old; clear consciousness, stable vital signs; hearing loss above 26 dB; signed the informed consent.
1.3 Exclusion criteria
Those not in conformity with the above diagnostic criteria; those with the hearing loss less than 26 dB; those complicated with primary cardiac, cerebral and renal diseases seriously endangering the life; those with mental disorders; and those unable to follow the therapeutic plan due to various reasons.
1.4 Statistical method
The SPSS 13.0 version statistical software was used for statistical management. The measurement data were expressed by mean ± standard deviationandt-test was used for same group before and after treatment, variance analysis was used for a betweengroup comparison. The enumeration data were processed by Chi-square test.P<0.05 indicates the statistically significant difference.
1.5 General data
Totally, 90 cases were the outpatients or inpatients from the Acupuncture Department and ENT Department of Traditional Chinese Medicine Hospital of Huangdao District, Qingdao, between January 2011 and December 2012. They were randomly divided into three groups based upon their visit order and the random digital table: an acupuncture plus Chinese herbs (APCH) group, an acupuncture group, and a Western medication (WM) group, 30 cases in each group. In analysis of the general data of the three groups, the differences were not statistically significant (allP>0.05), indicating that the three groups were comparable (Table 1).

Table 1. Comparison of general data among the three groups
2 Treatment Methods
2.1 APCH group
2.1.1 Acupuncture treatment
Acupoints: Fengchi (GB 20), Fengfu (GV 16), Fengmen (BL 12), Zhongwan (CV 12), Guanyuan (CV 4), Qihai (CV 6) and Tianshu (ST 25).
Method: The disposable sterile acupuncture needles of 0.30 mm in diameter and 40 mm in length were selected. Fengchi (GB 20), Fengfu (GV 16) and Fengmen (BL 12) were punctured quickly by 25 mm. After arrival of the needling sensation, the needles were taken out immediately. Zhongwan (CV 12), Guanyuan (CV 4), Qihai (CV 6) and Tianshu (ST 25) were punctured by about 30 mm. After arrival of the needling sensation, the needles were manipulated by reinforcing technique. The needles were retained for 30 min and manipulated once every 10 min. The treatment was given once every day. The therapeutic effects were observed after 15 treatments.
2.1.2 Chinese herbs
Composition:Fang Feng(Radix Ledebouriellae) 9 g,Chan Tui(Periostracum Cicadae) 9 g,Fu Ling(Poria) 9 g,Gan Cao(Radix Glycyrrhizae) 6 g,Huang Qin(Radix Scutellariae) 9 g,Bai Shao(Radix Paeoniae Albae) 9 g,Zhi Shou Wu(Radix Polygoni Multiflori) 20 g,Ju Hong(Exocarpium Citri Grandis) 9 g,Gua Lou(Fructus Trichosanthis) 9 g,Ban Xia(Rhizoma Pinelliae) 9 g,Yu Jin(Radix Curcumae) 9 g,Long Gu(Os Draconis) 12 g,Mu Li(Concha Ostreae) 12 g,Bei Sha Shen(Radix Glehniae) 12 g,Shi Chang Pu(Rhizoma Acori Graminei) 9 g,Cao Dou Kou(Semen Alpiniae Katsumadai) 6 g. The herbal decoction was taken orally warm for one dose per day. The therapeutic effects were observed after oral administration for 15 d.
2.2 Acupuncture group
Main acupoints: Tinghui (GB 2), Yifeng (TE 17), Xiaxi (GB 43) and Zhongzhu (TE 3) selected based upon the textbook ofAcupuncture and Moxibustion Science[3].
Adjuvant acupoints: Waiguan (TE 5), Hegu (LI 4), Quchi (LI 11) and Dazhui (GV 14) were added for invasion of wind and heat; Taichong (LR 3) and Qiuxu (GB 40) for upward disturbance of the liver fire; Fenglong (ST 40) and Dazhui (GV 14) for accumulation of phlegm and fire; Geshu (BL 17) and Xuehai (SP 10) for qi stagnation and blood stasis; Shenshu (BL 23) andGuanyuan (CV 4) for deficiency of kidney essence; and Zusanli (ST 36), Qihai (CV 6) and Pishu (BL 20) for deficiency of qi and blood.
Method: The same acupuncture needles as those in the APCH group were used. All the acupoints were punctured by about 25 mm. After arrival of the needling sensation, the reducing manipulation was applied for excess pattern, and the reinforcing manipulation was applied for deficient pattern. The needles were retained for 30 min and manipulated once every 10 min. The treatment was given once every day. The therapeutic effects were observed after acupuncture treatment for 15 d.
2.3 WM group
Alprostadil injection (Beijing Tide Pharmaceutical Co., Ltd., China) 2 mL, Adenosine Disodium Triphosphate for injection (Beijing Shuanglu Pharmaceutical Co., Ltd., China) 40 mg, and Coenzyme A for injection (Tianjin Pharmaceutical Jiaozuo Co., Ltd., China) 100 U were used for intravenous infusion after dissolved with 500 mL 5% glucose injection. Vitamin B12injection (Shanxi Hengda Pharmaceutical Co., Ltd., China) 500 ug, and Vitamin B1injection (Huangshan Tianmu Pharmaceutical Co., Ltd., China) 100 mg were used for muscular injection. The intravenous infusion and muscular injection were given once every day. The therapeutic effects were observed after the treatment for 15 d.
3 Observation of Therapeutic Effects
3.1 Criteria of therapeutic effects
The criteria of the therapeutic effects were stipulated based upon theGuideline of Diagnosis and Treatment of Sudden Deafness(2005, Jinan)[2].
Cure: The auditory threshold of damaged frequency was restored to the normal level, or to the level of the healthy ear or to the level before this sickness.
Remarkable effect: The average hearing ability of the damaged frequency was elevated by over 30 dB.
Effect: The average hearing ability of the damaged frequency was elevated by 15-30 dB.
Failure: The average hearing ability of the damaged frequency was improved by less than 15 dB.
建筑幕墻是一件舶來品,是在80年代初伴隨著改革開放的步伐進入中國建筑市場的[1]。早期的國內幕墻市場主要由外國公司承包,但隨著中國的改革開放,經濟的快速發展,建筑市場的爆炸性擴展,國內的建筑幕墻企業也從無到有,在幕墻設計、施工技術、產品質量、新產品、新技術等方面獲得了空前的發展。從90年代開始,國內幕墻企業就有了走出國門,參與國際競爭的實力。筆者所在的企業,80年代就開始在中東和非洲的一些國家承接幕墻和鋁合金門窗工程。隨著世界經濟的逐步復蘇和國家“一路一帶”政策的影響,現在走出去的企業越來越多。
3.2 Therapeutic results
3.2.1 Comparison of the decibel value of hearing loss among the three groups
Before treatment, by the statistical management of the decibel value of hearing loss among the three groups, the differences were not statistical significant (P>0.05). After treatment, the decibel value of hearing loss all declined in the three groups and the differences within the group before and after treatment were statistically significant (P<0.05), indicating that the methods in the three groups could improve the hearing ability. In the between-group comparisons after treatment, the APCH group was statistically different from the acupuncture group and the WM group (bothP<0.05), and the acupuncture group and the WM group were not statistically different (P>0.05), indicating that the hearing ability was improved better in the APCH group than in the other two groups (Table 2).
Table 2. Comparison of the decibel value of hearing loss before and after the treatment among the three groups
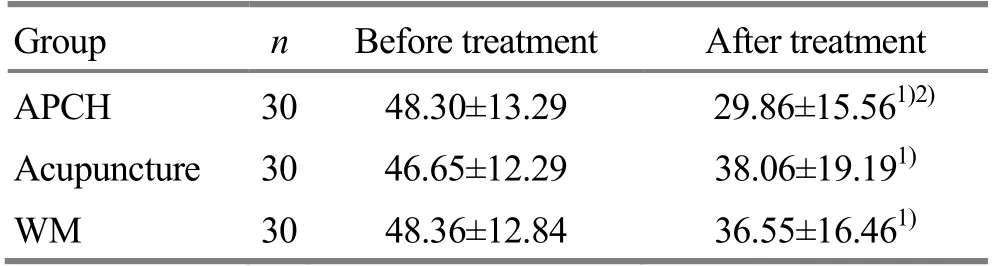
Table 2. Comparison of the decibel value of hearing loss before and after the treatment among the three groups
Note: Compared with the same group before treatment, 1) P<0.05; compared with the acupuncture group and the WM group, 2) P<0.05
Group n Before treatment After treatment APCH 30 48.30±13.29 29.86±15.561)2)Acupuncture 30 46.65±12.29 38.06±19.191)WM 30 48.36±12.84 36.55±16.461)
3.2.2 Comparison of therapeutic effects among the three groups
The total effective rate was 83.3% in the APCH group, 60.0% in the acupuncture group and 56.7% in the WM group. The total effective rate was higher in the APCH group than those in the other two groups (P<0.05), (Table 3).

Table 3. Comparison of clinical effects among three groups (case)
4 Discussion
Sudden deafness belongs to the scope of deafness in Chinese medicine and is a sudden unexpained hearing loss. It is believed in Chinese medicine that the ear is a site to communicate with the clear yang, it belongs to one of the clear orifices. Wind is a yang pathogenic factor, characterized by upward flowing and putward dispersion[4-5]. Wind easily blocks the clear orifice, leading to deafness frequently. Therefore, we treatsudden deafness clinically by expelling wind in our clinic.
Fengfu (GV 16) is located in the midline of the occipital region. Physiologically, it is like an imperial court to govern wind acupoints[6]. Pathologically, it is a site where pathogenic wind invades. Fengmen (BL 12) corresponds to the lung internally and is a path of respiration. Fengchi (GB 20) is a pass for pathogenic wind to enter the brain and is a site where pathogenic wind gathers. Therefore, Fengfu (GV 16), Fengmen (BL 12) and Fengchi (GB 20) are punctured to expel pathogenic wind and regulate the skin striations[7]. Zhongwan (CV 12) is the Front-Mu point of the stomach and an Influential acupoint of Fu organs. Guanyuan (CV 4) is located in a confluence site of primordial yin and yang and is the sea of Yuan-primordial qi. Qihai (CV 6) is a Yuan-Primary acupoint of the region between the heart and diaphragm, a site where Yuan-primordial qi gathers. Moreover, this acupoint also used to dredge all the meridians of the whole body, so that blood can flow through, once qi reaches. Tianshu (ST 25) is located in the juncture of the upper abdomen and lower abdomen, exactly in the middle of the human body, and is able to communicate with the middle jiao, mediate with the upper abdomen and lower abdomen, and govern the ascending and descending effect and is an axis for qi transformation, outflow and inflow of the three jiao. Therefore, Zhongwan (CV 12), Guanyuan (CV 4), Qihai (CV 6) and Tianshu (ST 25) are punctured to replenish qi, supplement the resource and regulate qi dynamic[8]. All the acupoints are used together to dissipate the external wind and eliminate the internal wind, combined by Chinese herbs of Fang Feng (Radix Ledebouriellae) and Chan Tui (Periostracum Cicadae) to expel wind and disperse pathogens, Fu Ling (Poria) and Gan Cao (Radix Glycyrrhizae) to strengthen the spleen and harmonize the center, Huang Qin (Radix Scutellariae), Bai Shao (Radix Paeoniae Albae), and Zhi Shou Wu (Radix Polygoni Multiflori) to balance and soothe the liver, Bei Sha Shen (Radix Glehniae), Ju Hong (Exocarpium Citri Grandis), Gua Lou (Fructus Trichosanthis), Yu Jin (Radix Curcumae) and Ban Xia (Rhizoma Pinelliae) to clarify the lung, regulate qi, dilate the chest and correct the reversely-flowing qi, and Cao Dou Kou (Semen Alpiniae Katsumadai) and Shi Chang Pu (Rhizoma Acori Graminei) to warm the middle jiao and dissolve phlegm and communicate with yin and yang, and Long Gu (Os Draconis) and Mu Li (Concha Ostreae) to reduce fire and suppress yang, hold back the spirit and extinguish the internal wind[9].
It has been proven by this study that the total effective rate is 83.3% in the APCH group, better than those in the WM group and the acupuncture group. Moreover, this therapy is applied by quick insertion and abdominal acupoints, thus producing less pain[13], but faster in operation and better in therapeutic effect[14]. Therefore, it needs promoting clinic[15].
Conflict of Interest
The authors declared that there was no conflict of interest in this article.
Acknowledgments
This work was supported by Traditional Chinese Medicine Scientific Research Project of Qingdao Health Bureau, Shandong Province (山東省青島市衛生局中醫科研計劃課題, No.2012-zyw018).
Statement of Informed Consent
Informed consent was obtained from all individual participants included in this study.
Received: 5 January 2015/Accepted: 8 February 2015
[1] Chinese Medical Association. Clinical Diagnostic and Therapeutic Guidelines: Volume of Otolaryngology, Head and Neck Surgery. Beijing: People’s Medical Publishing House, 2009: 410-411.
[2] Chinese Otorhinolaryngology Head and Neck Surgery Society of Chinese Medical Association, Editorial Board of Chinese Journal of Otorhinolaryngology Head and Neck Surgery. Guideline of diagnosis and treatment of sudden deafness (2005, Jinan). Zhonghua Er Bi Yanhou Tou Jing Waike Zazhi, 2006, 41(8): 569.
[3] Sun GJ. Acupuncture and Moxibustion Science. Shanghai: Shanghai Science and Technology Publishers, 1997: 306-307.
[4] Tian DH, Liu GS. Ling Shu (Spiritual Pivot). Beijing: People’s Medical Publishing House, 2007: 71.
[5] Huang Di Nei Jing Su Wen (Essential Questions of Yellow Emperor’s Classic of Internal Medicine). Beijing: People’s Medical Publishing House, 2012: 122.
[6] Zhang CX. Collective Annotation to Meanings of Acupoints. Shanghai: Shanghai Translation Publishing Company, 1984: 294.
[7] Yao YF. Exploration on pattern and treatment of wind acupoints. Zhongguo Zhen Jiu, 1999, 19(2): 41-43.
[8] Bo ZY. Abdominal Acupuncture. Beijing: China Science and Technology Publishers, 1999: 101.
[9] Lei ZQ. Chinese Materia Medica. Shanghai. Shanghai: Shanghai Science and Technology Publishers, 2000: 251.
[10] Tian DH. Huang Di Nei Jing Su Wen (Essential Questions of Yellow Emperor’s Classic of Internal Medicine). Beijing: People’s Medical Publishing House, 2013: 143.
[11] Wang XH. Basic Theory of Chinese Medicine. Beijing: People’s Medical Publishing House, 2001: 187.
[12] Li DY. Treatise on the Spleen and Stomach. Beijing: China Science and Technology Publishers, 2013: 22.
[13]Wang LP. Clinical experience on Bo's abdominal acupuncture. Zhongguo Zhen Jiu, 2004, 24(3): 201-202.
[14]Zhou ZT, Lin XS, Zhou MQ. Treatment of 42 cases of sudden deafness by abdominal acupuncture. Zhongguo Zhen Jiu, 2006, 26(4): 303.
[15]Ma YZ, Zeng W, Feng ZQ, Huang GQ, Chen MZ. Factors associated with sudden sensorineural hearing loss of the in-patients between 2001 and 2011. Tinglixue Ji Yanyu Jibing Zazhi, 2012, 20(4): 330-332.
Translator:Huang Guo-qi (黃國琪)
針藥并用治療突發性耳聾療效觀察
目的:觀察祛風法針藥并用治療突發性耳聾的臨床療效。方法:將90例突發性耳聾患者按照就診先后順序, 查隨機數字表后根據隨機號分成3組, 針藥并用組、針刺組和西藥組, 每組30例。針藥并用組速刺風池、風府、風門, 不留針; 然后針刺中脘、關元、氣海、天樞, 得氣后用補法, 留針30 min。同時口服祛風中藥。針刺組參照《針灸學》教材予以辨證取穴針刺治療。西藥組靜滴前列地爾注射液、注射用三磷酸腺苷二鈉和注射用輔酶A; 肌注維生素B12和維生素B1注射液。分別記錄3組患者治療前后的聽力損失分貝值, 并進行比較分析。結果:三組治療后與同組治療前比較, 聽力損失分貝值均有下降, 差異均有統計學意義(均P<0.05); 治療后, 三組聽力損失分貝值比較, 針藥并用組優于針刺組(P<0.05)和西藥組(P<0.05)。針藥并用組總有效率為 83.3%, 針刺組總有效率為60.0%, 西藥組總有效率為56.7%; 針藥并用組總有效率高于其他兩組(均P<0.05)。結論:祛風法針藥并用治療突發性耳聾的療效優于西藥組和針刺組。
針刺療法; 針藥并用; 中草藥; 聽覺喪失, 突發; 聾
R246.8 【
】A
Author: Wang Huan-ren, bachelor, deputy physician, associate professor.
E-mail: fanrym@126.com
Results:In the intra-group comparison after treatment among the three groups, the decibel values of hearing loss all declined, with statistically significant differences (allP<0.05). After treatment, the decibel value of hearing loss in the APCH group was better than those in the acupuncture group (P<0.05) and the WM group (P<0.05). The total effective rate was respectively 83.3% in the APCH group, 60.0% in the acupuncture group and 56.7% in the WM group. The total effective rate in the APCH group was better than those in other two groups (bothP<0.05).
Conclusion:The therapeutic effect was better for sudden deafness by wind-expelling method of acupuncture and Chinese herbs than by acupuncture alone or by Western medication.
猜你喜歡
中國民間療法(2021年19期)2021-11-20 06:23:00
中國民間療法(2021年18期)2021-11-02 08:20:38
中國民間療法(2021年5期)2021-06-09 09:21:36
中國民間療法(2021年4期)2021-06-09 09:20:18
中國民間療法(2021年1期)2021-04-20 02:30:34
基層中醫藥(2021年7期)2021-03-26 18:00:27
反射療法與康復醫學(2017年7期)2017-01-16 01:11:42
中醫研究(2014年8期)2014-03-11 20:29:23
中醫研究(2014年6期)2014-03-11 20:29:02
中國中醫藥現代遠程教育(2014年17期)2014-03-01 04:29:28
 Journal of Acupuncture and Tuina Science2015年4期
Journal of Acupuncture and Tuina Science2015年4期
- Journal of Acupuncture and Tuina Science的其它文章
- Clinical observation on collateral-pricking and cupping therapy plus moxibustion for localized neurodermatitis
- Therapeutic observation of superficial needling for hemifacial spasm
- Clinical study on abdominal acupuncture for osteoporotic vertebral compression fracture
- Effect observation on heat-sensitive moxibustion for cervical spondylosis of vertebral artery type
- Clinical observation on acupuncture combined with tuina manipulation for thoracic facet joint disorder
- Observation on clinical effects of herbal cake-partitioned moxibustion for knee osteoarthritis