A case of pulmonary mucormycosis presented with cardiac arrest
2023-11-27 10:51:14HaijiangZhouXuanQiJifeiCaiWenxinLiuChenyuKangGuyuZhangMiaomiaoWangXuefeiXieChaoLiangLihuaLiuJieGaoWeiYuanXueMeiShubinGuo
Haijiang Zhou, Xuan Qi, Jifei Cai, Wenxin Liu, Chenyu Kang, Guyu Zhang, Miaomiao Wang, Xuefei Xie,Chao Liang, Lihua Liu, Jie Gao, Wei Yuan, Xue Mei, Shubin Guo
Emergency Medicine Clinical Research Center, Beijing Chao-yang Hospital, Capital Medical University, Beijing Key Laboratory of Cardio-Pulmonary Cerebral Resuscitation, Beijing 100020, China
Mucormycosis is an uncommon and opportunistic fungal infection with high mortality.Infections may result from ingestion of contaminated food, inhalation of spores into the respiratory tract or inoculation into disrupted skin.[1]Pulmonary mucormycosis (PM) is the most common clinical type.Mucormycosis mostly occurs in patients with immunocompromised conditions,organ transplantations, neutropenia, autoimmune disorders or poorly controlled diabetes.The diagnosis of mucormycosis relies on histopathology and culture,while the lipid formulations of amphotericin B are the main choice of therapy.However, cardiac arrest caused by PM has rarely been reported before.Here, we report a case admitted to our center aimed at enhancing awareness among emergency physicians.
CASE
An 18-year-old man presented to our center with a chief complaint of intermittent dyspnea and cough for two months in February 2023.About two months ago,he experienced sudden appearance of dyspnea after recovery from COVID-19.The dyspnea was intermittent and could be relieved after a fit of cough every time.He had only a small amount of white sputum while he had no bloody sputum, fever or chest pain.He denied a definite previous history of bucking and choking.His blood glucose level was found elevated about one month ago (fasting blood glucose level about 14 mmol/L), but he did not receive standard treatment.About 10 h before his presentation, he suffered a severe cough again and the symptoms persisted.He lost consciousness and had a cardiac arrest after emergency consultation in the local hospital.Cardiopulmonary resuscitation,endotracheal intubation and mechanical ventilation were performed in the emergency room.Computed tomography (CT) scanning revealed the foreign bodies in the trachea (Figure 1).To receive further treatment, he was transferred to our center.
His body mass index (BMI) was 15.94 kg/m2.Routine blood tests on admission revealed the elevated levels of white blood cell count (12.36×109/L, reference range [ref.] [3.5–9.5]×109/L) and neutrophil count(11.44×109/L, ref.[1.8–6.3]×109/L), and the decreased levels of lymphocyte count (0.49×109/L, ref.[1.1–3.2]×109/L) and platelet (115×109/L, ref.[125–350]×109/L),while hemoglobin was found in normal range.Blood biochemistry examination revealed hyperglycemia (16.10 mmol/L, ref.[3.9–6.1] mmol/L), decreased levels of albumin (38.8 g/L, ref.[40–55] g/L) and creatine (51.4 μmol/L, ref.[57–97] μmol/L), along with an elevated blood urea level of 8.85 mmol/L (ref.[3.1–8.0] mmol/L), while aspartate transferase, alanine aminotransferase,total bilirubin, and electrolytes were within the normal ranges.Arterial blood gas analyses revealed a pH of 7.33(ref.7.35–7.45), an oxygen partial pressure of 128.7 mmHg (ref.83–108 mmHg, 1 mmHg=0.133 kPa), while lactate, partial pressure of carbon dioxide and bicarbonate ion level were all normal.Additionally, procalcitonin level was elevated at 6.30 ng/mL (ref.<0.05 ng/mL)while C-reactive protein was normal.Myocardial enzymes and coagulation function examinations were all within the normal range.Electrocardiogram showed a sinus rhythm with a heart rate of 98 beats/min.Serum(1,3)- β-D-glucan assay and galactomannan antigen assay analyses were both negative.
Tracheoscopy examination revealed an irregularly shaped movable mass with soft tissue density in the lower trachea.The mass was extracted by grasping forceps (Figure 2).Biopsy was performed, and bronchoalveolar lavage fluid was collected and sent for culture and pathology examination.Hyphae were found on fungal smears, while the results for germiculture and fungal culture were both negative.Hematoxylineosin staining and hexamine silver staining revealed the mucor hyphae with irregular wide branches and no fixed angle (Figure 3).The diagnosis of PM was made and intravenous amphotericin B was administered.The patient was transferred to the local hospital and was now under follow-up.
DISCUSSION
Mucormycosis, an infection caused by a group of filamentous molds within the ordersMucoralesandEntomophthorales, is a rare and emerging fungal infection with high mortality.[1,2]The orderMucoralescomprises of various genera such asRhizopus,Mucor,Lichtheimia(formerlyAbsidia),Rhizomucor,Cunninghamella,Apophysomyces spp., andSaksenaea.Among these,Rhizopusis the most common genus associated with mucormycosis, followed byMucorandLichthemia.[3]
Mucoralesinfection may result from inhalation of spores into the respiratory tract, ingestion of contaminated foods or inoculation of disrupted skin or wounds.[4-6]Mononuclear and polymorphonuclear phagocytes can prevent germination of the conidia, and eliminate fungal spores and hyphae by oxidative and nonoxidative killing mechanisms.[7]However, phagocytic function impairment,hyperglycemia and acidosis could contribute to the growth and persistence of the organism.[1-3]Moreover, the iron metabolism may also play a vital role in the pathogenesis of mucormycosis.Mucormycosis also exhibits angioinvasive propensity, resulting in thrombosis, necrosis and tissue infarction.[1-3]
The incidence of mucormycosis has been on the rise due to the increasing of patients with immunocompromised conditions.However, differences in epidemiology exist among different regions.[2]Mucormycosis is uncommon in developed countries and typically affects patients with hematological malignancies, whereas patients with uncontrolled diabetes are in the majority in developing countries.The prevalence of mucormycosis ranges from 0.01 to 0.2 per 100,000 population in Europe and the U.S., while the prevalence in India is 14 per 100,000 population.[2]The exact prevalence of murcomycosis in China is unclear,while a summary analysis of 676 case reports showed that the pulmonary type is the most common type and the average total cost per patient was 166,000 CNY.[8,9]
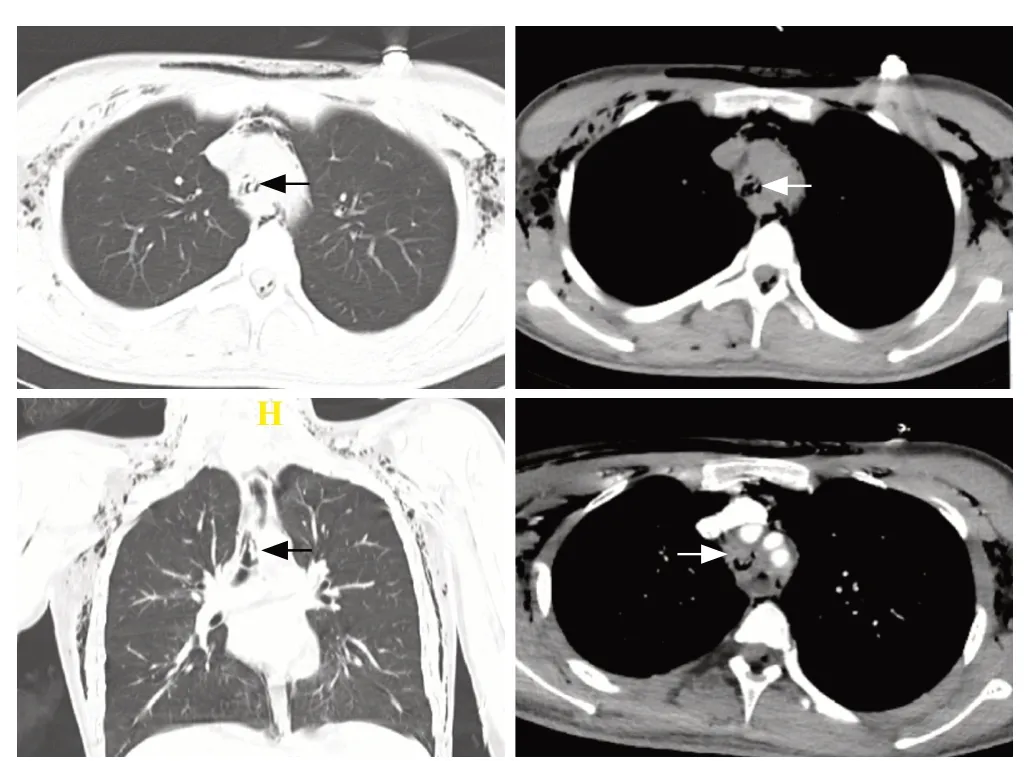
Figure 1.The computed tomography (CT) scanning of this patient at admission revealed a soft-tissue-density mass in the trachea (arrows).

Figure 2.The images during the tracheoscopy examination (A–C).Tracheoscopy revealed an irregularly shaped movable mass with soft tissue density in the lower trachea.D: the biopsy sample sent for histopathology examination.

Figure 3.The results of hematoxylin-eosin (HE) staining and hexamine silver staining.The staining revealed the mucor hyphae with irregular wide branches and no fixed angle.Above: HE staining, ×100;Below: hexamine silver staining, ×200.
Risk factors for mucormycosis include diabetes mellitus, trauma, hematological malignancies,neutropenia, solid organ or stem cell transplantation,burns and natural disaster.[10]Immunocompetent persons infected by Mucormycosis have rarely been reported.[11]Diabetes is the predominant risk factor for mucormycosis in Asia, whereas organ transplantation and hematological malignancies are more prevalent in Europe and North America.According to anatomic localization,mucormycosis can be classified into the following forms: rhino-orbito-cerebral, pulmonary, gastrointestinal,cutaneous, disseminated or mucormycosis with uncommon sites.[2]This patient had a one-month history of elevated blood glucose levels, and he did not give much importance to this issue or receive standardized treatment, which thereafter worsened his condition.
The imaging characteristics of PM are diverse.Lobar and segmental consolidation is the most common presentation, while multi-lobar distribution is less frequently reported.[12]In the early phase, initial CT scan can demonstrate perivascular ground-glass lesions prior to the progression to more extensive imaging findings.Ground-glass lesions usually develop into consolidation,nodules or masses, while necrosis is a common feature because of its vasculature invasion tendency.Invasive endobronchial or endotracheal masses as in the patient here, are rarely reported.The reverse halo sign is usually deemed a specific sign of PM, presenting in about 19%–94% of patients with PM, depending on the severity of underlying disease and the presence of neutropenia at diagnosis.[12]Moreover, the reverse halo sign is more closely related to PM than to invasive pulmonary aspergillosis.[13]In our case, CT scan at admission demonstrated segmental consolidation in the lower lobe of the left lung and a soft-tissue-density mass in the trachea, which could cause suffocation during respiration.
The diagnosis of mucormycosis includes the following elements: high index of suspicion, recognition of host factors and promptly assessment of clinical manifestations.[2]Bronchoscopic or percutaneous lung biopsy are reliable methods for diagnosing PM.[12,14]Quantitative polymerase chain reaction (qPCR) has become a promising reliable diagnostic tool in recent years.[15]According to guidelines and instructions,patients with mucormycosis were treated with amphotericin B (AmB, 0.5–1 mg/[kg·d]) or amphotericin B liposome (LAmB, 3–6 mg/[kg·d]).[16]A lipid formulation of amphotericin B was advocated as the first-line therapy for mucormycosis.[17,18]Posaconazole is recommended as salvage or maintenance therapy by European Conference on Infections in Leukemia(ECIL-6), while the European Society for Clinical Microbiology and Infectious Diseases (ESCMID) and European Confederation of Medical Mycology (ECMM)and Joint Clinical Guidelines recommend its use as first-line treatment at a dosage of 200 mg q6 h of the oral suspension.[16,17]Another salvage treatment option proposed by ECIL-6 is the combination of LAmB and caspofungin or posaconzole.[17]However, the duration of antifungal treatment has not been determined.Surgery is strongly recommended because of the enormous speed of the extension of the infection by theMucoraleshyphae.Not only the necrotic tissue but also the surrounding normal-looking tissue was advocated for resection.An adjunctive therapy is hyperbaric oxygen combined with the administration of cytokines.[2]
The mortality rate of mucormycosis is strongly correlated with the site and comorbidities.Patients with hematological malignancies or hematopoietic stem cell transplant recipients have a higher mortality rate.Mortality rates for disseminated diseases, gastrointestinal involvement and pulmonary infection were 96%, 85%and 76%, respectively.[19]The most effective predictors for mortality were rheumatological/autoimmune disease,hematological malignancies and admission to ICU.[20]
This patient had a one-month history of insufficient blood glucose control.The contraction of COVID-19 may contribute to his immune system impairment,leading to mucormycosis.The intermittent dyspnea,which could be alleviated by coughing, could be explained by the obstruction of the movable mass in the trachea.This case helps us broaden our horizon and emergency physicians should enhance awareness of mucormycosis, especially in immunocompromised patients.
Funding:This article was supported by the research grant of Sailing Plan Key Specialty (ZYLX202132) from Beijing Chaoyang Hospital, Capital Medical University, Beijing, China.
Ethical approval:This study was approved by the Institutional Review Board of Medical Ethics Committee of Beijing Chao-yang Hospital, Capital Medical University.
Conflicts of interest:The authors report no conflicts of interest.
Author contribution:All authors have substantial contributions to the acquisition, analysis, or interpretation of data for the work.HJZ and XM conceived and designed this research.HJZ, XQ and XFX collected data.HJZ, XQ, JFC, XFX, WXL, MMW, XM treated the patient.HJZ drafted the manuscript.HJZ, XM and SBG reviewed and revised the manuscript critically.All authors read and approved the final version of the submitted manuscript.
 World journal of emergency medicine2023年6期
World journal of emergency medicine2023年6期
- World journal of emergency medicine的其它文章
- The effects of hyperbaric oxygen therapy on paroxysmal sympathetic hyperactivity after cardiopulmonary resuscitation: a case series
- The effect of prophylactic antibiotics in acute upper gastrointestinal bleeding patients in the emergency department
- Uterine artery pseudoaneurysm after subtotal hysterectomy: a case report
- Tension urinothorax as a reversible cause of cardiac arrest: a case report
- Hemorrhagic pancreatitis from fenofibrate and metformin toxicity: a case report
- Pyopneumothorax caused by Parvimonas micra and Prevotella oralis: a case report