血清全氟化合物與代謝相關脂肪性肝病患病風險的關系
2023-02-24 00:58:18張露露賀穎倩趙亞楠王敏珍
中國環境科學 2023年2期
張露露,劉 婧,賀穎倩,趙亞楠,鄭 山,王敏珍
血清全氟化合物與代謝相關脂肪性肝病患病風險的關系
張露露,劉 婧,賀穎倩,趙亞楠,鄭 山,王敏珍*
(蘭州大學公共衛生學院,流行病與衛生統計學研究所,甘肅 蘭州 730000)
基于2017~2018年美國國家營養調查與健康調查數據集(NHANES),探究血清全氟化合物(PFAS)對代謝相關脂肪性肝病(MAFLD)的影響以及在不同人群中的效應差異.采用Logistic回歸模型和限制性立方樣條評估各污染物的效應和劑量反應關系.結果表明:單污染物模型發現血清全氟辛烷磺酸(PFOS)、全氟己烷磺酸(PFHxS)、全氟癸酸(PFDA)與MAFLD患病風險呈負向關聯,OR值分別為0.64(95%CI:0.45~0.91)、0.65(95%CI:0.46~0.93)、0.45(95%CI:0.30~0.67);多污染物模型中,與最低四分位數濃度(Q1)相比,血清全氟壬酸(PFNA)濃度處于Q2、Q3、Q4水平時,患MAFLD風險分別增加62%(OR=1.62,95%CI:1.10~2.39)、62%(OR=1.62,95%CI:1.01~2.60)、172%(OR=2.72,95%CI: 1.53~4.84),且呈正向線性劑量-反應關系(overall=0.002).血清PFDA處于Q2、Q3、Q4水平時,可導致MAFLD風險分別減少39%(OR=0.61,95%CI: 0.44~0.85)、46%(OR=0.54,95%CI:0.34~0.84)、74%(OR=0.26,95%CI:0.15~0.45),呈負向線性劑量-反應關系(overall<0.001).亞組分析顯示血清PFDA對51~65歲人群罹患MAFLD的影響更為顯著,而血清PFNA對女性的影響較大.綜上所述,血清PFNA及PFDA與MAFLD患病風險關聯,血清PFNA暴露是MAFLD發生的重要危險因素,而血清PFDA是保護因素, 女性、中老年人群是潛在的易感人群.
全氟化合物;代謝相關脂肪性肝病;劑量反應關系
全氟化合物(PFAS)最初在1940年代和1950年代生產[1],常用于一次性食品包裝、工業洗滌劑、消防泡沫或防水防油材料[2],具有熱穩定性、疏水性、疏油性和極低表面張力等特點,因此在環境中分布廣泛且難以降解.此外,長鏈PFAS在人體內半衰期極長[3],且在肝臟和其他器官內積累[4],因而被美國疾病控制和預防中心歸類為持久性有機污染物.雖然近年來由于各國的監管干預措施,人類對常見 PFAS的接觸逐漸減少,但其在環境中存在的普遍性和持久性仍對人類健康造成不利影響[5].研究表明, PFAS暴露與癌癥[6]、甲狀腺疾病[7]、免疫功能[8]、代謝紊亂[9]和肝臟損傷[10]等多種不良健康結局有關.
代謝相關脂肪性肝病(MAFLD)是2020年6月提出的一個非酒精性脂肪性肝病(NAFLD)新概念[11],其診斷不需排除其他慢性肝病,而是基于肝脂肪變性將肥胖癥、代謝綜合征和系統生物學的理解集中在一個焦點上[12-13].研究表明MAFLD全球患病率為38.77%[14],已成為重要的公共衛生問題.
研究表明PFAS暴露可能會增加人體代謝紊亂(如血糖、胰島素抵抗和血脂異常)和相關代謝性疾病(如2型糖尿病和代謝綜合征)發生風險[9,15-19].然而,關于PFAS與代謝紊亂的關聯存在異質性,有研究提示兩者并無關聯甚至是相反的結果[20-23].此外,PFAS可能對肝臟造成損傷,流行病學研究表明,PFAS水平與肥胖人群肝脂肪變性相關的肝功能指數呈正相關[24],并且會引起肝酶升高[25].
代謝紊亂和肝損傷是MAFLD發生的關鍵因素[26].實驗研究進一步表明,PFAS暴露會破壞正常的肝臟脂質代謝,導致肝臟脂肪變性[3,27].PFAS能夠與脂肪酸結合蛋白[28]和過氧化物酶體增殖物激活受體a(PPAR-a)[29]結合,進而破壞肝脂肪代謝及葡萄糖動態平衡、促進炎癥和MAFLD的發展.雖然關于PFAS破壞動物肝脂代謝誘發NAFLD的研究已被廣泛報道,但是關于PFAS與NAFLD之間的流行病學結果很少,與新定義MAFLD的關聯流行病學研究更是有限.
盡管以上大部分研究均支持PFAS的肝毒性和促進代謝紊亂,但也有不一致的流行病學結果.此外,目前也沒有關于PFAS與MAFLD關聯的直接流行病學證據.因此,本研究基于2017- 2018NHANES數據庫,探究常見血清PFAS與MAFLD患病風險的潛在關聯,旨在為PFAS與MAFLD患病風險研究提供最新流行病學證據,為重點人群篩查提供依據.
1 材料與方法
1.1 數據來源
美國國家營養調查與健康調查數據庫(National Health and Nutrition Examination Survey,NHANES)是一項評估美國居民健康和營養狀況的橫斷面調查,采用分層多階段抽樣設計每兩年進行一次調查,調查數據包括人口統計、膳食、生物監測、體檢和訪談等.該研究方案經美國國家衛生統計中心研究倫理審查委員會批準、參與者同意.考慮到數據庫包含PFAS和肝臟超聲彈性瞬時成像的年份,因此我們選取NHANES 2017~2018年的研究對象進行分析.
NHANES 2017~2018年數據庫中共有9254個對象,研究排除缺乏PFAS血清檢測(=7325)、肝臟瞬時彈性成像(=117)、年齡<20歲(=305)以及缺失多變量模型中重要協變量者(=332),最終納入1245名研究對象,詳細篩選流程見圖1.
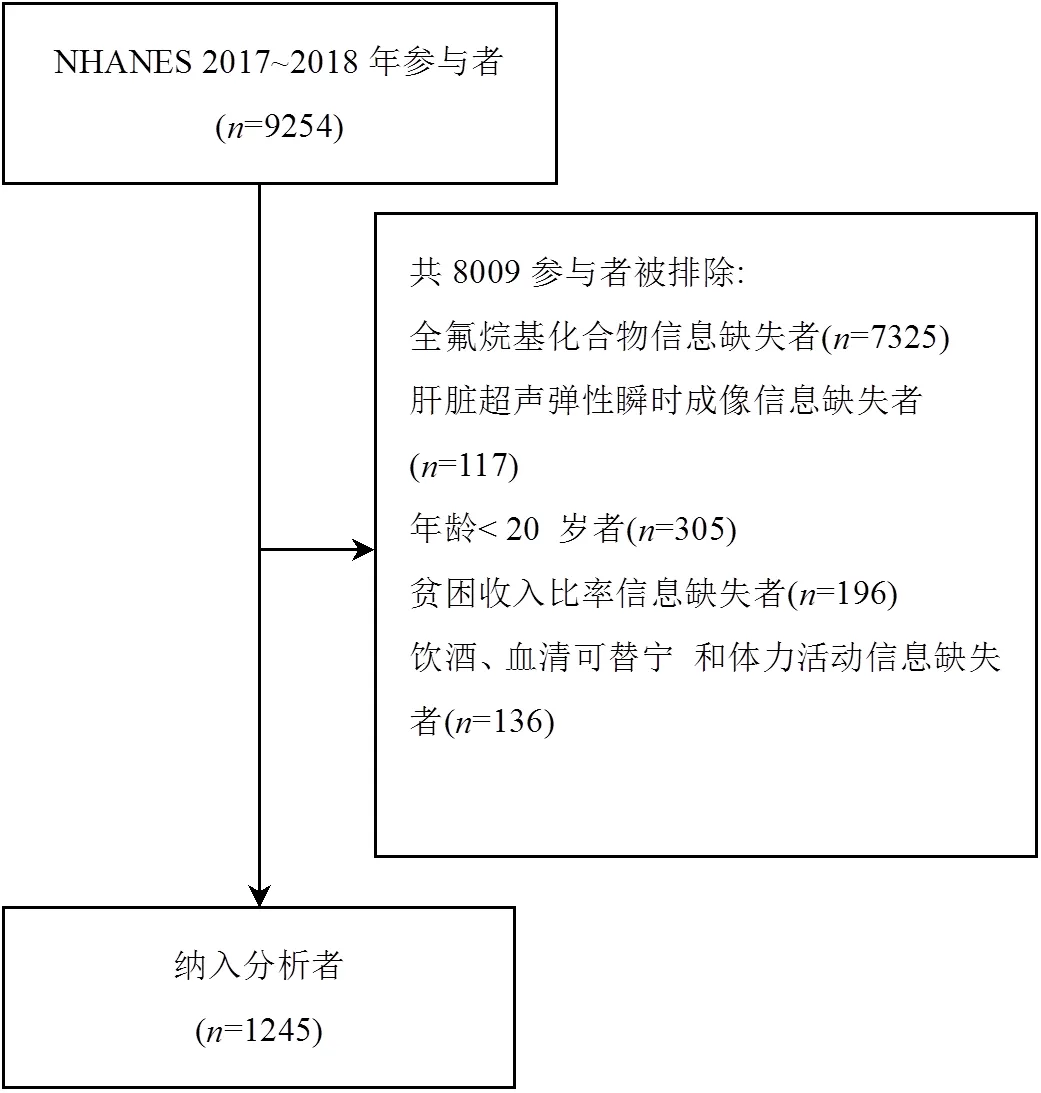
圖1 研究人群篩選過程
1.2 MAFLD的定義
采用瞬時彈性成像(FibroScan?)受控衰減參數(Controlled attenuation parameter,CAP)和肝臟硬度測量(Liver stiffness measurements,LSM)分別定義肝脂肪變性和肝纖維化.本研究參照Eddowes等人的研究[30],將CAP3274dB/m定為肝脂肪變性(該臨界值識別肝脂肪變性的敏感度為90%).排除禁食時間<3h、LSM完整讀數少于10次或LSM四分位間距范圍/LSM中位數超過30%的FibroScan?測量失敗者.
根據國際專家共識聲明[11],MAFLD診斷標準是基于肝脂肪變性證據有以下三個標準之一:超重/肥胖、2型糖尿病或代謝失調證據.代謝失調定義為滿足以下至少兩種代謝風險異常:1)男性腰圍3102cm,女性腰圍388cm;2)血壓3130/85mmHg或特定藥物治療;3)血漿甘油三酯異常(即血漿甘油三酯3150mg/dl或特定藥物治療);4)男性血漿高密度脂蛋白膽固醇<40mg/dl,女性血漿高密度脂蛋白膽固醇<50mg/dl或特定藥物治療;5)糖尿病前期(即空腹血糖水平100至125mg/d,或負荷后2h血糖水平140至199mg/dl或HbA1c 5.7%至6.4%);6)胰島素抵抗評分的穩態模型評估32.5;7)血漿高敏C反應蛋白水平>2mg/L.
1.3 血清PFAS的測定

1.4 其他變量定義
糖尿病定義根據美國糖尿病協會相關標準[31],即符合以下任何條件之一:1)自我報告診斷糖尿病.2)使用降糖藥物.3)血紅蛋白36.5% (48mmol/mol).4)空腹血糖3126mg/dl.2型糖尿病的診斷是基于糖尿病診斷,排除可能的1型糖尿病患者(診斷年齡<30歲,胰島素為唯一抗高血糖藥物).
貧困收入比(Poverty income ratio, PIR): <1.3為低、1.3~3.5為中、33.5為高.身體活動:0MET- minutes/week為不活動,1~499MET-minutes/week為低等體力活動水平,3500MET-minutes/week為中等及以上體力活動水平.
1.5 統計分析
連續變量以平均值±標準差或中位數(四分位數間距)表示,組間比較采用Student檢驗或Mann- Whitney檢驗;分類變量采用頻數(百分比)表示,組間比較采用卡方檢驗.
首先,使用Spearman相關性評估不同血清PFAS濃度之間的相關性.其次,采用logistic回歸模型以PFAS連續變量(血清PFAS值經對數變換,以10為底糾正偏態分布)和分類變量(第一分位數Q1作為參考)分別作為自變量,探究其與MAFLD發生的暴露反應關系.其中,單污染模型自變量包括單個PFAS和調整變量,多污染物模型自變量包括PFOA、PFOS、PFHxS、PFDA、PFNA以及調整變量.根據既往文獻[9,32],納入的模型調整變量包括年齡、性別、種族、貧困收入比、教育水平、身體活動、血清可替寧、飲酒.根據赤池信息準則,選取最優節點數量的限制性立方樣條進一步分析PFAS暴露與 MAFLD之間的劑量反應關系.最后采用分層多元回歸分析按年齡、性別、種族、貧困收入比、教育水平、飲酒狀況和身體活動分層進行亞組分析,交互作用分析闡明亞組之間效應的異質性,探討不同特征人群中MAFLD患病風險和血清PFAS濃度之間的關系.
數據分析采用R 4.1.3和SPSS25.0軟件完成.所有檢驗均為雙側檢驗,檢驗水準=0.05.
2 結果
2.1 一般人口學特征
本研究共納入研究對象1245名,其中MAFLD 542名(43.5%),男性占50.4%,平均年齡49.94±17.53歲.大多數參與者為非西班牙裔白人(37.5%),其次是非西班牙裔黑人(22.1%)和墨西哥裔美國人(13.6%).除貧困收入比外,MAFLD組與非MAFLD組年齡、性別、種族以及教育水平均存在統計學差異(<0.05).與非MAFLD患者相比,MAFLD患者平均年齡較高,高血壓、糖尿病、糖尿病前期、高甘油三酯血癥發生比例較高.此外血清PFDA水平在兩組差異有統計學意義,見表1.
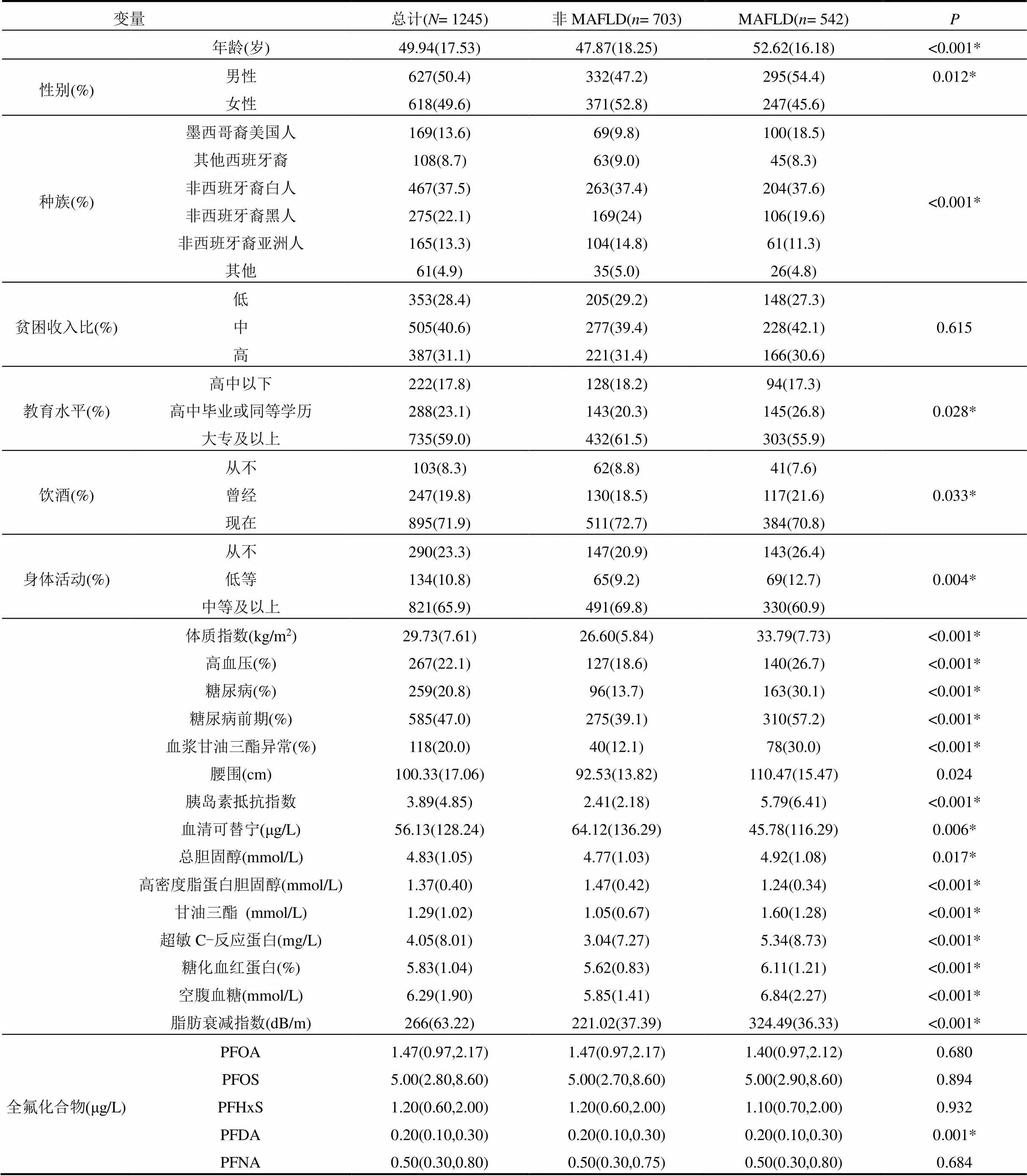
表1 一般人口學特征
注:數據描述為均值(標準差)或中位數(四分位數間距)或頻數(百分比),*表示組間差異顯著.
2.2 血清PFAS之間的相關性
由圖2所示,5種PFAS間存在不同程度的顯著相關性(<0.001),s0.27~0.74,均呈正相關.
2.3 血清PFAS濃度與MAFLD患病風險的關聯
表2顯示,在單污染物模型中,PFOS、PFHxS和PFDA與MAFLD風險降低相關,PFOS每增加一個單位,患MAFLD風險下降36%(OR=0.64,95%CI: 0.45~0.91),PFHxS每增加一個單位,患MAFLD風險下降35%(OR=0.65,95%CI: 0.46~0.93),PFDA每增加一個單位,患MAFLD風險下降55%(OR=0.45, 95%CI:0.30~0.67),趨勢性檢驗均具有統計學意義(trend<0.05).
在多污染物模型中, PFDA與MAFLD發生風險降低相關(OR=0.24,95%CI:0.13~0.43),PFNA與MAFLD發生風險增加相關(OR=2.94, 95%CI: 1.58~ 5.47).以Q1組為參照,血清PFDA 的Q2組、Q3組、Q4組的OR值分別為0.61(95%CI: 0.44~0.85) 、0.54 (95%CI:0.34~0.84)、0.26(95%CI:0.15~0.45),血清PFNA的Q2組、Q3組、Q4組的OR值分別為1.62 (95%CI:1.10~2.39)、1.62(95%CI:1.01~2.60)、2.72 (95%CI:1.53~4.84),均存在劑量反應關系(trend< 0.05).
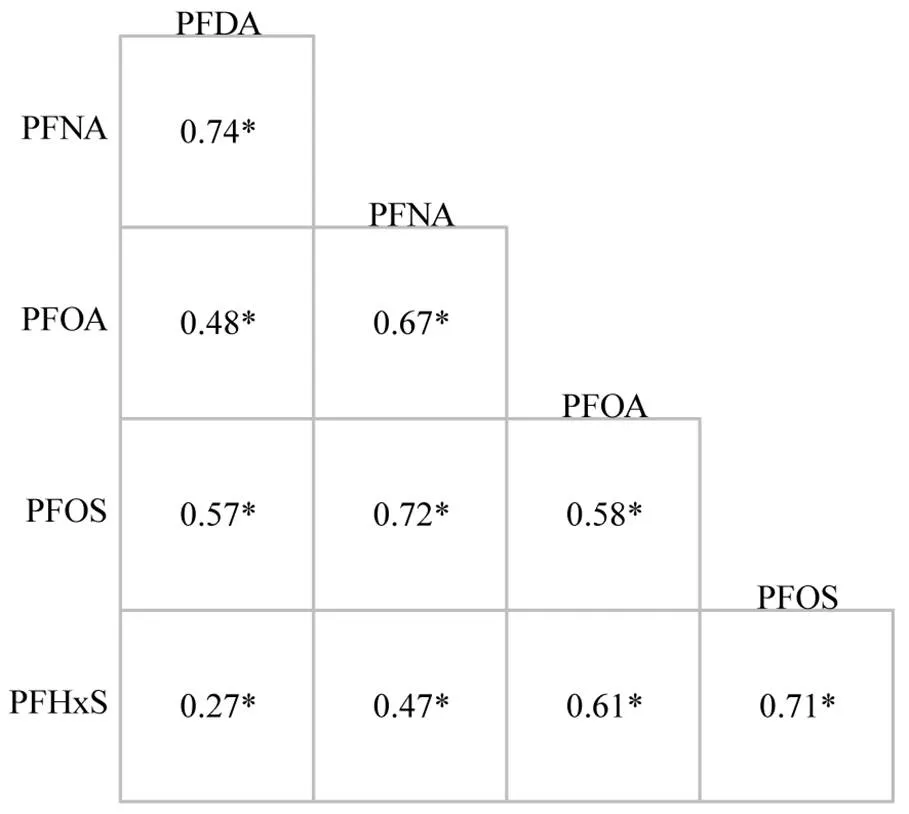
圖2 血清PFAS濃度之間的相關性
*表示顯著相關
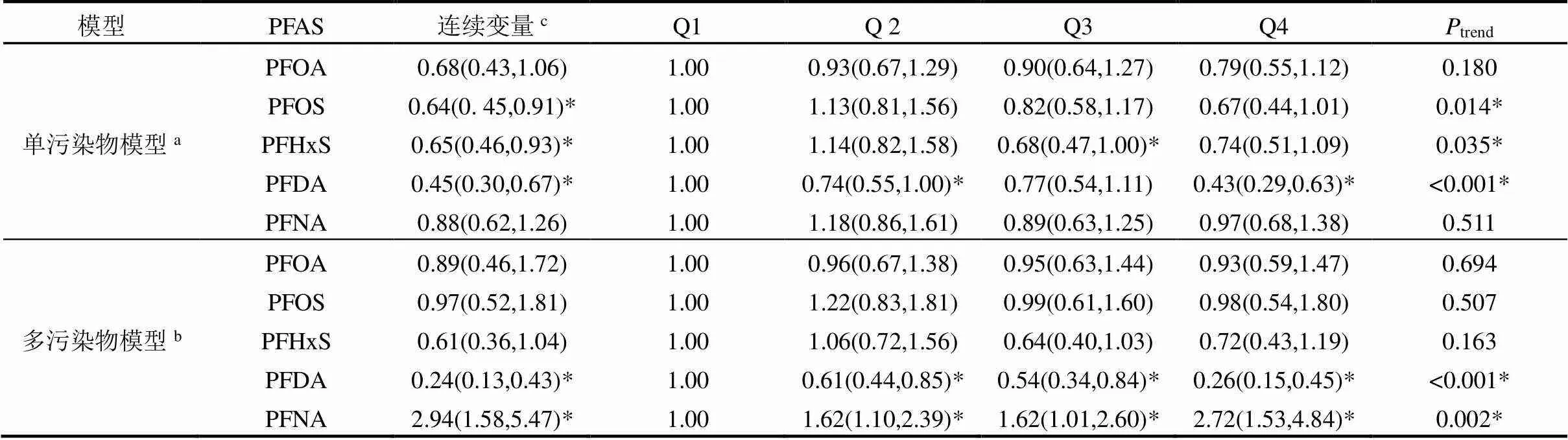
表2 血清PFAS濃度與MAFLD患病風險之間的關聯性
注:表中數字為OR(95%CI);OR,比值比;CI,置信區間;Q,四分位數;*為顯著相關. .a:單污染物模型在調整協變量基礎上一次納入一種PFAS進入模型;b:多污染物模型在調整協變量基礎上同時納入以上5種PFAS進入模型;c:血清PFAS濃度經lg10轉換.模型調整了年齡、性別、種族、貧困收入比率、教育水平、身體活動、飲酒狀況、血清可替寧.
2.4 血清PFAS與患MAFLD風險的劑量反應關系
如圖3所示,PFDA濃度與MAFLD患病風險呈負向線性劑量反應關系(overall<0.001,nonlinear= 0.484),隨著PFDA水平增加,MAFLD患病風險降低;PFNA濃度與MAFLD患病風險呈正向線性劑量反應關系(overall=0.002,nonlinear=0.452),隨著PFNA水平增加,患MAFLD風險增加.
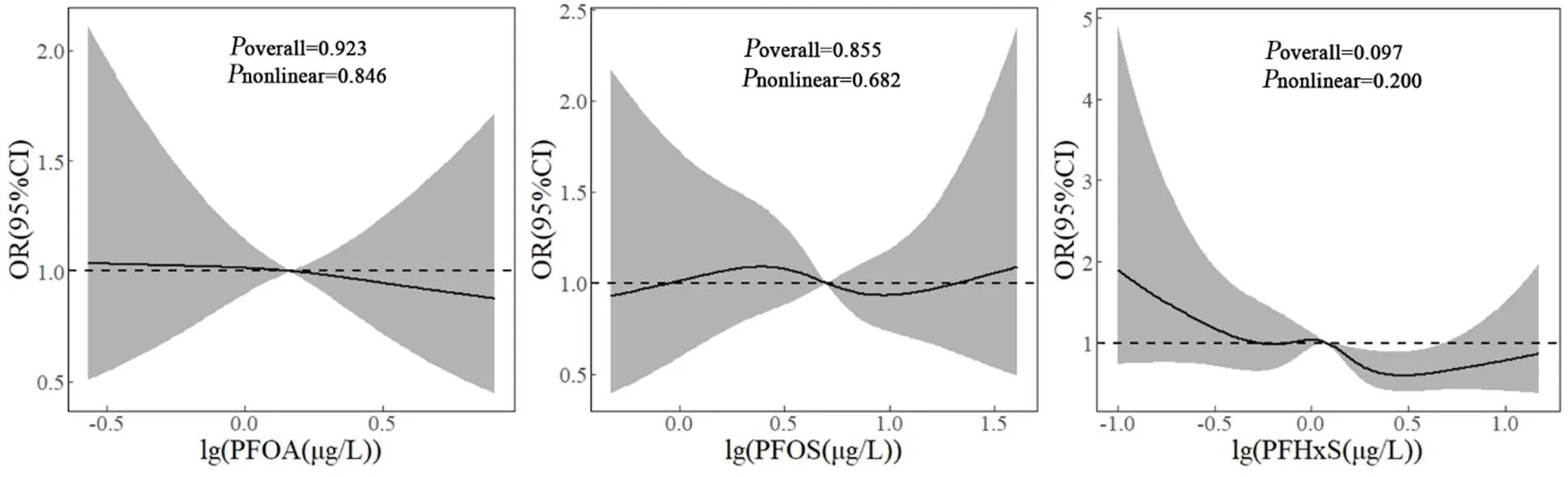
調整因素同表2
2.5 亞組分析
圖4所示為不同亞組之間血清PFDA、PFNA濃度對MAFLD患病風險的影響.血清PFDA濃度與年齡亞組之間存在顯著交互作用(inter=0.023),且在51~65歲年齡組血清PFDA與MAFLD患病風險相關性更強烈.此外,血清PFNA與性別亞組也存在顯著交互作用(inter=0.001),且在女性人群中血清PFNA與MAFLD患病風險相關性更強烈.
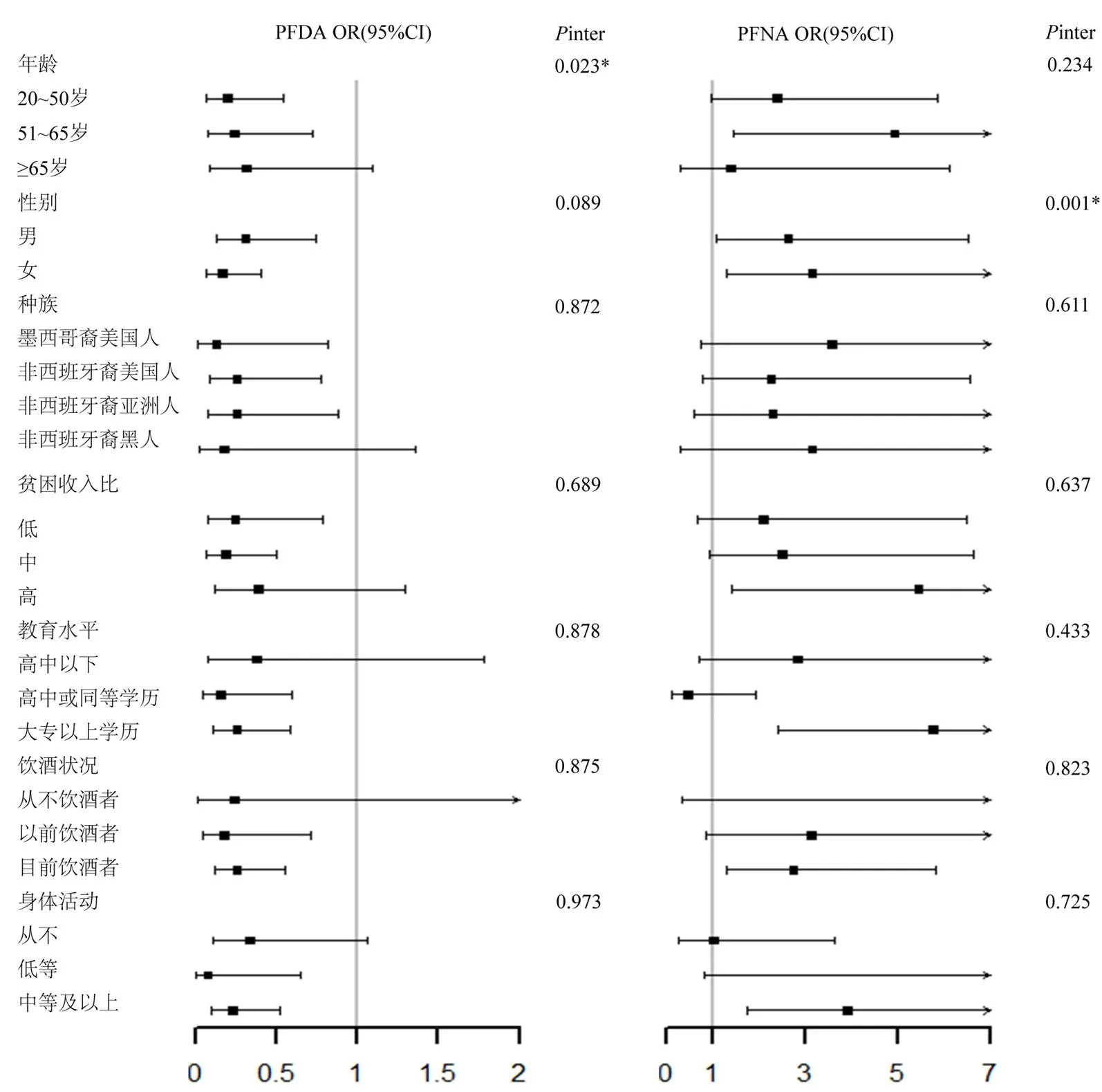
圖1 不同亞組人群血清PFDA、PFNA與MAFLD患病風險的關聯
*表示交互作用有顯著相關性
3 討論
本研究首次評估了美國成年人中多種血清PFAS與MAFLD患病風險的關系.單污染模型顯示,血清PFOS、PFHxS、PFDA與MAFLD患病風險降低相關.多污染模型中血清PFAS沒有顯示一致的關聯性,血清PFNA與MAFLD患病風險呈正向線性劑量反應關系,而血清PFDA與MAFLD患病風險呈負向線性劑量反應關系.
3.1 PFAS對MAFLD患病風險的影響
目前沒有研究直接表明PFAS與MAFLD發生的潛在關聯,只有少數流行病學研究報道PFAS有肝臟損傷以及增加代謝紊亂的風險.同樣基于NHANES數據庫,Gleason等探討了四種PFAS (PFHxS、PFOS、PFOA和 PFNA)與肝功能標志物的關系,發現谷丙轉氨酶隨著血清PFNA水平增加而增加[33],說明PFNA對肝臟有損傷作用.此外在美國俄亥俄州200名成年人的報告中,同樣觀察到PFNA與細胞角蛋白-18(一種脂肪肝生物標志物)存在正相關[34].研究顯示,PFAS 暴露與血液中脂質譜的改變有關,如甘油三酯、膽固醇、低密度脂蛋白升高和高密度脂蛋白降低[35-38].由于PFAS更容易引起肥胖人群血脂異常,并且 MAFLD 與肥胖密切相關,這在一定程度上說明PFAS暴露可能與MAFLD患病風險存在潛在關聯.此外,MAFLD是代謝綜合征的肝臟表現[39],Christense等[9]的研究發現PFNA始終與代謝綜合征及其組分的風險增加相關,而PFDA呈現出與代謝綜合征風險降低有關,這暗示了PFNA可能與MAFLD的風險增加有關系,而PFDA的保護性作用也與本研究結果一致.
動物實驗中,有研究報道PFAS會導致大鼠和非人靈長類動物的肝臟脂質代謝異常、肝臟腫大[40],從而誘發非酒精性脂肪性肝病,可能機制是通過激活PPAR-a誘導脂肪酸b氧化導致肝脂肪積累[41]和氧化應激[42],激活的PPAR-a上調參與調節脂肪酸和膽固醇的運輸與代謝以及炎癥反應的PPAR-a靶基因,并與其上游的過氧化物酶體增殖物反應原件結合[43].此外,PPAR-a在PFDA誘導的肝毒性中有破壞和保護雙重作用[44].PPAR-a功能在人與動物之間存在差異,因此需進一步研究來闡明人血清PFAS在MAFLD發展中的具體機制.
3.2 女性和中老年人的易感性較高
不同性別人群中PFNA相關的MAFLD風險存在差異.女性對PFAS的敏感性較高,與其他結果相似[45],這可能與男性和女性PFAS的不同毒代動力學有關[46].此外,中老年人群中血清PFDA與MAFLD患病風險相關相關效應更為強烈,考慮與中老年人生理功能衰退,對污染物的敏感性升高有關.
3.3 局限性
本研究的局限性:第一,基于橫斷面研究,因果關系的證據并不充分;第二,數據來自NHANES數據庫,外推性受限,需在其他人群中進行驗證;第三,由于 NHANES 2017~2018數據集的限制,缺乏涉及代謝風險異常的部分MAFLD診斷參數,例如負荷后2小時血糖水平和糖尿病類型,這可能會低估MAFLD患病率;第四,因研究條件的局限性,未排除職業、高脂肪飲食以及低水果和蔬菜攝入量等因素,可能導致效應估計有偏差.
4 結論
4.1 與最低四分位數濃度(Q1)相比,血清 PFNA濃度處于Q2、Q3、Q4水平時,患MAFLD風險分別增加62%、62%、172%,且限制性立方樣條分析呈正向線性劑量-反應關系(overall=0.002),表明PFNA暴露是MAFLD發生的重要危險因素.
4.2 與最低四分位數濃度(Q1)相比,血清PFDA處于Q2、Q3、Q4水平時,可導致MAFLD風險分別減少39%、46%、74%,限制性立方樣條分析呈負向線性劑量-反應關系(overall<0.001),表明PFDA暴露是MAFLD發生的重要保護因素.
4.3 亞組分析提示PFDA與年齡亞組存在顯著交互作用(inter=0.023),PFNA與性別亞組存在顯著交互作用(inter=0.001).其中,女性、中老年人群分別是PFNA效應與PFDA效應的易感人群.
[1] Lindstrom A B, Strynar M J, Libelo E L. Polyfluorinated compounds: Past, present, and future [J]. Environmental Science & Technology, 2011,45(19):7954-61.
[2] Kotthoff M, Müller J, Jürling H, et al. Perfluoroalkyl and polyfluoroalkyl substances in consumer products [J]. Environmental Science and Pollution Research, 2015,22(19):14546-59.
[3] Worley R R, Moore S M, Tierney B C, et al. Per- and polyfluoroalkyl substances in human serum and urine samples from a residentially exposed community [J]. Environ. Int., 2017,106:135-43.
[4] Pérez F, Nadal M, Navarro-Ortega A, et al. Accumulation of perfluoroalkyl substances in human tissues [J]. Environ. Int., 2013,59: 354-62.
[5] Sunderland E M, Hu X C, Dassuncao C, et al. A review of the pathways of human exposure to poly- and perfluoroalkyl substances (PFASs) and present understanding of health effects [J]. J. Expo. Sci. Environ. Epidemiol., 2019,29(2):131-47.
[6] Barry V, Winquist A, Steenland K. Perfluorooctanoic Acid (PFOA) exposures and incident cancers among adults living near a chemical plant [J]. Environmental Health Perspectives, 2013,121(11/12): 1313-1318.
[7] Dzierlenga M W, Allen B C, Clewell H J, III, et al. Pharmacokinetic bias analysis of an association between clinical thyroid disease and two perfluoroalkyl substances [J]. Environ. Int., 2020,141:105784.
[8] DeWitt J C, Peden-Adams M M, Keller J M, et al. Immunotoxicity of perfluorinated compounds: recent developments [J]. Toxicol. Pathol., 2012,40(2):300-311.
[9] Christensen K Y, Raymond M, Meiman J. Perfluoroalkyl substances and metabolic syndrome [J]. International Journal of Hygiene and Environmental Health, 2019,222(1):147-153.
[10] Attanasio R. Association between perfluoroalkyl acids and liver function: Data on sex differences in adolescents [J]. Data in Brief, 2019,27:104618.
[11] Eslam M, Newsome P N, Sarin S K, et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement [J]. Journal of Hepatology, 2020,73(1): 202-209.
[12] Zheng K I, Fan J G, Shi J P, et al. From NAFLD to MAFLD: a "redefining" moment for fatty liver disease [J]. Chin. Med. J. (Engl), 2020,133(19):2271-2283.
[13] Zheng K I, Sun D Q, Jin Y, et al. Clinical utility of the MAFLD definition [J]. J Hepatol, 2021,74(4):989-991.
[14] Chan K E, Koh T J L, Tang A S P, et al. Global prevalence and clinical characteristics of metabolic-associated fatty liver disease: A meta- analysis and systematic review of 10 739 607individuals [J]. The Journal of Clinical Endocrinology & Metabolism, 2022,107(9):2691- 2700.
[15] Zhang Y-T, Zeeshan M, Su F, et al. Associations between both legacy and alternative per- and polyfluoroalkyl substances and glucose-homeostasis: The Isomers of C8health project in China [J]. Environment International, 2022,158:106913.
[16] Zeeshan M, Zhang Y-T, Yu S, et al. Exposure to isomers of per- and polyfluoroalkyl substances increases the risk of diabetes and impairs glucose-homeostasis in Chinese adults: Isomers of C8 health project [J]. Chemosphere, 2021,278:130486.
[17] Han X, Meng L, Zhang G, et al. Exposure to novel and legacy per- and polyfluoroalkyl substances (PFASs) and associations with type 2diabetes: A case-control study in East China [J]. Environment International, 2021,156:106637.
[18] Duan Y, Sun H, Yao Y, et al. Serum concentrations of per-/ polyfluoroalkyl substances and risk of type 2diabetes: A case-control study [J]. Science of the Total Environment, 2021,787:147476.
[19] Yang Q, Guo X, Sun P, et al. Association of serum levels of perfluoroalkyl substances (PFASs) with the metabolic syndrome (MetS) in Chinese male adults: A cross-sectional study [J]. Science of the Total Environment, 2018,621:1542-1549.
[20] Jeddi M Z, Dalla Zuanna T, Barbieri G, et al. Associations of perfluoroalkyl substances with prevalence of metabolic syndrome in highly exposed young adult community residents-A cross- sectional study in Veneto Region, Italy [J]. International Journal of Environmental Research and Public Health, 2021,18(3):1194.
[21] Liu H-S, Wen L-L, Chu P-L, et al. Association among total serum isomers of perfluorinated chemicals, glucose homeostasis, lipid profiles, serum protein and metabolic syndrome in adults: NHANES, 2013~2014 [J]. Environmental Pollution, 2018,232:73-79.
[22] Su T-C, Kuo C-C, Hwang J-J, et al. Serum perfluorinated chemicals, glucose homeostasis and the risk of diabetes in working-aged Taiwanese adults [J]. Environment International, 2016,88:15-22.
[23] Conway B, Innes K E, Long D. Perfluoroalkyl substances and beta cell deficient diabetes [J]. Journal of Diabetes and Its Complications, 2016,30(6):993-998.
[24] Jain R B, Ducatman A. Selective associations of recent low concentrations of perfluoroalkyl substances with liver function biomarkers: NHANES 2011to 2014 data on US adults aged320years [J]. J Occup Environ Med, 2019,61(4):293-302.
[25] Attanasio R. Sex differences in the association between perfluoroalkyl acids and liver function in US adolescents: Analyses of NHANES 2013~2016 [J]. Environmental Pollution, 2019,254(PtB):113061.
[26] Chen Y-l, Li H, Li S, et al. Prevalence of and risk factors for metabolic associated fatty liver disease in an urban population in China: a cross-sectional comparative study [J]. BMC Gastroenterology, 2021,21(1):212.
[27] Das K P, Wood C R, Lin M T, et al. Perfluoroalkyl acids-induced liver steatosis: Effects on genes controlling lipid homeostasis [J]. Toxicology, 2017,378:37-52.
[28] Zhang L, Ren X M, Guo L H. Structure-based investigation on the interaction of perfluorinated compounds with human liver fatty acid binding protein [J]. Environ Sci Technol, 2013,47(19):11293-11301.
[29] Foreman J E, Chang S-C, Ehresman D J, et al. Differential hepatic effects of perfluorobutyrate mediated by mouse and human PPAR-alpha [J]. Toxicological Sciences, 2009,110(1):204-211.
[30] Eddowes P J, Sasso M, Allison M, et al. Accuracy of FibroScan controlled attenuation parameter and liver stiffness measurement in assessing steatosis and fibrosis in patients with nonalcoholic fatty liver disease [J]. Gastroenterology, 2019,156(6):1717-1730.
[31] Classification and diagnosis of diabetes: Standards of medical care in diabetes-2021 [J]. Diabetes Care, 2021,44(Suppl 1):S15-S33.
[32] Guo B, Guo Y, Nima Q, et al. Exposure to air pollution is associated with an increased risk of metabolic dysfunction-associated fatty liver disease [J]. Journal of Hepatology, 2022,76(3):518-525.
[33] Gleason J A, Post G B, Fagliano J A. Associations of perfluorinated chemical serum concentrations and biomarkers of liver function and uric acid in the US population (NHANES), 2007~2010 [J]. Environmental Research, 2015,136:8-14.
[34] John, Bassler, Alan, et al. Environmental perfluoroalkyl acid exposures are associated with liver disease characterized by apoptosis and altered serum adipocytokines [J]. Environmental pollution (Barking, Essex: 1987), 2019:247:1055-1063.
[35] Lin T-W, Chen M-K, Lin C-C, et al. Association between exposure to perfluoroalkyl substances and metabolic syndrome and related outcomes among older residents living near a Science Park in Taiwan [J]. International Journal of Hygiene and Environmental Health, 2020,230:113607.
[36] Spratlen M J, Perera F P, Lederman S A, et al. The association between perfluoroalkyl substances and lipids in cord blood [J]. Journal of Clinical Endocrinology & Metabolism, 2020,105(1):43-54.
[37] Jain R B, Ducatman A. Roles of gender and obesity in defining correlations between perfluoroalkyl substances and lipid/lipoproteins [J]. Science of the Total Environment, 2019,653:74-81.
[38] Christensen K Y, Raymond M, Meiman J. Perfluoroalkyl substances and metabolic syndrome [J]. Int. J. Hyg. Environ. Health, 2019,222(1): 147-153.
[39] Kim C H, Younossi Z M. Nonalcoholic fatty liver disease: a manifestation of the metabolic syndrome [J]. Cleve Clin J Med, 2008, 75(10):721-728.
[40] Lau C, Anitole K, Hodes C, et al. Perfluoroalkyl acids: a review of monitoring and toxicological findings [J]. Toxicol. Sci., 2007,99(2): 366-394.
[41] Wan H T, Zhao Y G, Wei X, et al. PFOS-induced hepatic steatosis, the mechanistic actions on β-oxidation and lipid transport [J]. Biochim. Biophys. Acta, 2012,1820(7):1092-101.
[42] Khansari M R, Yousefsani B S, Kobarfard F, et al. In vitro toxicity of perfluorooctane sulfonate on rat liver hepatocytes: probability of distructive binding to CYP 2E1and involvement of cellular proteolysis [J]. Environ. Sci. Pollut. Res. Int., 2017,24(29):23382-8.
[43] Feige J N, Gelman L, Michalik L, et al. From molecular action to physiological outputs: Peroxisome proliferator-activated receptors are nuclear receptors at the crossroads of key cellular functions [J]. Progress in Lipid Research, 2006,45(2):120-59.
[44] Luo M, Tan Z, Dai M, et al. Dual action of peroxisome proliferator- activated receptor alpha in perfluorodecanoic acid-induced hepatotoxicity [J]. Archive für Toxikologie, 2016,91(2):1-11.
[45] Sen P, Qadri S, Luukkonen P K, et al. Exposure to environmental contaminants is associated with altered hepatic lipid metabolism in non-alcoholic fatty liver disease [J]. Journal of Hepatology, 2022, 76(2):283-293.
[46] Harada K, Inoue K, Morikawa A, et al. Renal clearance of perfluorooctane sulfonate and perfluorooctanoate in humans and their species-specific excretion [J]. Environ. Res., 2005,99(2):253-261.
Relationship of serum perfluoroalkyl substances with the risk of metabolic associated fatty liver disease.
ZHANG Lu-lu, LIU Jing, HE Ying-qian, ZHAO Ya-nan, ZHENG Shan, WANG Min-zhen*
(Institute of Epidemiology and Statistics, School of Public Health, Lanzhou University, Lanzhou 73000, China)., 2023,43(2):964~972
To explore the effect of serum perfluoroalkyl substances (PFAS) on the metabolic-associated fatty liver disease (MAFLD) on the basis of the 2017~2018 US National Health and Nutrition Survey (NHANES) database. The logistic regression model and restricted cubic spline (RCS) were used to evaluate the association and dose-response relationship between PFAS and MAFLD. The main results showed that in a single pollutant model, perfluorooctane sulfonic acid (PFOS), perfluorohexane sulfonic acid (PFHxS) and perfluorodecanoic acid (PFDA) were negatively associated with the risk of MAFLD, with the ORs of 0.64 (95%CI:0.45~0.91), 0.65 (95%CI:0.46~0.93) and 0.45 (95%CI:0.30~0.67), respectively. In the multi-pollutant model, compared with the lowest quantile (Q1), the risk of MAFLD increased with the increase of perfluoronanoic acid (PFNA) by 62% (OR=1.62, 95%CI:1.10~2.39), 62% (OR=1.62, 95%CI:1.01~2.60) and 172% (OR=2.72, 95%CI: 1.53~4.84) at Q2, Q3, and Q4, respectively. Conversely, there was negative linear dose-response relationship (overall<0.001) between PFDA and the risk of MAFLD. The risk of MAFLD were 0.61(95%CI: 0.44~0.85), 0.54(95%CI: 0.34~0.84) and 0.26(95%CI: 0.15~0.45) when the concentration of PFDA reached to Q2, Q3, and Q4 levels. Subgroup analysis showed that serum PFDA had a more significant effect on the risk of MAFLD in 51~65 years old population. Females exposed to serum PFNA were more likely to develop MAFLD. In conclusion, serum PFNA and PFDA were significantly related to the risk of MAFLD, and PFNA exposure played a risky role in the occurrence of MAFLD while PFDA had protective effect. Women, middle-aged and elderly people might be potential susceptible groups.
perfluoroalkyl substances;metabolic associated fatty liver disease;dose-response relationship
X503.1;X18
A
1000-6923(2023)02-0964-09
張露露(1998-),女,江西南昌人,蘭州大學碩士研究生,主要從事環境流行病學研究.
2022-07-06
國家自然科學基金資助項目(41705122)
* 責任作者, 副教授, wangmzh@lzu.edu.cn
猜你喜歡
童話王國·奇妙邏輯推理(2024年5期)2024-06-19 16:03:38
課堂內外·初中版(科學少年)(2023年10期)2023-12-10 00:43:06
全科護理(2022年10期)2022-12-26 21:19:15
中老年保健(2021年3期)2021-08-22 06:50:04
天津醫科大學學報(2021年2期)2021-03-29 05:31:08
國際放射醫學核醫學雜志(2021年10期)2021-02-28 08:41:58
現代臨床醫學(2021年1期)2021-01-26 00:56:02
中學生數理化·七年級數學人教版(2020年10期)2020-11-26 08:24:50
數學物理學報(2020年2期)2020-06-02 11:29:24
光學精密工程(2016年6期)2016-11-07 09:07:19