Introduction to 2023 Chinese expert consensus on the whole-course management of hepatocellular carcinoma
2024-05-13 07:41:42JieLiZhuoranQiJianZhangSinuoChenJinglinXia
Hepatoma Research
2024年3期
Jie Li, Zhuoran Qi, Jian Zhang, Sinuo Chen, Jinglin Xia
Liver Cancer Institute, Zhongshan Hospital of Fudan University, Shanghai 200032, China.
BACKGROUND ON THE CONSENSUS
Primary liver cancer is a prevalent malignant neoplasm globally, with hepatocellular carcinoma (HCC)representing 75% to 85% of cases.In 2020, China accounted for nearly half of the global new cases and deaths of liver cancer[1].Consequently, enhancing the prognosis of the overall HCC population has emerged as a pressing public health concern in China, demanding urgent attention and resolution.
In recent years, the concept of “whole-course management of HCC” has been gradually integrated into HCC treatment practices and has shown preliminary benefits.Based on existing clinical evidence, the concept aims to develop a scientifically and reasonably comprehensive patient management plan through a multidisciplinary diagnosis and treatment model for the key links in the treatment process[2].To better guide the whole-course management of HCC patients, the Chinese Association of Liver Cancer of Chinese Medical Doctor Association has gathered multidisciplinary experts and scholars in relevant fields to formulate the Chinese expert consensus on the whole-course management of hepatocellular carcinoma(2023 edition)[3].
Building upon the BCLC (barcelona clinic liver cancer) staging system[4]and China liver cancer staging(CNLC)[5], this consensus introduces two whole-course management pathways for HCC: surgical and nonsurgical [Figures 1 and 2].These pathways are designed to achieve radical surgery or explore alternative treatment options, providing tailored treatment recommendations for HCC patients based on their specific stages and treatment phases.
WHOLE-COURSE MANAGEMENT OF HCC WITH CURATIVE THERAPY AS THE GOAL
Surgical resection is considered the primary treatment option for patients diagnosed with CNLC stage I and IIa, for whom preoperative neoadjuvant therapy is in the preliminary stage of exploration.As patients with technically resectable tumors classified as CNLC stage IIb and IIIa exhibit high-risk factors for recurrence,neoadjuvant therapy is recommended with options including first-line targeted therapy combined with immunotherapy or systemic therapy in conjunction with transcatheter arterial chemoembolization(TACE)[6,7].Additionally, neoadjuvant radiotherapy is recommended for patients with type II/III portal vein tumor thrombus (PVTT)[8].
Adjuvant therapy refers to the postoperative treatment administered to HCC patients who received radical resection with a high risk of postoperative recurrence and metastasis.However, there is still no globally recognized adjuvant treatment regimen.For hepatitis B-related HCC, the consensus points out that continued antiviral therapy is necessary after surgery.For HCC patients with a high risk of postoperative recurrence, adjuvant TACE can reduce the recurrence rate and prolong the survival time[9,10].Postoperative radiotherapy has shown the potential to improve disease-free survival (DFS) and overall survival (OS) for HCC patients with type I/II PVTT and narrow resection margins[11-13].In addition, a Chinese randomized controlled trial (RCT) study confirmed that Huaier granules, a kind of traditional Chinese medicine, could inhibit tumor recurrence and extrahepatic metastasis after HCC surgery[14].
WHOLE-COURSE MANAGEMENT OF HCC WITH NON-CURATIVE THERAPY AS THE GOAL
The treatment plan for non-surgical HCC patients should be tailored according to liver function.Priority should be given to selecting the initial treatment option that effectively controls the primary liver cancer lesion and multidisciplinary comprehensive treatment should be timely adopted to prolong the survival time and improve the quality of life.
Systemic therapy
The selection of first-line treatment should consider various factors, including the overall performance status, liver function status, tumor characteristics, treatment risks, and treatment goals of the patients.Aggressive systemic therapy could be considered in HCC patients with Child-Pugh class A or B ≤ 7.Targeted therapy combined with immunotherapy is the recommended systemic treatment approach, such as atezolizumab plus bevacizumab[15,16], sintilimab plus bevacizumab biosimilar[17], and apatinib plus camrelizumab[18].For patients who are contraindicated or unwilling to use immune checkpoint inhibitors(ICIs), targeted monotherapy including sorafenib[19], lenvatinib[20]and donafenib[21]can be considered.In cases where there is a high risk of bleeding, dual immunotherapy or immunotherapy monotherapy can be chosen as treatment strategies, such as durvalumab plus tremelimumab[22], durvalumab, tislelizumab[23], and nivolumab[24].FOLFOX chemotherapy can be considered for patients who are neither suitable for targeted therapy nor immunotherapy[25].
In the second-line treatment of HCC, several factors need to be taken into consideration, including tumor progression, first-line treatment, and adverse reactions.The main treatment options are regorafenib[26],apatinib[27], ramucirumab (AFP ≥ 400 ng/mL)[28], cabozantinib[29], pembrolizumab[30], camrelizumab[31], and tislelizumab[32].Notably, apart from sorafenib, there is limited support from phase III clinical trials for other second-line treatment options following the failure of new first-line treatment regimens.Treatment strategies can include sequential targeted therapy, conversion from targeted therapy to immunotherapy, or conversion from immunotherapy to targeted therapy.Moreover, second-line combined therapy may be more effective than monotherapy, which needs to be verified by large sample clinical trials[33].
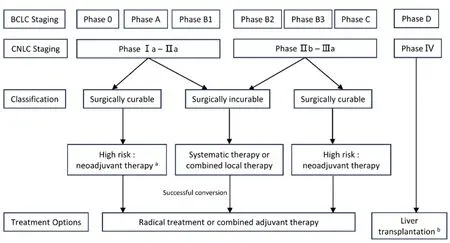
Figure 1.Whole-course management of HCC with curative therapy as the goal.a: exploration stage; b: Patients eligible for liver transplantation: Milan criteria/University of California, San Francisco (UCSF) criteria/Chinese criteria; BCLC: Barcelona clinic liver cancer; CNLC: China liver cancer staging.
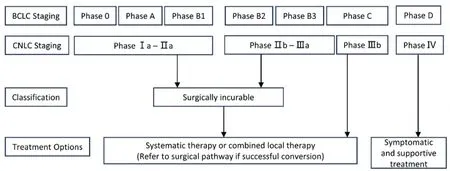
Figure 2.Whole-course management of HCC with non-curative therapy as the goal.BCLC: Barcelona clinic liver cancer; CNLC: China liver cancer staging.
Regarding the prevention and management of adverse reactions associated with systemic therapy, the consensus emphasizes the importance of conducting a comprehensive evaluation of basic organ function and tumor condition before treatment.Close monitoring and timely detection, evaluation, and management of adverse reactions during treatment are also highlighted.Depending on the type and severity of adverse effects, appropriate measures such as dose reduction, temporary suspension, or permanent discontinuation of targeted drugs[34], as well as temporary or permanent discontinuation of ICIs, should be considered[35].
Systemic therapy combined with local therapy
Local treatment has the potential to enhance the effectiveness of immunotherapy by modifying the tumor microenvironment.Additionally, the anti-angiogenic properties of targeted therapy contribute to reducing tumor recurrence following local treatment.Consequently, the combination of local and systemic therapies can effectively reduce tumor size, manage symptoms, and improve overall survival[36,37].Combination therapy may be a suitable option for liver function-preserved patients with moderate or high tumor burden,vascular invasion, and limited efficacy from local treatment alone[38].
The main combination therapy options are systemic therapy combined with TACE, hepatic arterial infusion chemotherapy (HAIC), radiotherapy, and ablation therapy.The targeted therapy plus TACE has shown promise in improving the survival outcomes of patients with advanced HCC[39,40].Several clinical trials investigating the combination of targeted therapy and immunotherapy with TACE are currently underway(NCT03572582; NCT03143270; NCT04340193; NCT04268888).Notably, Chinese researchers have made significant advancements in the treatment of HCC using HAIC based on FOLFOX chemotherapy.The results of phase III clinical trials have demonstrated that targeted therapy plus FOLFOX-based HAIC can further improve the survival of advanced HCC patients with PVTT[41].Despite encouraging preclinical findings, systemic therapy plus radiotherapy and systemic therapy plus ablation are still in the early stages of development and require more phase III clinical trials to provide evidence of efficiency and safety.
Conversion therapy
For patients with unresectable (or potentially resectable) HCC, more aggressive transformation strategies can be employed, particularly by selecting those with high overall response rates.The primary approach for conversion therapy is the first-line targeted drugs combined with immunotherapy, along with the optional inclusion of local therapy[42,43].Patients who experience tumor regression or downstaging following treatment should undergo comprehensive multidisciplinary discussions and evaluations to determine the feasibility of surgical intervention.Patients who are unable to successfully transition to resectable HCC should be treated according to the therapeutic principles established for unresectable HCC[44].
Whole-course management of special groups
The majority of clinical studies have excluded special populations, such as organ transplant recipients,individuals with decompensated cirrhosis, autoimmune diseases, and renal insufficiency, making the treatment particularly challenging.This consensus provides a comprehensive overview of the present status,contraindications, challenges, and outstanding issues concerning systemic therapy in special HCC patient populations.Due to limited large-scale research data and limited clinical application experience, the use of immunotherapy in patients with organ transplantation or autoimmune diseases should be approached with caution in combination with specialist opinions.In the management of these patients, individualized treatment protocols, safety evaluation, and collaboration among multidisciplinary teams are important components.
SYMPTOMATIC SUPPORTIVE TREATMENT AND FOLLOW-UP MANAGEMENT OF HCC
Patients diagnosed with HCC should receive comprehensive management that includes symptomatic and supportive treatment throughout the course of their disease.Preserved liver function is an important prerequisite to delivering effective treatment to HCC patients.However, it is susceptible to compromise by underlying liver disease, tumor progression, and adverse treatment reactions, directly impacting patients'prognosis.Close monitoring of liver function is essential before and during tumor treatment, with appropriate liver-protective measures implemented[45,46].In cases of drug-induced liver injury (DILI), a comprehensive evaluation should be conducted, and anti-tumor drug dosages may need to be reduced or temporarily discontinued.Antiviral therapy plays a crucial role in delaying disease progression, preventing HCC recurrence, and extending overall survival in patients with hepatitis B-related HCC[47].For patients with advanced HCC, evaluations of multidisciplinary teams and timely initiation of interventions are necessary for complications such as severe ascites, jaundice, hemorrhage, and hepatic encephalopathy.Moreover, patients should undergo continuous follow-up after treatment.Regular evaluations of intra- and extrahepatic tumors, as well as monitoring of underlying liver disease and adverse reactions, should be conducted based on the patient's tumor status and treatment modalities.
CONCLUSIONS
The whole-course management of HCC is based on standardized diagnosis and treatment, emphasizing multidisciplinary collaboration to develop individualized treatment plans that encompass the whole disease process of patients, including diagnosis, treatment, evaluation, and follow-up.In fact, this is consistent with the concept of “personalized management” in a recent policy review that proposed an HCC multiparametric therapeutic hierarchy in the context of multidisciplinary tumor boards[48].As ICIs transformed the treatment landscape for HCC, systemic therapy has become the core of the whole-course management of HCC, but several challenges persist, including exploring optimal sequence and combinatorial strategies,overcoming drug resistance, screening biomarkers for predicting patient suitability and treatment outcomes, and managing immune-related adverse reactions.Furthermore, stronger evidence support is required for adjuvant and neoadjuvant therapies, systemic therapy in combination with local treatment, and the continuation of third-line treatment.
This consensus proposes two whole-course management pathways for HCC, outlining the treatment options throughout all stages of the disease based on systemic therapy, which purposefully covers the treatment recommendations for special HCC patients.Furthermore, it highlights that symptomatic treatment and regular follow-up are important components of the whole-course management of HCC.With the ongoing advancement and diversification of the HCC treatment landscape, the whole-course management model of HCC is expected to become a vital approach to diagnosis and treatment, ultimately promoting the survival and quality of life of HCC patients.
DECLARATIONS
Authors’ contributions
Conception and design: Xia J
Manuscript writing: Li J, Qi Z, Zhang J, Chen S
Availability of data and materials
Not applicable.
Financial support and sponsorship
This work was supported by the National Natural Science Foundation of China (No.81972233; No.82373086).
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
? The Author(s) 2024.
登錄APP查看全文

- Hepatoma Research的其它文章
- Introduction of Chinese expert consensus on neoadjuvant therapy for primary liver cancer (2023 edition)
- Reflections and perspectives on adjuvant treatment in the setting of resected hepatocellular carcinoma
- Dysmetabolic comorbidities and non-alcoholic fatty liver disease: a stairway to metabolic dysfunctionassociated steatotic liver disease
- Progression of liver disease and associated risk of hepatocellular carcinoma
- Role of temporary portosystemic surgical shunt during liver resection to prevent a post-resection small for size-like syndrome
- The role of percutaneous hepatic perfusion (PHP) in the treatment of cholangiocarcinoma