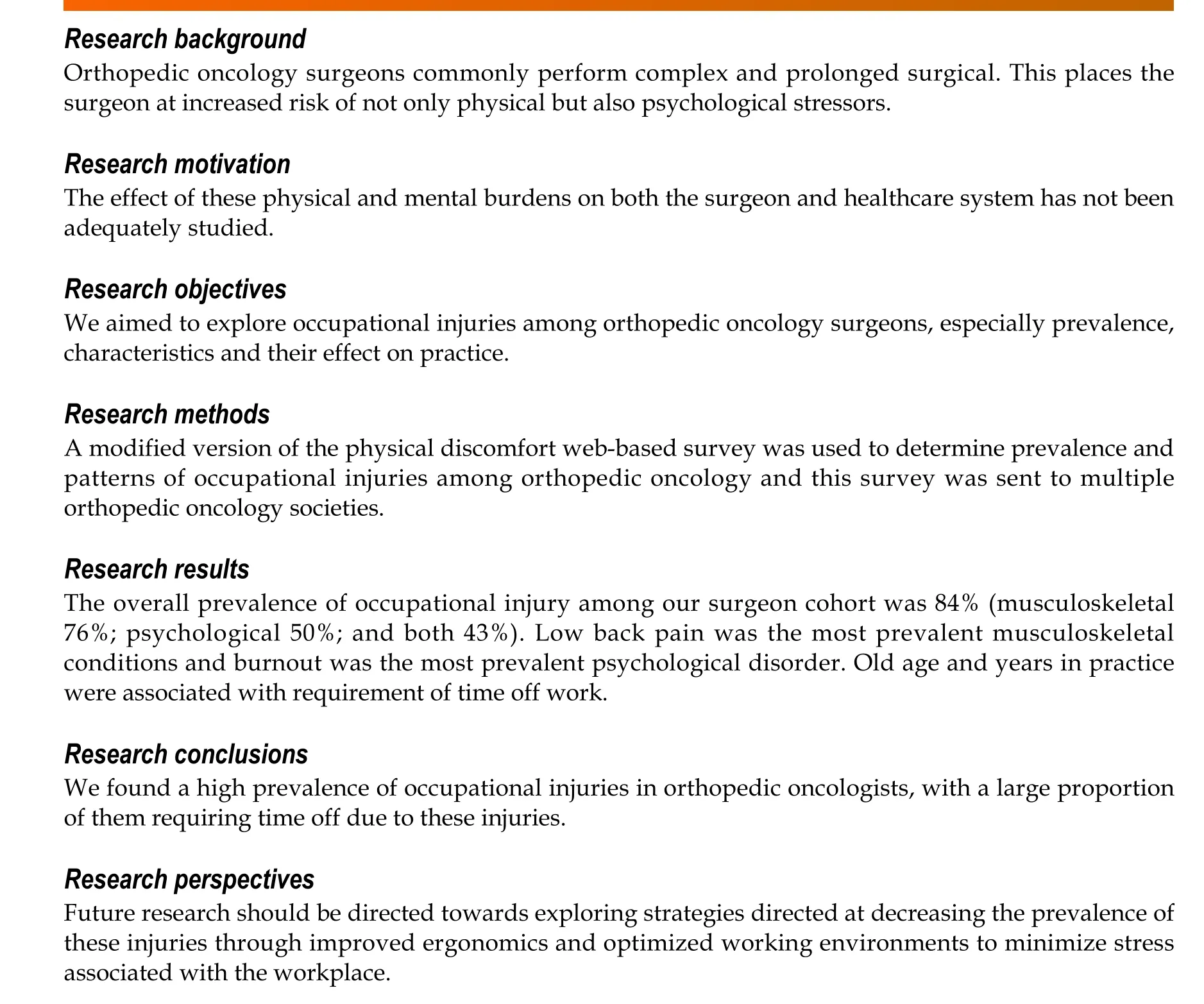
Occupational injuries and burn out among orthopedic oncology surgeons
2022-12-29 07:21:58AbdulrahmanAlaseemRobertETurcotteNathalieSteMarieMohammadAlzahraniSaadAlqahtaniKristaGoulding
World Journal of Orthopedics
2022年12期
關(guān)鍵詞:網(wǎng)絡平臺
Abdulrahman M Alaseem, Robert ETurcotte, Nathalie Ste-Marie, Mohammad M Alzahrani,Saad M Alqahtani,Krista A Goulding
Abstract
Key Words: Orthopedic oncology; Surgeons; Occupational; Musculoskeletal; Injuries.
lNTRODUCTlON
Alarming rates of occupational injuries have been previously reported in different surgical fields including orthopedic surgery[1-5]. It has been an area of interest and investigation due to the implications of these injuries on surgeons, health care system and the quality of provided care[6-9]. Occupational injuries are either work-related injuries or illnesses caused by incidents at a workplace or previous illnesses aggravated by work-related injuries, that could negatively impact the well-being of the affected workers or the quality of provided care[10-12]. Orthopedic surgeons are more vulnerable to a variety of work-related injuries and hazards associated with the nature of their profession such as blood born infections, sharp injuries, noise-induced hearing impairment, exposure to radiation and chemicals, heavy physical workload, emotional and psychological disturbances[13-16].
Several studies have suggested that orthopedic surgeons are at increased rates of occupational injuries[17-20]. When compared to general surgeons, orthopedic surgeons were found to have higher rates of subjective physical injuries. The most reported injuries were back pain, neck pain and upper extremity related complaints[15,21,22]. Furthermore, the psychological disturbances including burnout rates, were found to be higher among orthopedic surgeons as compared to other medical professions and the general population, which in turn may negatively impact the quality of patient care due to increased medical errors and depersonalization[10,23].
Orthopedic oncology is a subspecialty of orthopedics that is physically and psychologically challenging as it involves prolonged and complex surgical procedures, as well as higher rates of serious surgical complications and limited survivorship and functional outcome relating to the oncology patient population. Consequently, such physical and psychological stressors may subject orthopedic oncology surgeons to higher rates of work-related “occupational” injuries that can impact their quality of life, wellness and the quality of delivered patient care. These occupational stressors can lead to preventable musculoskeletal injuries, time off work, increased burnout rates, emotional and psychological disturbances. Investigating this aspect among orthopedic oncology surgeons can help institutions and occupational health agencies to develop preventive strategies to minimize the negative implications of these injuries on the quality of provided care and promote surgeons’ personal well-being.
To our knowledge, there are no studies to date investigating the occupational injuries among orthopedic oncology surgeons. The aim of this survey is to explore occupational injuries in orthopedic oncologists, including their prevalence and characteristics.
MATERlALS AND METHODS
An anonymous online, web-based, modified version of the Physical Discomfort Survey (originally developed by the Workplace Safety and Health Division of Manitoba, Canada)[24] and modified version of Maslach Burnout Inventory-Human services survey for medical personnel[25] was emailed to all surgeon members of Musculoskeletal Tumor Society (MSTS), Canadian Orthopedic Oncology Society (CANOOS), and European Musculoskeletal Oncology Society (EMSOS). Only practicing orthopedic oncology surgeon members of the above-mentioned societies were eligible to participate in our study. The first invitation email was sent out in November 2016 and a reminder email was sent out in January 2017. The survey was closed by mid-February 2017. To minimize the magnitude of potential selection and response biases, we sent our survey to all surgeon members of three large orthopedic oncology societies in North America and Europe. Furthermore, we attempted to reduce the potential response bias by sending a subsequent reminder email.
The survey was divided into 3 parts, the first part included questions about participant’s demographic data (age, gender, hand dominance), practice setting (academic, community or private), practice duration in years and the average operative caseloadperyear. The second part of the survey was about the musculoskeletal complaints by region (neck, lower back, upper extremity and lower extremity). For each question, participants were asked about the diagnosis, medical or surgical treatments (if any) and if they ever required work stoppage consequently. The third part of the survey involved questions concerning psychological disturbances (anxiety, depression, insomnia, suicidal thoughts and burnout symptoms) and symptoms of “burnout” (emotional exhaustion, depersonalization, low job satisfaction), treatments required (if any) and any time off work needed as a result.
Descriptive statistics were used to report participants’ demographics. The prevalence of occupational injury was estimated as the number of injuriespertotal number of respondents. To determine significant associations between patient demographics and occupational hazards, we performed classical tests of hypothesis as well as logistic regression analysis. Statistical significance was set at an alpha of 0.05 and analysis was carried out using Stata v12.1 (Statacrop).
RESULTS
Sixty-seven orthopedic oncology surgeons (58 male and 9 female surgeons) completed the survey (22% response rate). Of the respondent, 40.3%, 43.3% and 6% of respondents were from MSTS, EMSOS and CANOOS, respectively. Most of the participant surgeons are practicing in academic setting (83.3%). The oncologic yearly caseload was seventy-five cases or more in 38.8% of the surgeons.
Eighty four percent of surveyed orthopedic oncology surgeons reported an occupational injury. Musculoskeletal injuries were reported by 76% of participating surgeons, psychological injuries by 50% and both by 43%. The most common musculoskeletal injuries were low back pain (39%), shoulder symptoms (27%), neck pain (24%), lumbar disc herniation (16%), shoulder tendinitis (15%), lateral epicondylitis (13%), hip or knee osteoarthritis and varicose veins (10 % each) (Figure 1). Consequently, time off work was reported by 33.3% surgeons and 27% required treatment including either medical or surgical treatment. Exacerbation of musculoskeletal injuries was experienced by 18% of respondents (Table 1).
Thirty-three surgeons reported a psychological disturbance (50%). The most prevalent were burnout (27%), anxiety and insomnia (20% each) and depression (11%). More seriously, suicidal thought was reported by one participant (Figure 2). Medical and/or psychiatric treatment was required by 18% of respondents and the time off work was required by 3% (Table 2). Young age (35-45 years) was the only significant factor associated with developing symptoms of burnout (P< 0.015).
Eighteen surgeons (26.9%) required time off work due to occupational injuries (17 musculoskeletal injuries and 1 psychological disturbance). Factors significantly associated with time off work were age and years of practice of the surgeon (P< 0.011) in the logistic regression analysis models performed.
DlSCUSSlON
Our study revealed a concerning prevalence of occupational injuries among orthopedic oncology surgeons (84%), which is much higher than the previously reported rates in other orthopedic subspecialties[11,17-20]. This could lead to consequences not only on the surgeon’s career, but also on the quality and cost of provided health care. One third (33.3%) of participating surgeons reported periods of work stoppage due to work-related injuries and 27% required either medical or surgical treatments. Fifty percent of respondents reported symptoms of occupational psychological disturbances, with burnout being the most reported (27%) followed by insomnia and anxiety (20% each). Orthopedic surgeons in general have higher work-related subjective musculoskeletal symptoms when compared to general surgeons[15]. However, orthopedic oncology is a unique field in orthopedics which deals with complex osseous and soft tissue tumors and therefore, orthopedic oncologists are involved in prolonged meticulous surgical procedures with relatively higher complication rates than any other orthopedic specialties. Furthermore, Orthopedic oncologists face psychological stressors as they are involved in psychological and emotional aspects associated with the management of oncology patients. Hence, it is not surprising that this surgeon population have higher rates of occupational injuries including musculoskeletal and psychological disturbances as shown in the results of this study.
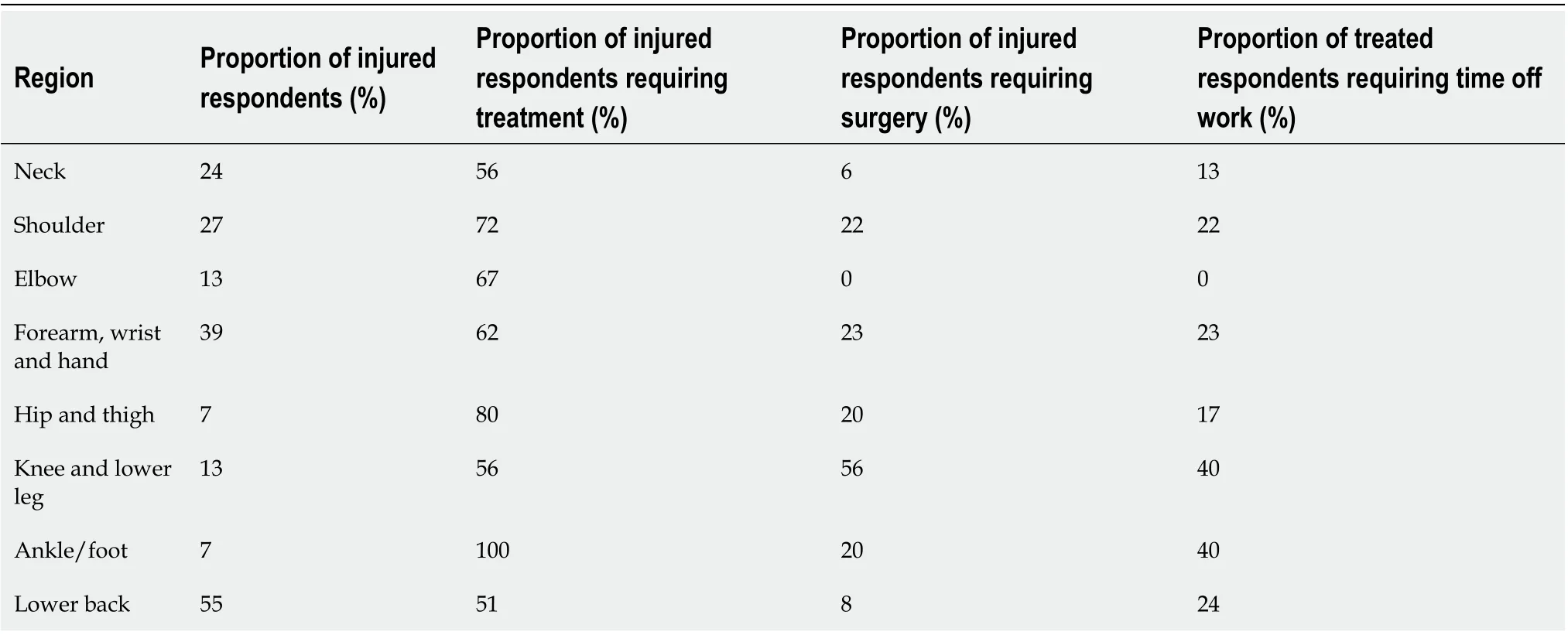
Table 1 Proportion of orthopaedic oncologists’ surgeons with diagnosed musculoskeletal disorders per region requiring treatment and time off work
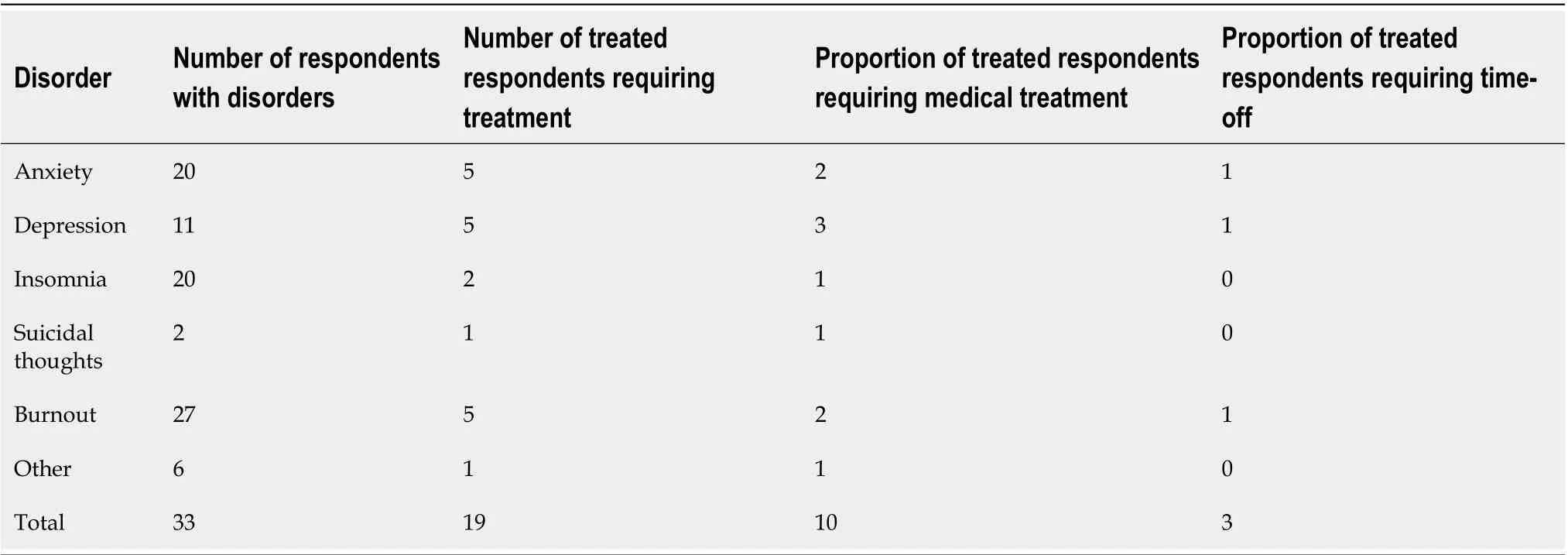
Table 2 Proportion of orthopaedic oncologists’ surgeons with diagnosed psychological disorders requiring treatment and time off work
Several factors have been shown in the literature as contributing factors to the high rates of occupational injuries among surgeons[4-8]. The nature of their work involves poor ergonomics such as lengthy non-neutral postures while operating, repetitive intra-operative physically demanding tasks, the height of operating table and the non-ergonomically designed surgical instruments[5-8]. New ergonomic innovations have been suggested to improve the operating room environment and minimize the risks of occupational injuries; however, the utilization of these devices is not yet popularized. These factors are applicable even more to orthopedic oncologists due to the complexity and nature of their profession. However, if such work-related injuries are not addressed early, it may progress to more sever morbidity and adversely influence the surgeon’s wellbeing and career lifespan.
In addition, psychological disturbances were also found to be high in surgeons, especially in surgical oncologists in the current literature[26]. This is consistent with our results showing high psychological morbidity rates among orthopedic oncologists. Nevertheless, many surgeons may neglect their occupational health issues and thus not pursue the appropriate help when needed, likely due to lack of mindfulness about the potential occupational health injuries and the heavy workload nature of their professions[8].
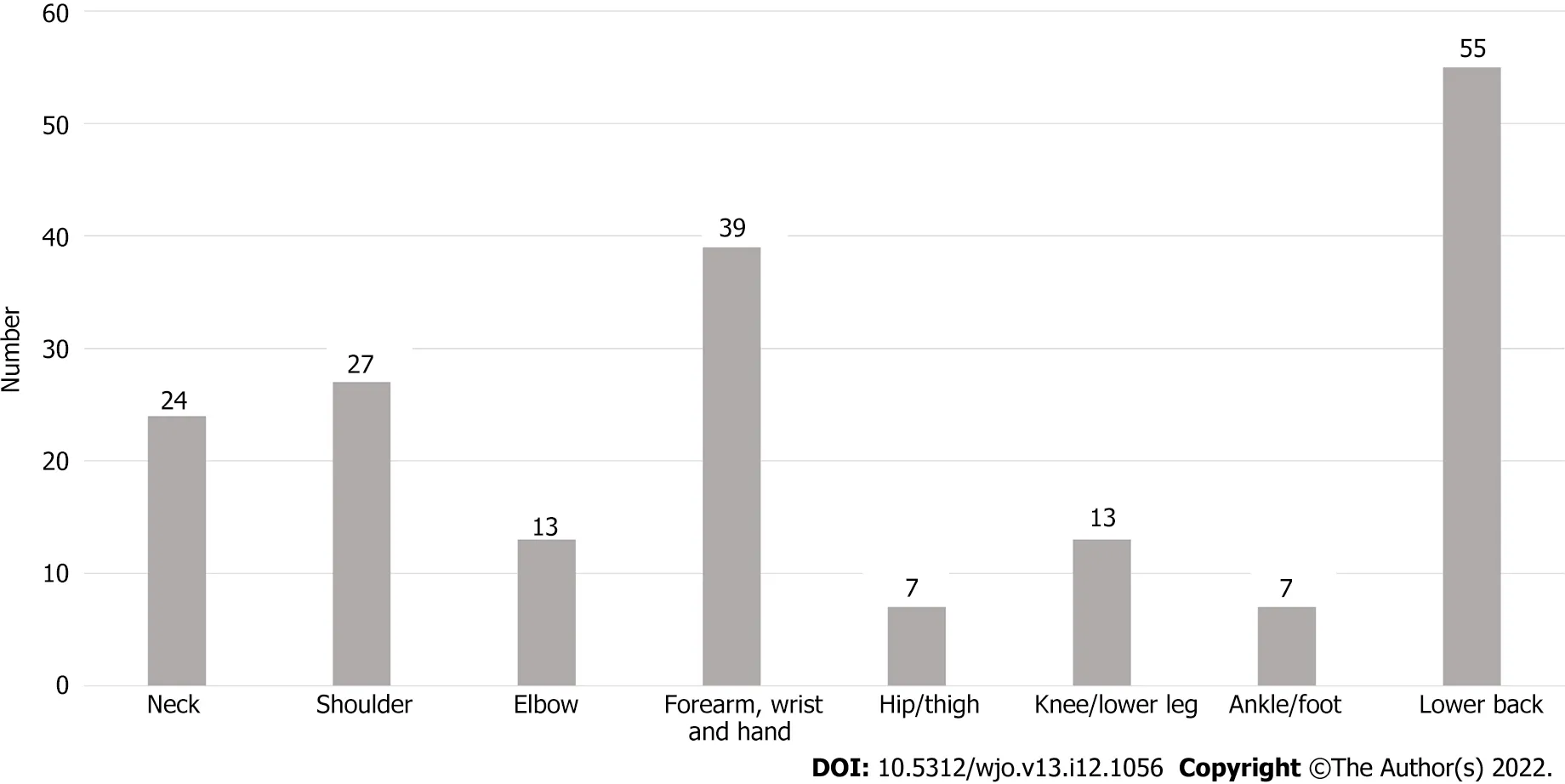
Figure 1 Percentages of reported musculoskeletal disorders and complaints among survey participants.
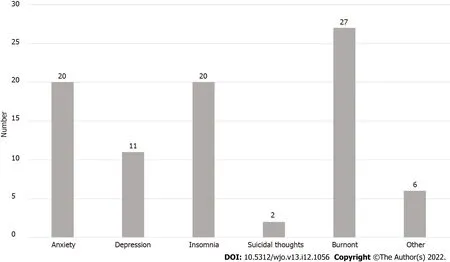
Figure 2 Percentages of reported psychological disorders among survey participants.
The limitations of our survey study are similar to most survey studies in the literature. One of the limitations is the subjective nature of self-reported occupational musculoskeletal and psychological complaints. However, our participants are practicing surgeons and most likely they are accurately reporting their health issues. Additionally, the primary focus of our study is to assess the magnitude of occupational injuries among orthopedic oncologist and the characteristics of these injuries. Most workrelated symptoms are subjective complaints and may not be associated with objective clinical findings. Therefore, it is widely accepted to evaluate the prevalence of occupational injuries by self-administered surveys. Another possible argument is the significantly higher prevalence rate of occupational injuries reported in our study. This possibly inflated prevalence could be related to that some participants in such surveys are currently or have previously been affected by occupational injuries, thus probably leading to possible response or selection bias. Although we believe this is certainly a valid concern, we still anticipate a high rate of occupational injuries among orthopedic oncologists if we assume the nonrespondents are not affected with occupational injuries. The surveys used in our current study included modified self-reported outcomes, which could be an area of limitation. Future research should be directed at studying the reliability, validity, and area of weaknesses of these surveys. One of the strengths of our study is that the study sample, although relatively small, is representative of the orthopedic oncology surgeons’ population in North America and Europe, which is considered not a large population.
實施欺凌行為的性別差異方面,男生在“對他人實施毆打、推搡等肢體暴力行為”和“脅迫他人或勒索財物”以及“嘲笑、取綽號、惡意評論過他人的生理特征等”三個行為方面顯著高于女生,而在“言語辱罵、當面或背地里說壞話”、“在網(wǎng)絡平臺惡意中傷他人、散播他人隱私、謠言等”、“故意孤立、排擠他人”方面,男生與女生之間并無顯著差異。
CONCLUSlON
The purpose of this survey was to increases the mindfulness of work-related health issues and its possible consequences on surgeons’ wellness, patient care delivery and institutional health quality measures. Our data should help health institutions and occupational health services develop early educational programs directed to surgeons and provide preventive and supportive ergonomic measures in order to improve the surgeons’ wellness and minimize the undesirable consequences of occupational injuries on the health care system.
ARTlCLE HlGHLlGHTS
FOOTNOTES
Author contributions:Alaseem AM, Turcotte RE, Alzahrani MM, Al-Qahtani SM, Goulding KA contribute to study design; Alaseem AM, Turcotte RE, Ste-Marie N, Alzahrani MM, Al-Qahtani SM, Goulding KA contribute to manuscript preparation; Turcotte RE, Alzahrani MM, Al-Qahtani SM, Goulding KA contribute to methodology; Ste-Marie N contribute tostatistical analysis.
lnstitutional review board statement:This was a survey study and institutional review board was not required for this study.
lnformed consent statement:This study is a survey and informed consent was not required.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:Raw data and material are available as needed.
STROBE statement:The authors have read the STROBE Statement-checklist of items, and the manuscript was prepared and revised according to the STROBE Statement-checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Canada
ORClD number:Mohammad M Alzahrani 0000-0003-1299-1529; Saad M Alqahtani 0000-0002-9925-2480.
S-Editor:Liu GL
L-Editor:A
P-Editor:Liu GL
登錄APP查看全文
猜你喜歡
甘肅教育(2021年12期)2021-11-02 06:30:06
裝備制造技術(shù)(2021年1期)2021-05-21 07:55:08
福建基礎教育研究(2019年6期)2019-05-28 17:48:32
石油化工自動化(2018年5期)2018-11-14 02:34:18
人大建設(2017年11期)2017-04-20 08:22:46
長春中醫(yī)藥大學學報(2017年1期)2017-04-16 05:56:52
學周刊(2016年23期)2016-09-08 08:56:58
新疆醫(yī)科大學學報(2015年10期)2015-12-26 12:33:32
衛(wèi)生職業(yè)教育(2014年20期)2014-05-16 03:17:38
中國工程咨詢(2012年12期)2012-02-13 02:46:38
 World Journal of Orthopedics
2022年12期
World Journal of Orthopedics
2022年12期
- World Journal of Orthopedics的其它文章
- Wooden foreign body impalement through the right shoulder region - an unusual penetrating injury: A case report
- Taper-wedge stem suitable for anterior approach total hip arthroplasty: Adequate biomechanical reconstruction parameters and excellent clinical outcome at mid-term follow-up
- Accuracy of the rotator cuff reparability score