Comparison of intravitreal aflibercept and dexamethasone implant in the treatment of macular edema associated with diabetic retinopathy or retinal vein occlusion: a Meta-analysis and systematic review
2022-09-14 06:37:16XuanYuQiuXiaoFeiHuYaZhouQinJiXianMaQiuPingLiuLiQinJingMingLi
INTRODUCTION
Diabetic retinopathy (DR) and retinal vein occlusion(RVO) are the two most common retinal vascular diseases. DR is a common cause of moderate and severe visual impairment in working-age population. At present,there are 92.6 million DR patients worldwide, of which approximately 20.6 million suffer from diabetic macular edema (DME), and nearly 28.4 million suffer from visual impairment. Its main clinical manifestations include retinal microaneurysm, spot or patchy hemorrhage, cotton wool spots,macular edema (ME),. RVO is the second most common retinal vascular disease. It is estimated that there are 5.2 to 16 cases per 1000 patients with RVO and there are nearly 16 million cases worldwide. Vascular dilation and tortuosity,retinal hemorrhages as well as cystoid macular edema (CME)are the characteristics of RVO. When the retinal vascular changes only affect the peripheral retina, it may not have a significant impact on vision. Once the macular area involved,there will be a significant decrease in vision. ME is a common serious complication of both DR and RVO. Thus, seeking therapeutic strategy for ME have attracted great concern of ophthalmologists and retinal specialists.
Two of the most important pathogenic mechanism of ME are the increased release of vascular endothelial growth factor(VEGF) and the production of pro-inflammatory cytokines.Therefore, anti-VEGF and anti-inflammation are the main treatment regimens for ME. Anti-VEGF agents such as aflibercept have been proved to effectively prevent vision loss and is currently recognized as a preferred treatment for ME.Aflibercept is a recombinant fusion protein consisting of the extracellular domain of human VEGF receptor-1 and 2 fused to the Fc fragment of human IgG1. Previous studies have shown that aflibercept has a significantly greater binding affinity for VEGF than bevacizumab or ranibizumab, and it may last longer in the eye. However, the effects of intraocular anti-VEGF agents can only be sustained for a short period with a single administration. Inflammation plays a pivotal role in the pathophysiology of ME. Thus, corticosteroids have been clinically used in the treatment of ME for years. The sustained dexamethasone intravitreal implant (DEX implant; Ozurdex), a biodegradable device, was first approved by the Food and Drug Administration in 2009 for the treatment of ME with RVO. Its unique dosage form can overcome the ocular administration barrier and prolong the action time of dexamethasone in the eye.In previous studies, both the aflibercept and dexamethasone implant have been shown to be effective in the treatment of ME. They can slow the progression of vision loss in most patients and alleviate ME. However, there have been few systematic reviews or Meta-analyses comparing the clinical efficacy and safety between the aflibercept and dexamethasone implant. Thus, in this context, we conducted this Meta-analysis and systematic review to evaluate the efficacy and safety of aflibercept and dexamethasone for patients with RVO or DR associated ME, including best-corrected visual acuity (BCVA),central retinal thickness (CRT) and other indicators such as number of injections and serious adverse events (SAEs).
納入的50名護士研究數據均以SPSS20.0軟件分析,計量資料以(± s)表示,行t檢驗或方差分析,選取Pearson 法處理護士職業疲憊感、工作壓力源和社會支持之間的關系,P<0.05為差異具有統計學意義。
MATERIALS AND METHODS
根據視頻監控資料及村民描述,事故發生時風向發生過偏轉。這主要是由于強雷暴單體本身是一個移動的逆時針旋轉的低壓系統,在它移動過程中,廊橋處于該強雷暴不同的象限,導致風向發生偏轉。
We screened the article in accordance with the following criteria. 1) The causes of ME include DR and RVO; 2) The final articles should be controlled trial design comparing the efficacy and safety of intravitreal aflibercept with dexamethasone implant in the treatment of ME; 3) There are useful data to be extracted in the final articles including BCVA and CRT; 4) The final selected documents are not time-limited but must be in English; 5) The final article must have 3mo or more follow-up period.
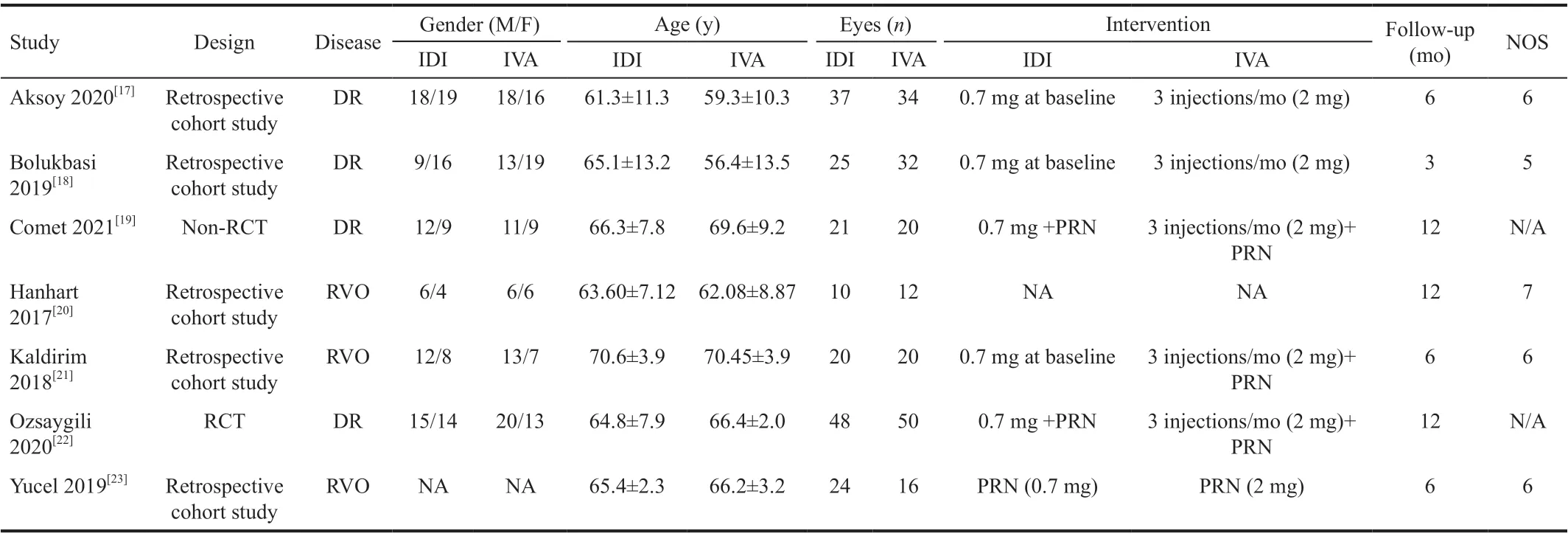
The titles, abstracts,and full texts are screened by two researchers independently using the above selection criteria. The differences of opinions were resolved through discussion. This includes randomized controlled trials (RCTs), real-world prospective and retrospective clinical studies. The following data should be extracted and organized from the final articles: the name of first author, year of publication, the type of study design,key characteristics of subjects (such as: number of research subjects, age, sex, and number of eyes in the study) as well as data of research results (such as: BCVA, CRT, mean number of intravitreal injections, SAEs).
Quality evaluation of RCTs were performed using Revised Cochrane risk of bias tool for individually randomized, parallel group trials (RoB2.0).Methodological Index for Non-randomized Studies (MINORS)were used to perform quality assessment for non-RCTs.Quality of cohort studies were assessed with Newcastle-Ottawa scale (NOS).
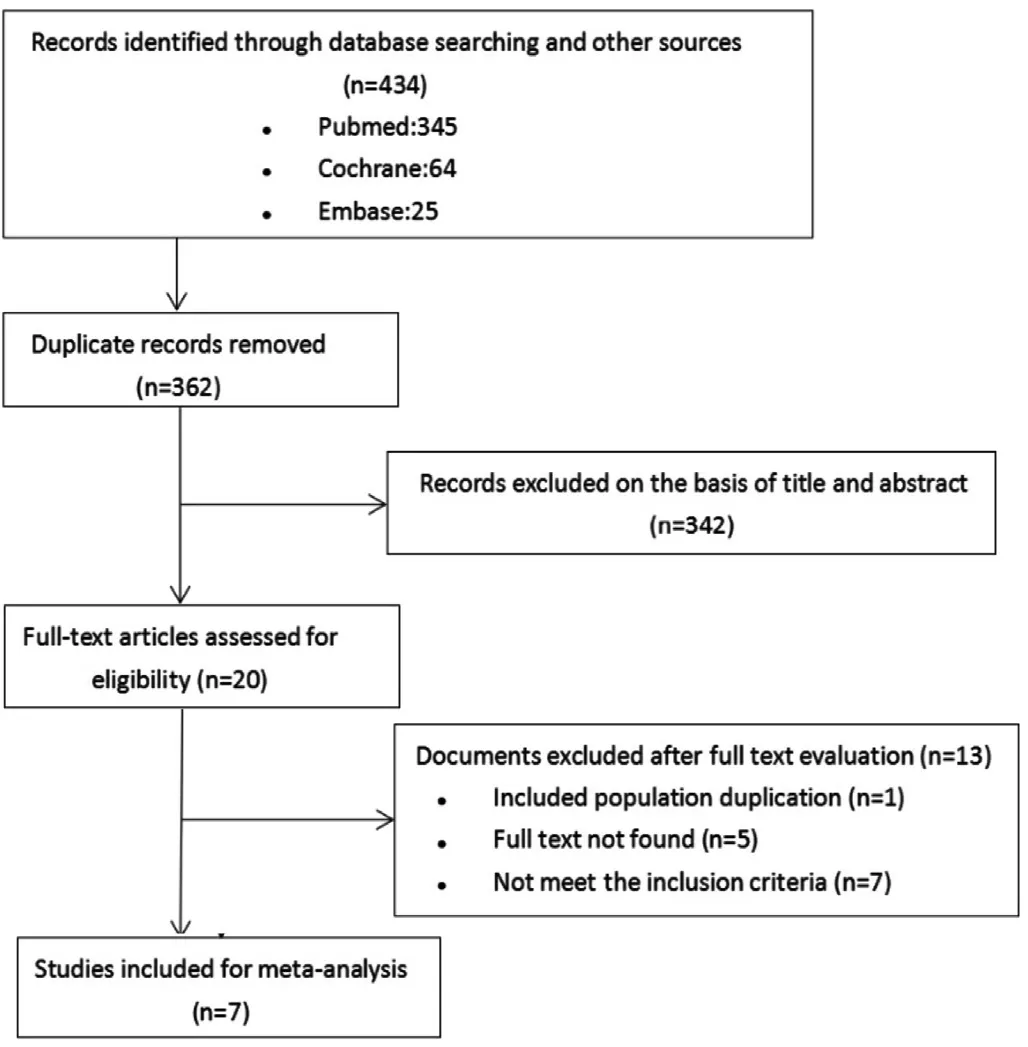
The flow chart of the selection process is shown in Figure 1. In the literature search, 434 studies were identified in PubMed, Cochrane, and Embase. After checking for duplications, 362 studies were left. Of these studies, 20 articles that were relevant to the study topic remained for fulltext review. Finally, after full-text review of these 20 articles, 7 studies met inclusion criteria.
RESULTS
Meta-analysis was performed using RevMan5.3 software. Enumeration data (SAEs) were described by relative risk (RR) and 95% confidence interval(CI), while measurement data including BCVA, CRT, mean number of intravitreal injections were described by mean difference (MD) and 95%CI.test was used for heterogeneity test. If≥0.1 and≤50%, a fixed-effect model would be used for Meta-analysis.<0.1 and>50% indicated statistical heterogeneity among references. In this case, the source of the heterogeneity needs to be analyzed and sensitivity analysis should be performed to detect stability.If there was no clinical heterogeneity, random effects model would be used for Metaanalysis. If there was large heterogeneity and the source of heterogeneity could not be known, descriptive analysis would be used.<0.05 was considered statistically significant.
(1)水體700 nm波段的后向散射系數與總懸浮物濃度和無機懸浮物濃度具有較好的相關性,所構建的指數反演模型具有可行性,因此后射散射儀具備實時監測懸浮物濃度的功能,能夠作為水體組分垂向結構分析的測量手段。
高職院校實訓基地不僅需要滿足在校學生的實踐教學需求,同時也擔負為當地社會經濟發展培養專業人才這一重任。所以高職院校實訓基地建設要盡量考慮這一因素,在建設中要考慮滿足培養當地專業人才所需環境和設備資源,最大限度實現資源的共享,為社會經濟發展做出自己的貢獻。
The change of BCVA is the most important index to observe the therapeutic efficacy. Different studies recorded BCVA in a different way.Among them, logarithm of minimum angle of resolution(logMAR) visual chart was used in 3 studies, Early Treatment Diabetic Retinopathy Study (ETDRS) letters was used in 2 studies, and Snellen visual chart was used in 2 studies. For the purpose of statistical analysis, all visual acuity data were converted into logMAR. To extrapolate all available data,6 studies (=347) were used for the analysis of 3-month outcomes, 4 studies (=219) were used for the analysis of 6-month outcomes and 3 studies (=161) were included for 12-month analysis. After testing the heterogeneity, we all used the fixed effects model (3mo:=0.60,I=0; 6mo:=0.98,I=0; 12mo:=0.96,I=0). The pooled results demonstrated no significant difference in BCVA gain between aflibercept and dexamethasone in either 3mo (MD -0.05; 95%CI -0.11, 0.02;=0.17) or 12mo (MD -0.01; 95%CI -0.38, 0.37;=0.98). But there was a significant difference of BCVA gain at 6mo (MD 0.12; 95%CI 0.03, 0.21;=0.008) between two groups with original data showing slightly worse of dexamethasone than aflibercept for BCVA improvement (Figure 2).
After heterogeneity test, we found there was great heterogeneity among these studies, so the random effects model was used (3mo:<0.01 I=84%; 6mo:<0.01I=92%; 12mo:=0.02I=74%). After comparison between aflibercept and dexamethasone, the two medications had no significant differences in reducing CRT overall (3mo: MD -28.14; 95%CI -79.95, 23.67;=0.29; 6mo:MD 27.67; 95%CI -84.89, 140.24;=0.63; 12mo: MD -59.00;95%CI -127.37, 9.37;=0.09; Figure 3).
Four included articles reported adverse events related to intraocular pressure (IOP).
The results of CRT showed that in terms of anatomic improvement, compared with intravitreal injection of aflibercept, dexamethasone implant was not significantly inferior to aflibercept. The statistical results told us that compared with the intravitreal injection of aflibercept, the dexamethasone implant can effectively reduce the number of injections. Thus, dexamethasone demonstrated its unique advantages including less repeated injection and subsequent better patient compliance. Although dexamethasone is not a prime anti-VEGF drug compared with aflibercept, as a hormone, it can indirectly decrease VEGF expression, stabilize white blood cells, and reduce relief of inflammatory cytokines.Studies have shown that dexamethasone is slightly superior to aflibercept, in both anatomy and function during the first three months of administration. It indicated that in clinical practice,dexamethasone implant may be the first choice for patients with injection anxiety, heavy economic burden, or poor compliance.Statistical results of adverse reactions told us that dexamethasone has similar drawbacks as other steroids. For example, it may increase IOP to some extent and accelerate the progress of cataract. In this Meta-analysis, 25% (5 patients) of the Kald?r?m and Yazgandexamethasone group and 12% (3 patients) of the Bolukbasidexamethasone group used antiglaucoma drugs regularly to control their IOP, and the Hanhart and Rozenmandexamethasone group had elevated IOP without medication control. There was no significant change of IOP in Cometand Aksoydexamethasone groups.Therefore, we can conclude that dexamethasone implant was more likely to cause elevated IOP in patients than aflibercept,but they were manageable.
1932年5月,中野重治的保釋被取消,再一次入獄。此次的入獄比上一次遭受了更為嚴重的迫害,不得已中野重治于1934年向當局表明轉向的意思后得以出獄。但是中野重治并沒有丟掉無產階級作家的心,出獄后,他深入思考自己的屈辱,開始了作為作家的新的戰斗。1937年中野重治和宮本百合子等人收到了禁止執筆的處分。戰爭結束后當年11月,中野重治再入共產黨,作為共產黨員在文學界甚至政界活躍。……
登錄APP查看全文
猜你喜歡
裝備制造技術(2020年12期)2020-05-22 09:25:38
福建教育學院學報(2019年4期)2019-06-12 08:39:10
活力(2019年21期)2019-04-01 12:18:24
計算機測量與控制(2017年6期)2017-07-01 16:23:53
電子制作(2017年8期)2017-06-05 09:36:15
新時代職業教育(2016年4期)2016-02-06 02:15:35
學習月刊(2015年8期)2015-07-09 03:55:40
中國教育技術裝備(2015年6期)2015-03-01 02:36:27
江蘇高職教育(2014年4期)2014-02-28 11:40:57
海峽影藝(2012年1期)2012-11-30 08:15:44
 International Journal of Ophthalmology
2022年9期
International Journal of Ophthalmology
2022年9期
- International Journal of Ophthalmology的其它文章
- What can we learn from negative results in clinical trials for proliferative vitreoretinopathy?
- Suggestions on gut-eye cross-talk: about the chalazion
- A novel mutation of RPGR in a Chinese family with X-linked retinitis pigmentosa
- Novel technique of penetrating keratoplasty in high-risk grafts with significant corneal neovascularization
- COVlD-19 infection with keratitis as the first clinical manifestation
- Corneal histomorphology and electron microscopic observation of R124L mutated corneal dystrophy in a relapsed pedigree