高爾基體蛋白73單獨(dú)及聯(lián)合甲胎蛋白檢測(cè)在肝細(xì)胞癌診斷中的價(jià)值
2014-06-07 10:00:52張進(jìn)銀胡萬發(fā)王健魏紅山
傳染病信息 2014年5期
張進(jìn)銀,胡萬發(fā),王健,魏紅山
·臨床研究·
高爾基體蛋白73單獨(dú)及聯(lián)合甲胎蛋白檢測(cè)在肝細(xì)胞癌診斷中的價(jià)值
張進(jìn)銀,胡萬發(fā),王健,魏紅山
目的探討血清高爾基體蛋白(Golgiprotein,GP)73單獨(dú)及聯(lián)合甲胎蛋白(AFP)檢測(cè)在肝細(xì)胞癌(hepatocellular carcinoma,HCC)診斷中的價(jià)值。方法選擇HCC、肝炎、非HCC的其他腫瘤患者和健康人群,分別以酶聯(lián)免疫吸附試驗(yàn)檢測(cè)GP73水平,電化學(xué)發(fā)光法檢測(cè)AFP水平。結(jié)果HCC組GP73水平為(231.2±92.3)ng/ml,明顯高于肝炎組、其他腫瘤組和健康對(duì)照組,差異有統(tǒng)計(jì)學(xué)意義(P<0.005)。GP73在81.08 ng/m l處獲得最大約登指數(shù),此時(shí)診斷HCC的靈敏度和特異度分別為86.2%和87.8%,高于AFP診斷的價(jià)值。GP73聯(lián)合AFP診斷HCC,可使診斷靈敏度進(jìn)一步提高至92.3%。結(jié)論GP73作為一種新型HCC血清標(biāo)記物在HCC診斷中有較高的靈敏度和特異度,且優(yōu)于AFP。GP73聯(lián)合AFP檢測(cè)可進(jìn)一步提高HCC診斷的靈敏度。
肝腫瘤;高爾基體蛋白73;酶聯(lián)免疫吸附測(cè)定;α-胎蛋白
肝細(xì)胞癌(hepatocellular carcinoma,HCC)是我國常見惡性腫瘤之一,每年死亡約11萬例,占全世界HCC死亡人數(shù)的45%[1]。由于多數(shù)HCC患者有肝炎及肝硬化等基礎(chǔ)性疾病,發(fā)病初期隱匿,臨床確診時(shí)多已發(fā)展至中晚期,治療效果差,5年生存期短。為此,在高危人群中建立監(jiān)測(cè)HCC的血清標(biāo)志物尤為重要。近年來高爾基體蛋白(Golgiprotein,GP)73被認(rèn)為在HCC診斷中具有較高的價(jià)值[2-3],為此我們選擇HCC患者,以血清GP73和甲胎蛋白(AFP)單獨(dú)或聯(lián)合檢測(cè),并進(jìn)行對(duì)比觀察,現(xiàn)報(bào)道如下。
1 對(duì)象與方法
1.1 對(duì)象HCC 65例(HCC組)為我院2012年12月—2013年5月的住院患者,經(jīng)查住院病歷及病理資料均為HCC術(shù)前標(biāo)本。178名(健康對(duì)照組)為2013年4月我院的體檢人群,均體格檢查正常、肝腎功能正常以及影像學(xué)檢查無異常。慢性乙型肝炎105例(慢乙肝組),為我院2013年4月的住院患者,其中HBe陽性50例,HBe陰性55例。非HCC的其他腫瘤患者49例(其他腫瘤組),為我院2013年4月的住院患者,其中乳腺癌8例,子宮惡性腫瘤6例,直腸癌5例,胃癌5例,胰腺癌5例,鼻咽癌3例,食管癌7例,肺癌5例,結(jié)腸癌5例。收集符合要求的血清標(biāo)本,置-70℃保存。肝炎及HCC診斷符合《病毒性肝炎防治方案》[4]。
1.2 方法對(duì)GP73和AFP聯(lián)合檢測(cè)進(jìn)行靈敏度和特異度分析,只要有1項(xiàng)為陽性即判定為聯(lián)合檢測(cè)陽性。應(yīng)用受試者工作特征曲線(receiver-operating characteristic curve,ROC曲線)分析GP73和AFP的診斷效能。
1.3 生化及GP73檢測(cè)用酶聯(lián)免疫吸附試驗(yàn)檢測(cè)血清GP73水平(試劑盒為北京熱景生物技術(shù)有限公司生產(chǎn)),嚴(yán)格按試劑盒說明書進(jìn)行操作。AFP用雅培i2000免疫發(fā)光分析儀及配套試劑進(jìn)行檢測(cè)。所有檢測(cè)均嚴(yán)格按標(biāo)準(zhǔn)實(shí)驗(yàn)室質(zhì)控方法進(jìn)行。
1.4 統(tǒng)計(jì)學(xué)處理用SPSS 15.0進(jìn)行統(tǒng)計(jì)分析。計(jì)量資料呈正態(tài)分布,用±s表示。多組間指標(biāo)差異性比較用單因素方差分析(組間方差齊),組內(nèi)各組與HCC組的多重比較用Dunnett-t檢驗(yàn)。GP73和AFP診斷HCC的診斷試驗(yàn)用ROC分析。P<0.05表示差異具有統(tǒng)計(jì)學(xué)意義。
2 結(jié)果
2.1 一般情況HCC組、慢乙肝組、其他腫瘤組和健康對(duì)照組的年齡和性別差異無統(tǒng)計(jì)學(xué)意義(表1)。
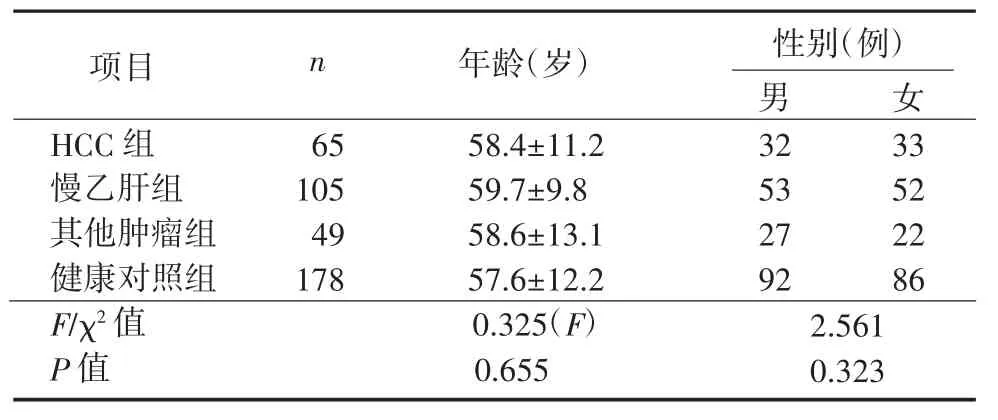
表1 各組一般情況Table 1 Basic characteristics of each group
2.2 各組血清GP73和AFP水平比較各組GP73和AFP水平檢測(cè)結(jié)果見表2。HCC組GP73和AFP水平明顯高于慢乙肝組、其他腫瘤組及健康對(duì)照組(P<0.01)。
表2 各組GP73和AFP水平比較(±s,ng/m l)Table 2 Comparison of GP73 and AFP levels among the groups(±s,ng/m l)
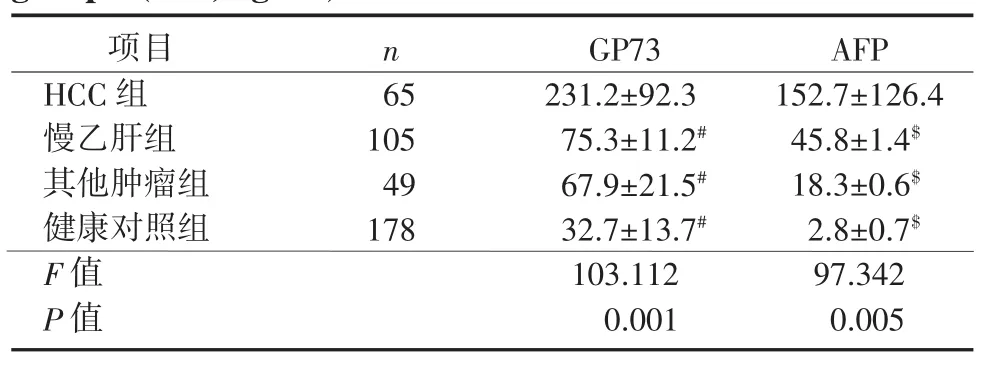
表2 各組GP73和AFP水平比較(±s,ng/m l)Table 2 Comparison of GP73 and AFP levels among the groups(±s,ng/m l)
注:#.與HCC組GP73水平與其他3組比較,P<0.01;$.與HCC組比較,P<0.01
項(xiàng)目HCC組慢乙肝組其他腫瘤組健康對(duì)照組F值P值n 65 105 49 178 GP73 231.2±92.3 75.3±11.2#67.9±21.5#32.7±13.7#103.112 0.001 AFP 152.7±126.4 45.8±1.4$18.3±0.6$2.8±0.7$97.342 0.005
2.3 ROC分析以病理結(jié)果為“金標(biāo)準(zhǔn)”,以1-特異度為橫坐標(biāo),以靈敏度為縱坐標(biāo)繪制ROC曲線。GP73在81.08 ng/ml處獲得最大約登指數(shù),此時(shí)GP73診斷HCC的靈敏度和特異度分別為86.2%和87.8%,線下面積為0.922。AFP在20.00 ng/ml處獲得最大約登指數(shù),此時(shí)診斷HCC的靈敏度和特異度分別為61.5%和89.0%,線下面積為0.801(線下面積比較χ2=4.841,P<0.05)。見圖1、表3。
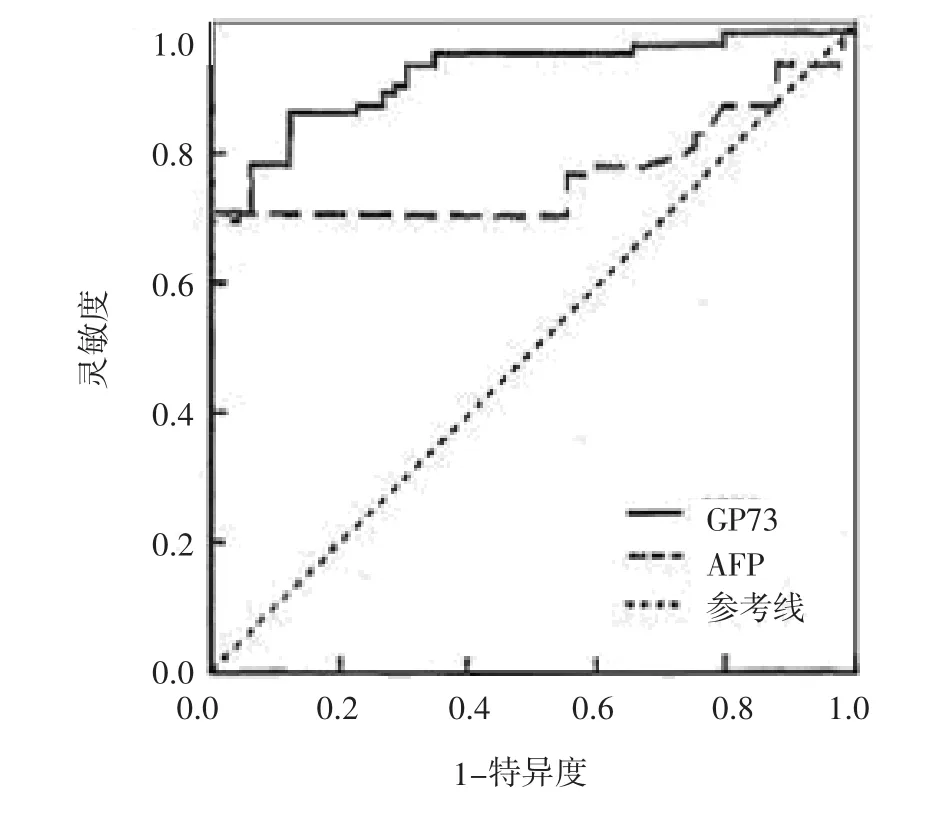
圖1 GP73和AFP水平診斷HCC的ROC曲線Figure 1 ROC curves of GP73 and AFP levels for the diagnosis of HCC

表3 GP73和AFP診斷HCC情況Table 3 Authentic assessment of GP73 and AFP levels in the diagnosis of HCC
2.4 GP73聯(lián)合AFP診斷HCC HCC組中GP73陽性48例,AFP陽性35例。GP73和AFP聯(lián)合檢測(cè)靈敏度提高到92.3%,而特異性保持在較高的水平,為83.1%(表4)。
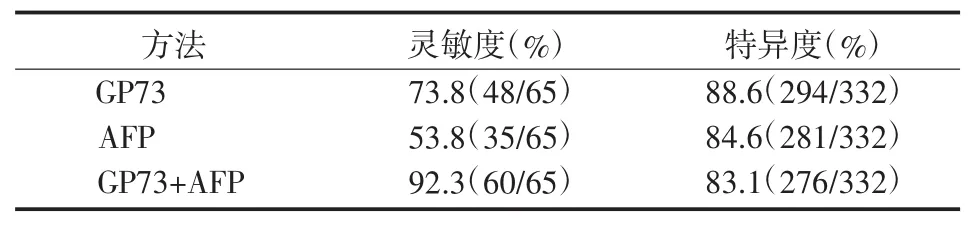
表4 GP73單獨(dú)及聯(lián)合AFP診斷HCC情況Table 4 Com parison of GP73 level alone and in combination w ith AFP level in the diagnosis of HCC
3 討論
HCC是我國常見的惡性腫瘤,年病死率約20.37/10萬,居惡性腫瘤死亡率的第2位,是亟待解決的公共衛(wèi)生難題[5]。AFP是目前全球應(yīng)用最為廣泛的HCC標(biāo)志物,具有較高的特異度和靈敏度[6-8]。但近年來發(fā)現(xiàn),部分HCC患者雖有較典型的臨床表現(xiàn)和影像學(xué)資料,但AFP水平卻低于診斷標(biāo)準(zhǔn),提示以AFP水平輔助診斷HCC仍有一定局限性。GP73是定位于高爾基體的一種Ⅱ型跨膜蛋白,主要由膽管上皮細(xì)胞表達(dá)[9],在肝細(xì)胞表達(dá)很少甚至不表達(dá)。
本研究提示HCC組血清GP73水平為(231.2± 92.3)ng/ml,較慢乙肝組、其他腫瘤組和健康對(duì)照組均明顯升高,進(jìn)一步分析30例AFP陰性患者,發(fā)現(xiàn)有18例(60%)GP73呈陽性,提示GP73用于HCC診斷具有較好的靈敏度和特異度,有助于AFP陰性HCC的診斷,與Br?ker等[10]報(bào)道類似。
約登指數(shù)亦稱正確指數(shù),是評(píng)價(jià)診斷性試驗(yàn)研究真實(shí)性的有效方法[11],其數(shù)值越大,檢測(cè)試驗(yàn)真實(shí)性越高。本研究發(fā)現(xiàn)GP73用于HCC診斷的約登指數(shù)為0.740,其線下面積大于AFP線下面積,差異有統(tǒng)計(jì)學(xué)意義,提示GP73診斷HCC的效能優(yōu)于AFP。針對(duì)AFP<20.00 ng/ml的患者,采用GP73診斷,其約登指數(shù)亦可達(dá)0.505,其線下面積亦大于AFP線下面積,差異有統(tǒng)計(jì)學(xué)意義,提示GP73用于HCC診斷的約登指數(shù)較高,診斷的真實(shí)性好[12]。
AFP是目前臨床應(yīng)用最廣的輔助診斷HCC的傳統(tǒng)方法,本研究對(duì)入選標(biāo)本檢測(cè)發(fā)現(xiàn)其靈敏度和特異度分別為53.8%和84.6%,仍有一定局限性。GP73是近年來用于HCC診斷的新方法,本組同份標(biāo)本采用GP73檢測(cè),結(jié)果顯示靈敏度和特異度分別為73.8%和88.6%,雖然較AFP檢測(cè)有一定提高,但仍有部分患者低于檢測(cè)水平,提示單純以GP73檢測(cè)亦有一定局限性。采用GP73聯(lián)合AFP檢測(cè),靈敏度和特異度分別達(dá)92.3%和83.1%,均明顯優(yōu)于上述單一檢測(cè)方法,提示GP73聯(lián)合AFP檢測(cè)可進(jìn)一步提高HCC診斷的靈敏度和特異度,此結(jié)果與之前報(bào)道類似[13-15]。
綜上所述,GP73是診斷HCC的一種新型血清學(xué)指標(biāo),具有良好的靈敏度和特異度,檢測(cè)結(jié)果真實(shí)性高,是輔助診斷HCC的有效方法。GP73聯(lián)合AFP檢測(cè)可進(jìn)一步提高HCC診斷的靈敏度和特異度[16],有效克服因單一實(shí)驗(yàn)室診斷所致的局限性,具有良好的臨床應(yīng)用價(jià)值。
[1]C hen K,ShiW,Xin Z,etal.R eplication of genomewide a ss ociation s tudie s on hepatocellula r ca r cinoma s u s ceptibility loci in a C hine s e population[J].PL oS O ne,2013,8(10):e77315.
[2]Shan SG,Gao YT,Xu Y J,etal.G r adually inc r ea s ed Golgi p r otein 73 e x p r e ss ion in the p r og r e ss ion of benign live r di s ea s e s to p r ecance r ou s le s ion s and hepatocellula r ca r cinoma co rr elate s with p r ogno s i s of patient s[J].Hepatol R e s,2013,43(11):1199-1210.
[3]O zkan H,E r dalH,Tutkak H,etal.Diagno s tic and p r ogno s tic validity of Golgi p r otein 73 in hepatocellula r ca r cinoma[J].Dige s tion,2011, 83(1-2):83-88.
[4]中華醫(yī)學(xué)會(huì)傳染病與寄生蟲病學(xué)分會(huì),中華醫(yī)學(xué)會(huì)肝病學(xué)分會(huì).病毒性肝炎防治方案[J].傳染病信息,2000,13(4):141-150
[5]Sha r iff M I,C o x I J,Gomaa A I,et al.Hepatocellula r ca r cinoma: cu rr ent t r end s in wo r ldwide epidemiology,r i s k facto rs,diagno s i s and the r apeutic s[J].E x pe r t R ev Ga s t r oente r ol Hepatol,2009,3(4): 353-367.
[6]A s ham EH,K a s eb A,Ghob r ial R M.Management of hepatocellula r ca r cinoma[J].Su r g C lin No r th Am,2013,93(6):1423-1450.
[7]Xu J B,Q i FZ,Xu G,etal.Value of alpha-fetop r otein and clinical cha r acte r i s tic s in patient s with live r neopla s m[J].Neopla s ma,2014, 61(2):218-224.
[8]Si r ipong s akun S,Wei SH,L in S,etal.Evaluation of alpha-fetop r otein in detecting hepatocellula r ca r cinoma r ecu rr ence afte r r adiof re q uency ablation[J].J Ga s t r oente r ol Hepatol,2014,29(1):157-164.
[9]K ladney R D,C ui X,B ulla GA,et al.E x p r e ss ion of G P73,a r e s ident Golgi memb r ane p r otein,in vi r al and nonvi r al live r di s ea s e[J].Hepatology,2002,35(6):1431-1440.
[10]Br?ke r ME,I j ze r man s J N,Wit j e s C D,etal.The p r edictive value of Golgip r otein 73 in diffe r entiatingbenign f r ommalignant live r tumo rs[J].PL oS O ne,2014,9(7):e100187.
[11]L uo J,Xiong C.Youden inde x and a ss ociated cut-point s fo r th r ee o r dinal diagno s tic g r oup s[J].C ommun Stat Simul C omput,2013,42 (6):1213-1234.
[12]Hu B,Tian X,Sun J,etal.Evaluation of individual and combined application s of s e r um bioma r ke rs fo r diagno s i s of hepatocellula r car cinoma:ameta-analy s i s[J].I nt J Mol Sci,2013,14(12):23559-23580.
[13]Mao Y,Yang H,Xu H,etal.Golgi p r otein 73(G O LP H2)i s a valuable s e r um ma r ke r fo r hepatocellula r ca r cinoma[J].Gut,2010,59 (12):1687-1693.
[14]Wang NY,Wang C,L iW,et al.Pr ogno s tic value of s e r um AF P, AF P-L3,and G P73 in monito r ing s ho r t-te r m t r eatment r e s pon s e and r ecu rr ence of hepatocellula r ca r cinoma afte r r adiof r e q uency abla-tion[J].A s ian P ac J C ance r Pr ev,2014,15(4):1539-1544.
[15]Hou S C,Xiao M B,Ni R Z,et al.Se r um G P73 i s complementa r y to AF P and GGT-II fo r the diagno s i s of hepatocellula r ca r cinoma[J]. O ncol L ett,2013,6(4):1152-1158.
[16]Wang Y,Yang H,Xu H,etal.Golgi p r otein 73,not Glypican-3, may be a tumo r ma r ke r complementa r y toα-fetop r otein fo r hepatocellula r ca r cinoma diagno s i s[J].J Ga s t r oente r ol Hepatol,2014,29 (3):597-602.
(2014-08-05收稿 2014-09-05修回)
(責(zé)任編委 王永怡 本文編輯 陳玉琪)
Diagnostic value of Golgi protein 73 alone and in combination w ith alpha fetoprotein in hepatocellular carcinoma
ZHANG Jin-yin,HUWan-fa,WANG Jian,WEIHong-shan*
Department of Laboratory,Chaoyang Hospital of Huainan,Huainan,Anhui232001,China
*Corresponding author,E-mail:drliver@163.com
Objective To investigate the value of serum Golgiprotein 73(GP73)alone and in combination with alpha fetoprotein(AFP)in detecting hepatocellular carcinoma(HCC).Methods The levels of GP73 and AFP in the peripheral blood of patients with HCC,hepatitis,other tumors without HCC and controls were detected by ELISA and electrochemiluminescence immunoassay (ECLIA),respectively.Results The average level of GP73 in HCC patients was 231.2±92.3 ng/ml,markedly higher than the levels of hepatitis group,non-HCC tumor group and the control group,respectively,and the differences between the levelswere significant (P<0.005).Themaximal Youden’s index was obtained when GP73 was 81.08 ng/m l,and the corresponding sensitivity and specificity of GP73 level in the diagnosis of HCC were 86.2%and 87.8%,higher than those of AFP level.The combined detection of GP73 and AFP levels in the diagnosis of HCC made the sensitivity further increase to 92.3%.Conclusions GP73,as a novel serum marker,has a higher sensitivity and specificity in the diagnosis of HCC,and is superior to AFP.Combined detection of GP73 and AFP can further improve the sensitivity in the diagnosis of HCC.
liver neoplasms;Golgiapparatus;enzyme-linked immunosorbent assay;alpha-fetoprotein
R735.7;R329.24
A
1007-8134(2014)05-0296-03
232001,淮南朝陽醫(yī)院檢驗(yàn)科(張進(jìn)銀);232001,淮南東方腫瘤醫(yī)院檢驗(yàn)科(胡萬發(fā));232001淮南,安徽理工大學(xué)病源微生物教研組(王健);100011,首都醫(yī)科大學(xué)淮南附屬北京地壇醫(yī)院傳染病研究所(魏紅山)
魏紅山,E-mail:drliver@163.com
猜你喜歡
美與時(shí)代·美術(shù)學(xué)刊(2022年3期)2022-04-27 01:18:15
中學(xué)生數(shù)理化·七年級(jí)數(shù)學(xué)人教版(2021年6期)2021-11-22 07:50:58
中學(xué)生數(shù)理化·七年級(jí)數(shù)學(xué)人教版(2021年6期)2021-11-22 07:50:58
中學(xué)生數(shù)理化·七年級(jí)數(shù)學(xué)人教版(2021年6期)2021-11-22 07:50:58
中老年保健(2021年3期)2021-08-22 06:50:04
天津醫(yī)科大學(xué)學(xué)報(bào)(2021年2期)2021-03-29 05:31:08
現(xiàn)代臨床醫(yī)學(xué)(2021年1期)2021-01-26 00:56:02
人大建設(shè)(2019年12期)2019-05-21 02:55:32
海峽科技與產(chǎn)業(yè)(2016年3期)2016-05-17 04:32:12
現(xiàn)代檢驗(yàn)醫(yī)學(xué)雜志(2014年4期)2014-02-02 02:44:59

- 傳染病信息的其它文章
- AST高于正常值上限2倍且大于A L T對(duì)A I DS合并青霉菌病的篩查價(jià)值
- γ-干擾素釋放試驗(yàn)對(duì)結(jié)核病患者臨床診斷性能評(píng)價(jià)研究
- 肝病患者真菌感染的特點(diǎn)及耐藥性分析
- 多個(gè)地區(qū)不同來源山夫登堡沙門菌分子分型研究
- 世界衛(wèi)生組織艾滋病生存質(zhì)量簡表中文版應(yīng)用于H I V/A I DS患者的信度和效度評(píng)價(jià)
- 常用炎癥因子指標(biāo)結(jié)合終末期肝病模型評(píng)分對(duì)慢性重癥肝炎預(yù)后預(yù)測(cè)價(jià)值