老年餐后低血壓與血管內皮功能相關性研究
2012-10-17 03:29:48牛麗婷何玉梅韓慧儒
中國醫藥導報 2012年31期
關鍵詞:老年人
牛麗婷 徐 江 何玉梅 韓慧儒
河北省秦皇島市骨科醫院,河北秦皇島 066000
餐后低血壓(PPH)是指進餐后的收縮壓(SBP)和(或)舒張壓(DBP)比餐前降低 20 mm Hg(1 mm Hg=0.133 kPa)或以上;或餐后2 h之內每隔15 min測餐前SBP在100 mm Hg以上,餐后SBP在90 mm Hg以下[1-2]。本研究探索了老年餐后低血壓與血管性假血友病因子(vwF)、纖維蛋白原(Fbg)的相關性。現將結果報道如下:
1 資料與方法
1.1 一般資料
選擇2010年3月~2011年12月在我院老年科就診且明確有老年餐后低血壓的患者270例作為實驗組,其中,男162例,女 108例,平均年齡(66.56±5.48)歲。 另選取 120例老年健康者作為對照組。不同組間年齡、性別比較,差異無統計學意義(P>0.05),具有可比性。
1.2 方法
實驗組每日進餐總熱量為 105~126 kJ/(kg·d),控制餐中的蛋白質占總熱量的10%~15%,碳水化合物占50%~60%,脂肪占20%~30%。檢測餐后vwF、Fbg的表達水平,分析實驗組患者餐后低血壓與vwF、Fbg表達的相關性。
1.3 統計學方法
所得數據輸入統計軟件SPSS 15.0進行處理,計量資料用均數±標準差(±s)表示,組間比較采用t檢驗,以P<0.05為差異有統計學意義。
2 結果
早餐后低血壓共120例,中餐后低血壓共105例,晚餐后低血壓共45例,vwF和Fbg的表達水平分別與對照組相比,差異有統計學意義(P<0.05)。餐后低血壓與vwF和Fbg的表達水平具有正相關性(r=0.589、0.603,P<0.05)。見表1、2。
表1 兩組患者餐后低血壓與vwF的關系(±s)
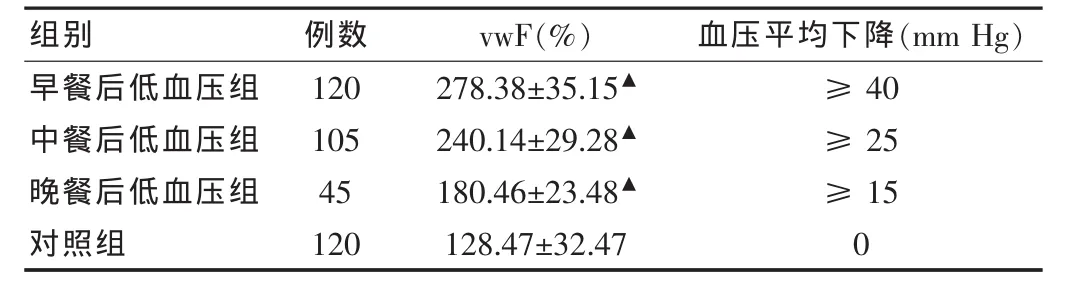
表1 兩組患者餐后低血壓與vwF的關系(±s)
注:與對照組比較,▲P<0.05
組別 例數 vwF(%) 血壓平均下降(mm Hg)早餐后低血壓組中餐后低血壓組晚餐后低血壓組對照組120 105 45 120 278.38±35.15▲240.14±29.28▲180.46±23.48▲128.47±32.47≥40≥25≥15 0
3 討論
在本研究中筆者發現,老年餐后血壓的測量中,早餐后平均下降40 mm Hg的老年人有120例,中餐后平均下降25 mm Hg的老年人有105例,晚餐后平均下降15 mm Hg的老年人有45例,因此,老年人發生餐后低血壓的發生率以早餐后最高,中餐次之,晚餐最末。老年人由于身體各臟器老化,易導致內皮損傷,造成心腦血管疾病的發生。vwF是血管內皮細胞受損的重要標志物。有研究表明,vwF為細胞外基質的組成成分,在肝臟損傷和修復過程中發揮積極作用[3-7]。血管內皮是合成vwF的主要場所,vwF的功能是調節血小板黏附,促進凝血,vwF是目前反應內皮細胞功能的最好的生化指標。Fbg升高能夠激活Ⅶ因子,促進血小板凝集,并且激活纖維溶酶激活抑制劑,導致纖維機制的異常,影響內皮功能[8-11]。在本研究中筆者發現,老年餐后vwF和Fbg的表達水平分別與對照組相比,差異有統計學意義(P<0.05)。同時,筆者進行了老年餐后低血壓與血管內皮功能關系的研究,研究發現,餐后低血壓與vwF和Fbg的表達水平具有正相關性(r=0.589、0.603,P<0.05)。 推測這個結果可能與餐后血壓下降的水平超過了老年人心腦血管自身調節的閾值,從而導致了內皮紊亂,內皮功能損害。本研究的結果將為老年餐后低血壓的治療提供新方法和新依據。
表2 兩組患者餐后低血壓與Fbg的關系(±s)
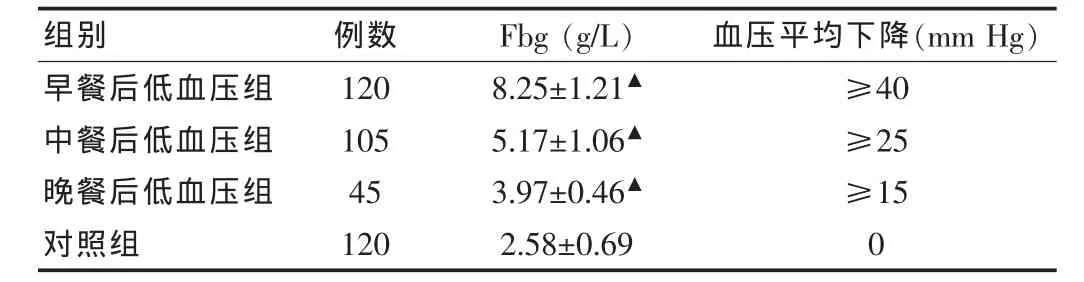
表2 兩組患者餐后低血壓與Fbg的關系(±s)
注:與對照組比較,▲P<0.05
組別 例數 Fbg(g/L) 血壓平均下降(mm Hg)早餐后低血壓組中餐后低血壓組晚餐后低血壓組對照組120 105 45 120 8.25±1.21▲5.17±1.06▲3.97±0.46▲2.58±0.69≥40≥25≥15 0
[1]Choi JH, Lee HS, Lee TY,et al.A case of postprandial hypotension in the intensive care unit treated with acarbose[J].Korean Circ J,2011,41(10):629-631.
[2]Luciano GL,Brennan MJ,Rothberg MB.Postprandial hypotension[J].Am J Med,2010,123(3):281.
[3]Lubart E,Segal R,Baumoehl Y,et al.Postprandial hypotension in longterm care elderly patients on enteral feeding[J].J Am Geriatr Soc,2006,54(9):1377-1381.
[4]Ignashov AM,Tiurina TV,Vrabii AA,et al.Postprandial hypotension in patients with compression of the celiac trunk[J].Vestn Khir Im I I Grek,2010,169(5):66-70.
[5]Son JT,Lee E.Prevalence and risk factors of postprandial hypotension in Korean elderly people[J].J Korean Acad Nurs,2009,39(2):198-206.
[6]Villavicencio CC,Miralles BR,Gonzalez MP,et al.Orthostatic and postprandial hypotension in elderly patients with chronic diseases and disability:prevalence and related factors[J].Rev Esp Geriatr Gerontol,2009,44(1):12-18.
[7]Jian ZJ,Zhou BY.Efficacy and safety of acarbose in the treatment of elderly patients with postprandial hypotension[J].Chin Med J(Engl),2008,121(20):2054-2059.
[8]Catz A,Bluvshtein V,Pinhas I,et al.Hemodynamic effects of liquid food ingestion in mid-thoracic paraplegia:is supine postprandial hypotension related to thoracic spinal cord damage[J].Spinal Cord,2007,45(1):96-103.
[9]Tanakaya M,Takahashi N,Takeuchi K,et al.Postprandial hypotension due to a lack of sympathetic compensation in patients with diabetes mellitus[J].Acta Med Okayama,2007,61(4):191-197.
[10]Shibao C,Gamboa A,Diedrich A,et al.Acarbose,an alpha-glucosidase inhibitor,attenuates postprandial hypotension in autonomic failure[J].Hypertension,2007,50(1):54-61.
[11]王津,史衛國,畢建亭.丹紅注射液對不穩定型心絞痛病人炎癥反應物及纖溶活性的影響[J].中西醫結合心腦血管病雜志,2007,5(8):673-575.
猜你喜歡
保健醫苑(2022年1期)2022-08-30 08:40:44
公民與法治(2022年4期)2022-08-03 08:20:26
保健醫苑(2022年6期)2022-07-08 01:25:16
保健醫苑(2022年4期)2022-05-05 06:11:20
中老年保健(2021年4期)2021-08-22 07:10:20
保健醫苑(2021年7期)2021-08-13 08:47:44
公民與法治(2020年18期)2020-10-28 08:48:10
保健醫苑(2020年1期)2020-07-27 01:58:14
家庭醫學(下半月)(2020年1期)2020-05-11 02:05:28
海峽姐妹(2018年1期)2018-04-12 06:44:24
