米索前列醇預防產后出血52例分析
2012-01-26 07:59:50胡珊,胡燕
重慶醫學 2012年18期
胡 珊,胡 燕
(重慶武警總隊醫院婦產科,重慶 400061)
米索前列醇預防產后出血52例分析
胡 珊,胡 燕
(重慶武警總隊醫院婦產科,重慶 400061)
目的探討米索前列醇在預防產后出血中的效果?方法 回顧性分析該院2009年1月至2010年12月100例正常單胎足月的自然分娩患者,將其隨機分為觀察組52例和對照組48例,觀察組產婦在胎兒娩出后口服米索前列醇片400μg或600 μg,對照組在胎兒娩出后肌內注射縮宮素20U,分別測定兩組產婦的出血量?第三產程時間?產后出血發生率和血壓等指標?結果兩組在第三產程時間?產后2h出血量?產后出血發生率等方面比較,差異有統計學意義(P0.05)?結論米索前列醇口服給藥促進子宮收縮作用強于肌內注射縮宮素,能有效縮短第三產程,減少產后出血?
產后出血;米索前列醇;產程,第三;預防和防護用藥
產后出血是指胎兒娩出后產婦24h內陰道流血量超過500mL?產后出血是產科的嚴重并發癥,在中國乃至于世界范圍內,位居產婦死亡原因首位?25%的圍產期死亡是由于出血,而每年因產后出血而受到死亡威脅的產婦達到2 000萬[1]?第三產程平均持續10~15min,而超過30min通常被認為是延長了?即使在第三階段積極處理,仍有3%的產婦出現第三產程延長?胎盤滯留可能由簡單的粘連胎盤或不同的病態粘連所引起,包括侵入性胎盤?植入胎盤等?而已經觀察到粘連胎盤與宮腔粘連?子宮內膜炎?繼往子宮手術或子宮腔異常相關?對第三產程的積極處理,如在胎肩出來后,肌內注射縮宮素或甲麥角新堿,可以顯著降低胎盤滯留的發生率,并顯著降低圍產期早期和晚期出血的發病率[2]?
手取胎盤是滯留胎盤的一種處理方式?然而,它與子宮內膜炎?出血及子宮壁創傷性穿孔的高風險相關,且需要使用全身或局部麻醉?滯留胎盤的有效藥物治療是基于對子宮肌層的刺激性收縮,如果力量足夠的話,可以誘導胎盤的分離[3]?
縮宮素?麥角新堿和前列腺素均誘導持久的子宮肌層收縮?最近的研究已經發現,通過臍靜脈注射使用的子宮收縮藥可能在對滯留胎盤的處理中是有效的[4]?繼往臨床常用的子宮收縮藥有縮宮素?前列腺素衍生物?鈣劑?垂體后葉素?止血藥治療?近年來,米索前列醇因其高效?不良反應少而逐漸應用廣泛[5-6]?本院產科自2009年1月至2010年12月,使用米索前列醇預防產后出血,取得良好效果,現報道如下?
1 資料與方法
1.1 一般資料 2009年1月至2010年12月在本院產科自然分娩的產婦100例,年齡21~42歲,孕周37~41周,按隨機原則將其分為觀察組52例,對照組48例?兩組產婦的年齡?孕周?孕產次?新生兒體質量比較,差異無統計學意義(P0.05)?
1.2 方法
1.2.1 給藥方法 觀察組產婦在胎兒娩出后立即口服米索前列醇片,患者體質量在50kg以上者服600μg,≤50kg服400 μg(每片200μg);對照組在胎兒娩出后立即肌內注射縮宮素20U?
1.2.2 產后出血評定標準 產后2h出血量大于或等于400 mL或24h內產婦陰道流血量大于或等于500mL為產后出血診斷標準?
1.2.3 觀察指標 記錄第三產程時間,產后2h陰道出血量及兩組用藥前及用藥后30和120min的心率?血壓?
1.2.4 出血量計算方法 胎兒娩出后,用接血盤放在臀部下方收集血液,離開產床后使用衛生墊,2h后使用電子秤稱質量,使用容積法聯合稱質量法測量出血量?出血量=(已用過用品質量-用品用前質量)/1.05+直接收集的血液體積[1]?
1.3 統計學處理 運用SPSS12.0統計軟件對數據進行處理,計量資料采用±s表示,以P0.05為差異有統計學意義?
2 結 果
2.1 兩組患者第三產程時間及產后出血量比較 觀察組第三產程時間短于對照組,產后2h出血量?產后24h出血量少于對照組,兩組比較差異有統計學意義(P0.05)?觀察組無產后出血發生,對照組出現1例產后出血(2.08%),兩組比較差異無統計學意義(P0.05)?見表1?
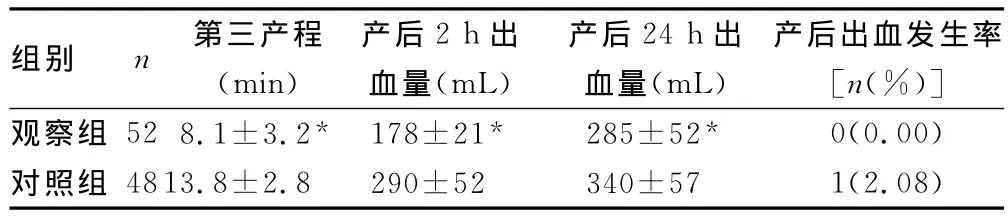
表1 兩組第三產程時間及產后出血量比較

表2 兩組產婦用藥前后血壓和心率變化
2.2 兩組患者用藥前后心率?血壓比較 兩組患者用藥前后心率?血壓比較,差異無統計學意義(P0.05),見表2?
3 討 論
子宮收縮乏力是產后出血最常見的原因,占產后出血的90%,積極防治子宮收縮乏力性出血是降低產婦死亡的關鍵[1]?
傳統方法用縮宮素促進子宮收縮,防止產后出血,肌內注射縮宮素吸收快,3~5min即出現作用,但作用不持久,半衰期為10min;縮宮素個體差異大,其敏感性與體內雌激素和孕激素水平有密切關系[7]?因此,國際上開始使用米索前列醇替代縮宮素等藥物用于促進子宮收縮,預防產后出血?目前已經有多個多中心雙盲實驗研究對米索前列醇的作用進行了研究,取得了理想的效果[4,8]?米索前列醇系前列腺素E1的衍生物,口服2.5min后即可引起子宮收縮,半衰期為1.5h[3],作用持續時間較長,可維持子宮處于較長時間的收縮狀態,能較好地預防產婦產后2h內出血的難題[2]?
本組資料表明,口服米索前列醇可明顯縮短第三產程,減少產后2h出血量,產后出血發生率明顯減少,與對照組比較,差異有統計學意義(P0.05)?本組資料還表明,米索前列醇使用前后產婦心率?血壓無明顯變化,差異無統計學意義(P0.05)?米索前列醇可適用于合并高血壓產婦產后出血的預防,這與國內外的研究結果一致[9-10]?
可見,在第三產程早期給予米索前列醇口服,可更長久地維持子宮收縮,減少產后出血量?由于子宮收縮增強,第三產程時間縮短,胎盤剝離排出加快,由胎盤因素引起的產后出血也會有所減少?口服米索前列醇有效地解決了產后2h出血問題,具有防治產后出血效果顯著?不引起血壓升高的優點,并且價格低廉?不良反應少?值得臨床推廣?
[1] Rajan PV,Wing DA.Postpartum hemorrhage:evidencebased medical interventions for prevention and treatment[J].Clin Obstet Gynecol,2010,53(1):165-181.
[2] Sheldon WR,Blum J,Durocher J,et al.Misoprostol for the prevention and treatment of postpartum hemorrhage[J].Expert Opin Investig Drugs,2012,21(2):235-250.
[3] Prata N,Passano P,Rowen T,et al.Where there are(few)skilled birth attendants[J].J Health Popul Nutr 2011,29(2):81-91.
[4] Winikoff B,Dabash R,Durocher J,et al.Barrera G et al:treatment of post-partum haemorrhage with sublingual misoprostol versus oxytocin in women not exposed to oxytocin during Labour:a double-blind,randomised,non-inferiority trial[J].Lancet,2010,375(9710):210-216.
[5] Chaudhuri P,Biswas J,Mandal A.Sublingual misoprostol versus intramuscular oxytocin for prevention of postpartum hemorrhage in low-risk women[J].Int J Gynaecol Obstet,2012,116(2):138-142.
[6] Ha MR,Alsahly N.Rectal versus oral misoprostol for active management of third stage of labor:a randomized controlled trial[J].Arch Gynecol Obstet,2011,283(5):935-939.
[7] Harara R,Hanafy S,Zidan MS,et al.Intraumbilical injection of three different uterotonics in the management of retained placenta[J].J Obstet Gynaecol Res,2011,37(9):1203-1207.
[8] Widmer M,Blum J,Hofmeyr GJ,et al.Misoprostol as an adjunct to standard uterotonics for treatment of post-partum haemorrhage:a multicentre,double-blind randomised trial[J].Lancet,2010,375(9728):1808-1813.
[9] Hofmeyr GJ,Fawole B,Mugerwa K,et al.Administration of 400μg of misoprostol to augment routine active management of the third stage of labor[J].Int J Gynaecol Obstet,2011,112(2):98-102.
[10]Lin CJ,Chien SC,Chen CP:The use of misoprostol in termination of second-trimester pregnancy[J].Taiwan J Obstet Gynecol,2011,50(3):275-282.
Analysis of the effects of misoprostol on the prevention of postpartum hemorrhage in 52 cases
ObjectiveTo evaluate the effects of misoprostol on the prevention of postpartum hemorrhage.Methods100normal term single birth parturients that spontaneous labored were randomly orally given misoprostol 400or 600μg(experimental group),or intramuscularly given oxytocin 20U(control group)after fetal disengagement.The hemorrhage volume,blood pressure,the time of third stage of labo and the rate of hemorrhage were examined.ResultsThere was a remarkable difference in the time of third stage of labor,hemorrhage volume and the rate of hemorrhage between the experiment group and the control group(P0.05).ConclusionMisoprostol that orally given can effectively promote uterine contraction,decrease postpartum hemorrhage volume,reduce the third stage of labor,and is better than oxytocin.
postpartum hemorrhage;misoprostol;labor stage,third;protective agents
10.3969/j.issn.1671-8348.2012.18.016
A
1671-8348(2012)18-1832-02
2012-03-02
2012-04-22)
?基層園地?
