lnfluence of SCENlC recommendations on terminology used for histopathologic diagnosis of inflammatory bowel disease-associated dysplasia
2022-08-19 05:31:54YuanLiHanlinWang
lNTRODUCTlON
Patients with inflammatory bowel disease (IBD),either ulcerative colitis (UC) or Crohn disease (CD),have an increased risk of developing colorectal cancer (CRC).IBD-associated CRC constitutes 10%-15%of deaths in IBD patients[1].The risk of developing CRC in UC is similar to that in CD[2,3].Dysplasia,which is stratified by histopathologic features into low-grade dysplasia (LGD) and high-grade dysplasia(HGD),is currently considered the best marker of CRC risk in IBD.Surveillance colonoscopy therefore is recommended to detect dysplasia for early CRC prevention.Dysplastic foci may be visible under colonoscopy as raised lesions or invisible found on random (non-targeted) biopsies of the colonic mucosa.Invisible dysplasia,especially HGD,is usually an indication of total colectomy.
Raised or polypoid dysplasia in the setting of IBD has been termed “dysplasia-associated lesion or mass (DALM)” in the past,which was believed to be associated with a high risk for CRC development[4,5].Therefore,a diagnosis of DALM usually meant total colectomy for cancer prevention[5].However,it is extremely difficult or even impossible for endoscopists and pathologists to distinguish a DALM lesion from a sporadic adenoma,another polypoid precancerous lesion of CRC that is not associated with IBD.Similar to that in the general population,the occurrence of sporadic adenoma in IBD patients also increases with age,but its progression to CRC appears to take much longer.Complete removal of a sporadic adenoma by endoscopic polypectomy is considered an adequate treatment for cancer prevention[6].In addition,with the advancement in endoscopic technology and increasing use of highresolution endoscopy,chromoendoscopy,image-enhanced endoscopy and magnifying endoscopy,many invisible dysplastic foci under routine endoscopy in IBD patients now become visible[7],and many of them can be completely removed under endoscopy without the necessity of colectomy.Furthermore,recent studies have shown that cancer risk is not increased if DALM lesions can be completely removed by endoscopy,and thus total colectomy is also unnecessary[8,9].These changes in practice have greatly reduced the necessity of total colectomy for CRC prevention in IBD patients.
With these new developments,the International Consensus Recommendations on Surveillance for Colorectal Endoscopic Neoplasia Detection and Management in Inflammatory Bowel Disease Patients(SCENIC) were published in 2015[10],which addressed two important issues: How surveillance colonoscopy should be performed for dysplasia detection,and how dysplasia should be managed.
According to SCENIC recommendations,endoscopically visible dysplasia can be categorized into polypoid (≥ 2.5 mm,pedunculated or sessile) and non-polypoid (superficially elevated and < 2.5 mm,flat or depressed) lesions.It is also recommended that the terms “DALM”,“adenoma-like” and “nonadenoma-like” be abandoned.The aim of this study was to investigate whether the SCENIC recommendations had any influence on the terminologies used by pathologists to diagnose dysplasia detected during surveillance colonoscopies in IBD patients.
Will you be off at once? So he was frightened and went out; but he felt quite faint, and trembled and shook, and his knees and legs began to give way under him
MATERlALS AND METHODS
Study groups
We retrospectively reviewed all pathology reports from patients who had clinically established diagnosis of UC and underwent surveillance colonoscopy with biopsy at Ronald Reagan UCLA Medical Center during two periods of time: January 2012 through December 2014 (pre-SCENIC) and January 2016 through December 2018 (post-SCENIC).Patients with CD,indeterminate colitis and first-time diagnosis of UC were excluded.Endoscopic biopsies from UC patients who had already undergone total colectomy were also excluded from the study.A total of 1203 colonoscopic biopsies from 901 UC patients during the pre-SCENIC period (2012-2014) and a total of 1273 biopsies from 977 UC patients during the post-SCENIC period (2016-2018) were reviewed.Their corresponding endoscopic findings (
,polyp or other elevated lesions) and histopathologic diagnoses (
,adenoma,hyperplastic polyp or others) were recorded.Clinical indications for total colectomy for UC patients and corresponding histopathologic findings in colectomy specimens were also recorded and compared between the preand post-SCENIC periods.The study was approved by the Institutional Review Board at UCLA.
Statistical analysis
Clinicopathologic and outcome findings were compared between the pre- and post-SCENIC groups using the
or Fisher exact test (for categorical features).All statistical analyses were performed using the SPSS software.
< 0.05 was considered statistically significant.
RESULTS
Polyps and polypoid lesions removed by targeted biopsies/polypectomies
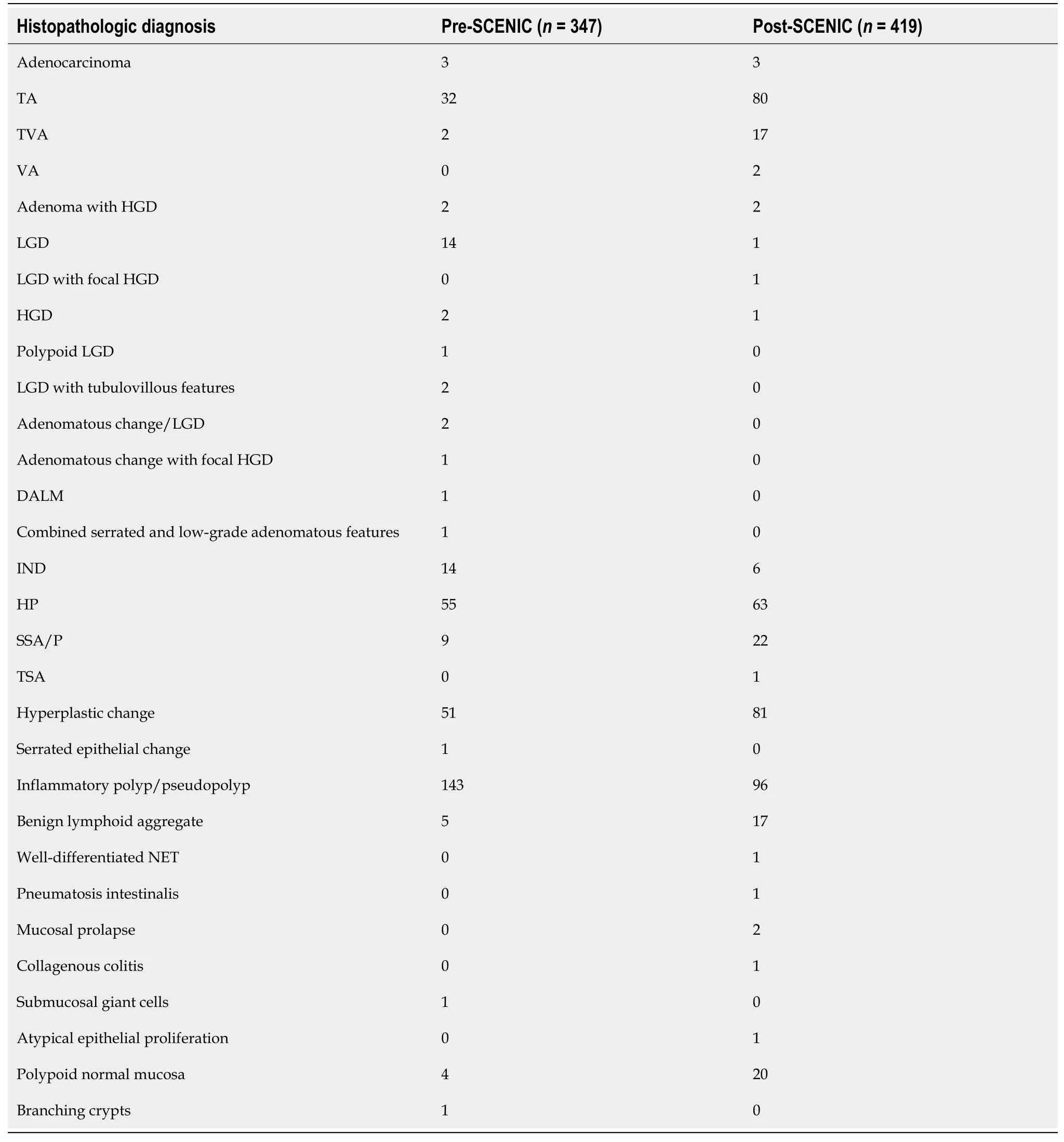
A total of 347 polyps/polypoid lesions were detected and removed among 1203 endoscopic biopsies(28.8%) during 2012-2014 (Table 1).Among these polyps/polypoid lesions,60 (17.3%) were found to be dysplastic/adenomatous.In pathology reports,39 of 60 (65.0%) cases were directly diagnosed as“adenoma” (
= 36) or “adenomatous change” (
= 3).These included 17 cases with multiple adenomatous lesions.Nineteen (31.7%) cases were diagnosed as “dysplasia” (LGD,
= 14; polypoid LGD,
= 1; LGD with tubulovillous features,
= 2; HGD,
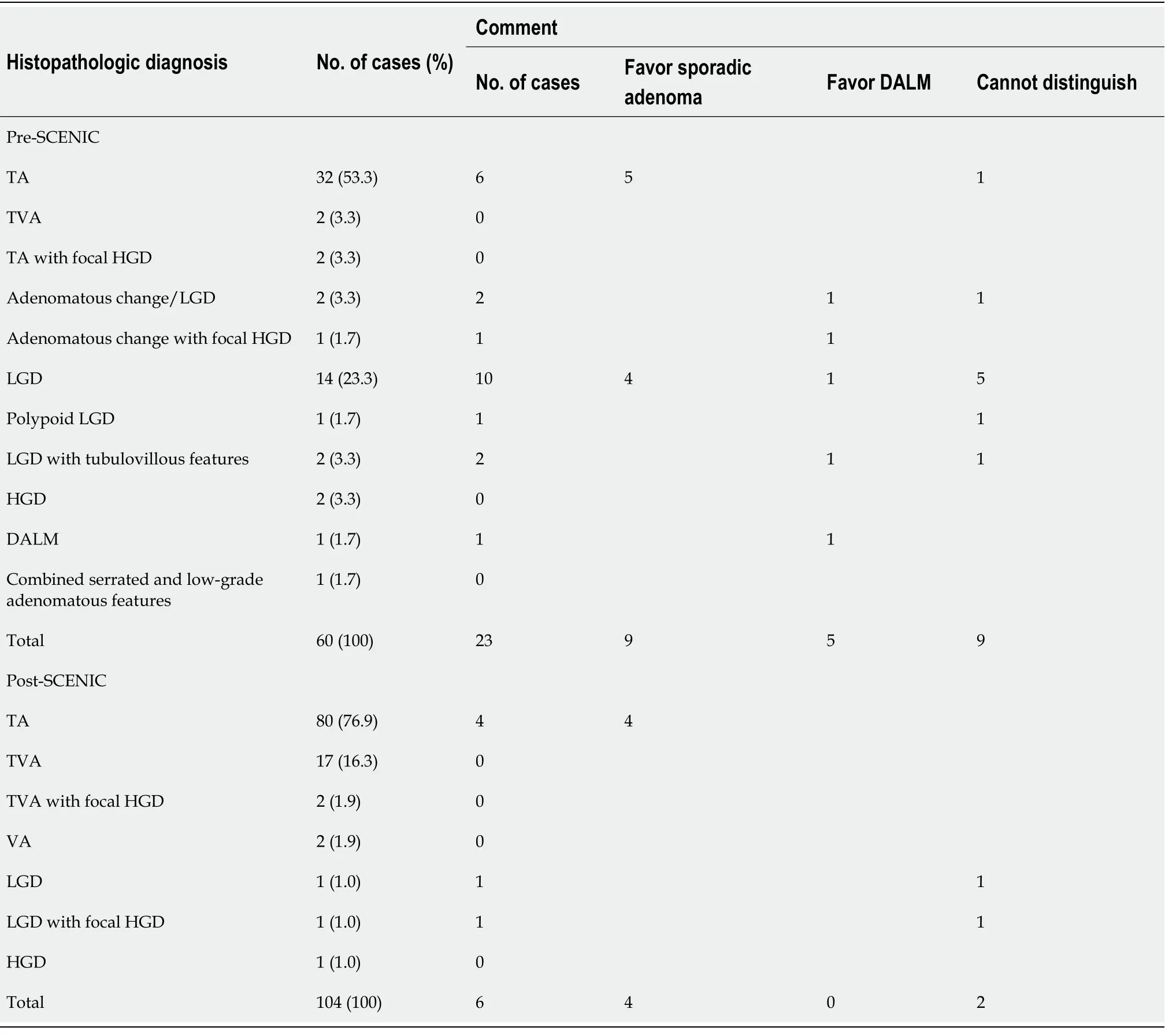
= 2),of which 9 had multiple dysplastic lesions.One (1.7%) polypoid dysplastic lesion was diagnosed as “DALM”,and another polyp was diagnosed as “combined serrated and low-grade adenomatous features”.A comment on the distinction between sporadic adenoma and DALM was included in pathology reports for 23 (38.3%) of these cases(Table 2).These included 9 of 39 (23.1%) cases diagnosed as “adenoma” or “adenomatous change” and 13 of 19 (68.4%) cases diagnosed as “dysplasia”.Of the cases diagnosed as “adenoma”,sporadic adenoma was favored for 5 (55.6%) cases in the comment,DALM for 2 (22.2%),and indistinguishable for 2 (22.2%).Of the cases diagnosed as “dysplasia”,sporadic adenoma was favored for 4 (30.8%) cases,DALM for 2 (15.4%),and indistinguishable for 7 (53.8%).The single case diagnosed as “DALM” also had a comment to further favor the diagnosis.
As shown in Table 1,a total of 419 polyps/polypoid lesions were identified and removed among 1273 endoscopic biopsies (32.9%) during 2016-2018.Of the 104 (24.8%) polyps/polypoid lesions that were found to be dysplastic/adenomatous,101 (97.1%) were directly diagnosed as “adenoma”.These included 21 cases with multiple adenomatous lesions.Only 3 (2.9%) polyps was diagnosed as“dysplasia”,which were all diagnosed in 2016.As shown in Table 2,only 6 (5.8%) of these cases had a comment in pathology reports on the distinction between sporadic adenoma and DALM,including 4 cases diagnosed as “adenoma” (all favored sporadic adenoma) and 2 diagnosed as “dysplasia” (both stated as indistinguishable).Except for one case diagnosed in early 2017,all cases with comments were diagnosed in 2016.
Compared to the pre-SCENIC period,more cases were simply diagnosed as adenoma (97.1%
65.0%;
< 0.001) and much fewer cases had a comment in pathology reports (5.8%
38.3%;
< 0.001)during the post-SCENIC period.In fact,all polyps or polypoid lesions that showed dysplastic/adenomatous features were simply diagnosed as adenoma since 2017,and none of these cases had a comment in pathology report regarding the distinction between sporadic adenoma and DALM after early 2017.
And long after everyone else had given up hope Ivan and Marie would wander through the woods crying Snowflake, my dove, come back, come back! And sometimes they thought they heard a call, but it was never the voice of Snowflake
Invisible dysplasia on random biopsies
The witch s cottage is one of the more popular elements in illustrations of the tale. To see several illustrators visions of the house, visit the Illustrations of Hansel and Gretel page.Return to place in story.
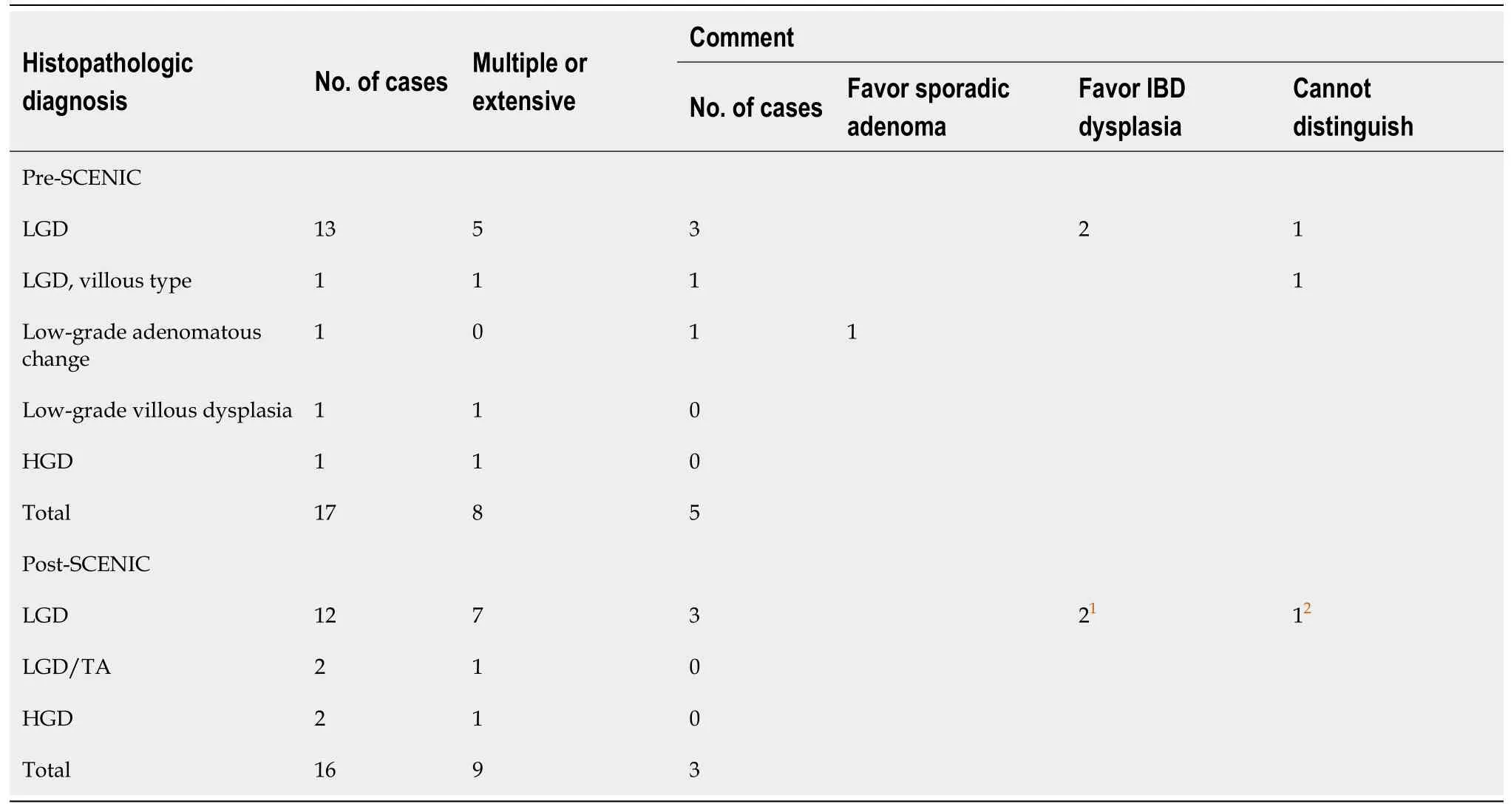
During 2012-2014,17 of 1203 (1.4%) cases were diagnosed to have dysplasia on random biopsies(Table 3).Among them,8 (47.1%) showed multiple foci of or extensive dysplasia.Five (29.4%) cases had a comment in pathology reports.For 2 cases,IBD-associated dysplasia was favored considering the background of chronic colitis and the random nature of the biopsies.One case was diagnosed as “lowgrade adenomatous change” and sporadic adenoma was favored in the comment despite the random nature of the biopsy.For the remaining 2 cases,the comment stated that a definitive distinction between IBD-associated dysplasia and sporadic adenoma could not be made based on histologic assessment alone and recommended clinical and endoscopic correlation.
The swineherd--that is to say--the Prince, for no one knew that he was otherthan an ill-favored swineherd, let not a day pass without working atsomething; he at last constructed a rattle18, which, when it was swung round,played all the waltzes and jig19 tunes20, which have ever been heard since thecreation of the world.
Dysplasia in IBD can be either flat (endoscopically invisible) or elevated (endoscopically visible).Elevated lesions were used to be called “DALMs”,which were believed to have a high association with cancer and thus regarded as a strong indication for colectomy[11].DALMs are a group of heterogeneouslesions which can be further divided into adenoma-like and non-adenoma-like based on their endoscopic appearance.Non-adenoma-like DALMs refer to velvety patches,plaques,irregular bumps and nodules,wart-like thickenings,stricturing lesions,and broad-based masses.These lesions are believed to carry a high risk of concurrent malignancy,often representing the surface of an invasive adenocarcinoma and therefore often requiring colectomy[8].On the other hand,adenoma-like DALMs are well-circumscribed lesions similar to sporadic adenomas endoscopically and pathologically.It has been suggested that adenoma-like DALMs that occur outside or proximal to the areas of mucosa involved by inflammation are considered sporadic in origin and can be managed conservatively by polypectomy.On the contrary,adenoma-like DALMs detected within the area of inflammation may be IBD-associated and thus colectomy and close surveillance may need to be considered.Other features favoring IBD-associated adenoma-like DALMs include young age at diagnosis,long duration of disease,prominent villous architecture,a mixture of normal and dysplastic epithelia at the surface of polyp,“bottom-up” dysplasia,increased inflammation in polyp,presence of stalk dysplasia,and a high frequency of
and a low frequency of
mutations[12-15].However,none of these features has proven to be specific despite the great efforts made by pathologists in the distinction between IBDassociated adenoma-like DALMs and sporadic adenomas.
SSA/P on targeted biopsies/polypectomies
For endoscopically invisible dysplasia,histopathologic interpretation of random surveillance biopsies plays an essential role in clinical management.Current recommendation for invisible HGD is colectomy given the high risk of synchronous and metachronous carcinoma[18].For endoscopically invisible LGD,the management is controversial.The American Society for Gastrointestinal Endoscopy recommended colectomy for multifocal LGD but an individualized approach for unifocal LGD[19].We had a total of 94 colectomies for UC patients during the pre- and post-SCENIC periods.The majority (72.3%) of the surgeries were performed for medically refractory disease and nonneoplastic complications.The rest of patients (27.7%) had resections for carcinoma,HGD,multifocal LGD,and unifocal LGD diagnosed on surveillance biopsies.There were 4 patients who underwent colectomies for unifocal LGD,all of which occurred during the pre-SCENIC period.Three cases had a polyp/mass detected during surveillance endoscopy,which ranged in size from 1.0 cm to 6.5 cm.Only one case had resection based on histopathologic diagnosis of unifocal LGD on a random surveillance biopsy.
Then said the poor woman, From whence knowest thou that I was a queen? The white maiden answered, I am an angel sent by God, to watch over thee and thy child
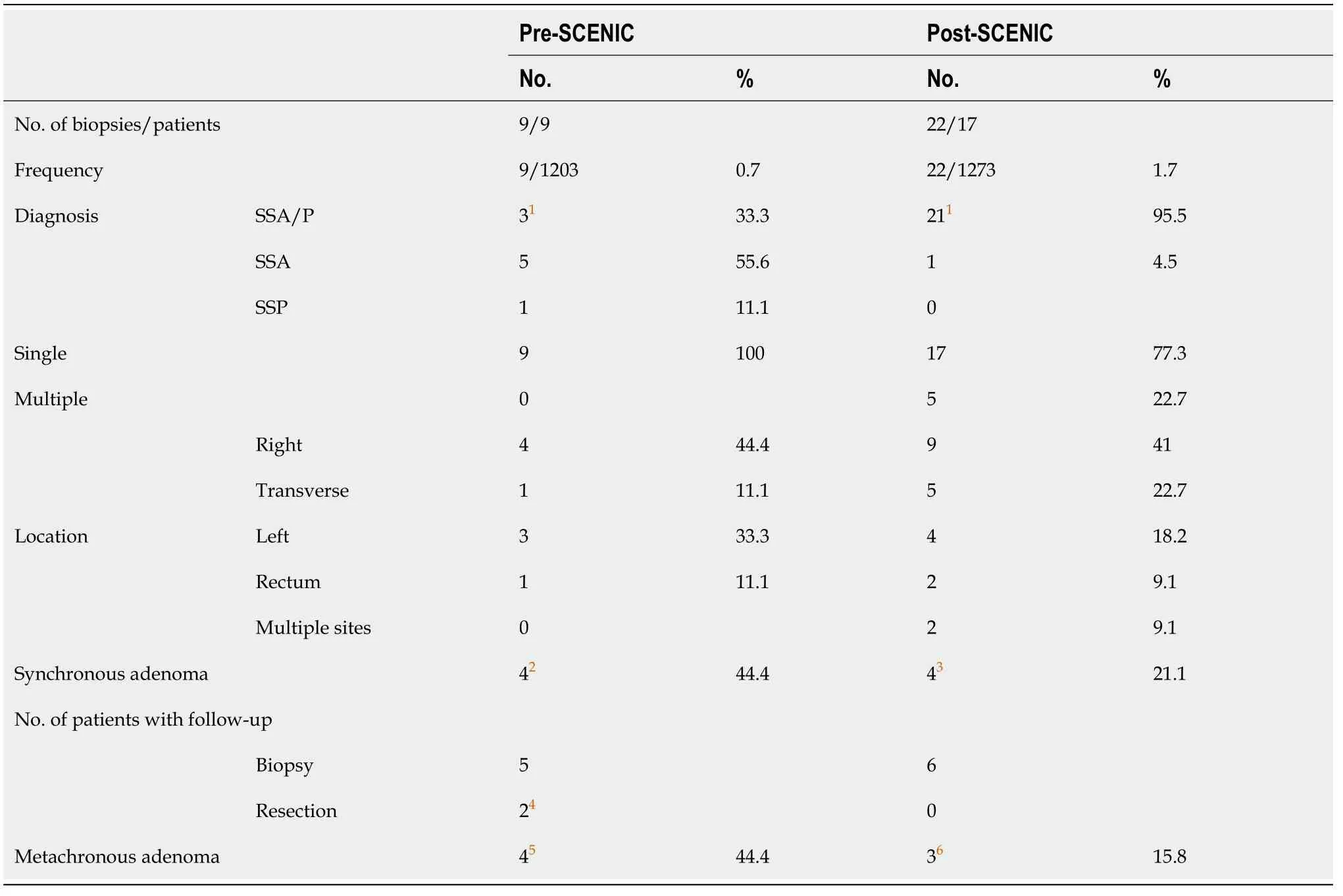
During 2016-2018,22 of 1273 cases (1.7%) from 19 patients were diagnosed as “SSA/P”,including one case diagnosed as “SSA” in 2018 and one case diagnosed as “SSA/P with low-grade cytologic dysplasia”.None of the cases had a comment in pathology report on the significance of the lesion.Six(27.3%) patients had follow-up data from subsequent colonoscopic biopsies.Adenoma was found in one and SSA/P in 2 patients.No dysplastic lesions were detected in the remaining 3 patients.None of the patients underwent surgical resection.
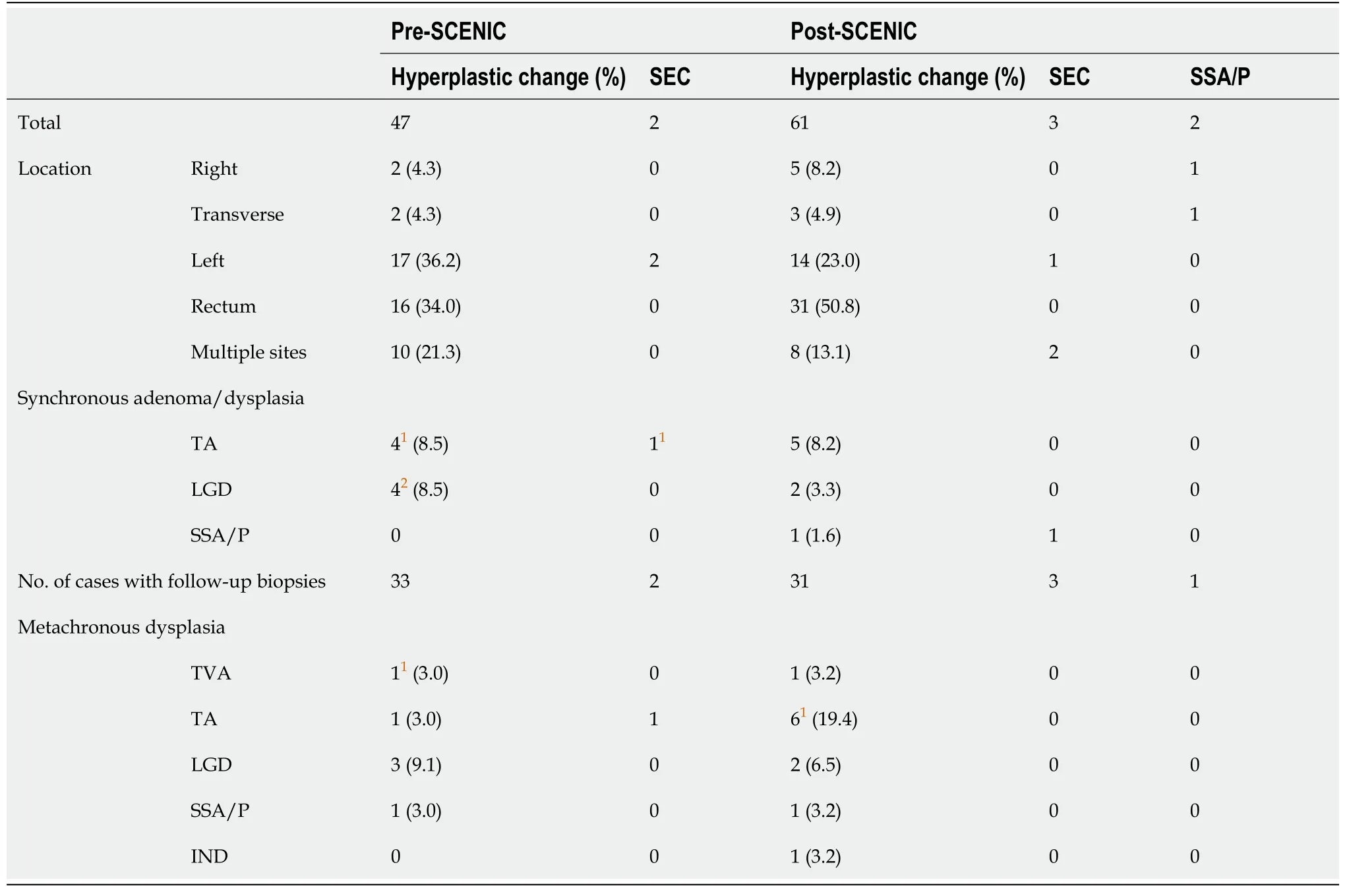
SEC on random biopsies
During 2016-2018,a total of 66 (5.2%) cases showed serrated colonic mucosa on random biopsies,which was termed “hyperplastic change” (
= 61),“SEC” (
= 3),and “SSA/P” (
= 2).Similar to that seen during pre-SCENIC period,the left colon and rectum were the most common locations (72.7%).Synchronous adenoma/dysplasia was found in 9 (13.6%) cases.Five of them had synchronous TA,2 had LGD on random biopsies,and 2 had SSA/P.Thirty-five (53.0%) cases had follow-up biopsies.Metachronous adenoma/dysplasia was found in 10 (28.6%) cases including 2 cases showing LGD on random biopsies.
During 2012-2014,a total of 49 (4.1%) cases showed serrated colonic mucosa on random biopsies(Table 5),which was termed “hyperplastic change” (
= 47) or “SEC” (
= 2).The most common locations were the left colon and rectum (71.4%).Synchronous adenoma/dysplasia was found in 9(18.4%) cases.Five of them had synchronous TA including 2 with multiple TAs.The other 4 cases had synchronous LGD on random biopsies including 2 with multiple foci of LGD.Thirty-five (71.4%) cases had follow-up biopsies.Metachronous adenoma/LGD was found in 7 (20.0%) of these cases including one case with multiple tubulovillous adenomas (TVA) and 3 cases with LGD on random biopsies.
Thou, Vasilissa, they both said, shalt go and fetch the fire, for thou hast neither steel pins nor silver needles and cannot see to spin thy flax! They both rose up, pushed Vasilissa out of the house and locked the door, crying:
During 2016-2018,16 of 1273 (1.3%) cases were diagnosed to have dysplasia on random biopsies,including 9 (56.3%) that showed multiple foci of or extensive dysplasia.Three (18.8%) cases had a comment in pathology report on the nature of dysplasia,including 2 diagnosed in 2016 and one in 2017.IBD-associated dysplasia was considered in the comment for 2 cases.For the other case,diagnosed in 2016,the comment stated that the distinction between IBD-associated dysplasia and sporadic adenoma could not be made reliably on histologic grounds.
Indications for total colectomies
Table 6 shows that during 2012-2014,a total of 54 UC patients underwent total colectomies,40 (74.1%) of which were done for medically refractory colitis (
= 34) or nonneoplastic complications (
= 6).These patients had no prior history of dysplasia or neoplasia.Histopathologic examination of colectomy specimens showed no dysplasia or neoplasia in 38 (95%) cases.One of the two remaining cases was incidentally found to have multiple foci of well-differentiated (low-grade) neuroendocrine tumor in therectum that ranged in size from 0.3 cm to 1.0 cm and invaded the lamina propria,muscularis mucosae and focally the superficial submucosa.No lymph node metastasis was identified.The other case was found to have a small TA.Fourteen (25.9%) patients underwent surgeries for adenocarcinoma or dysplasia detected on surveillance colonoscopies.Six (42.9%) cases were found to have invasive adenocarcinoma in resection specimens.
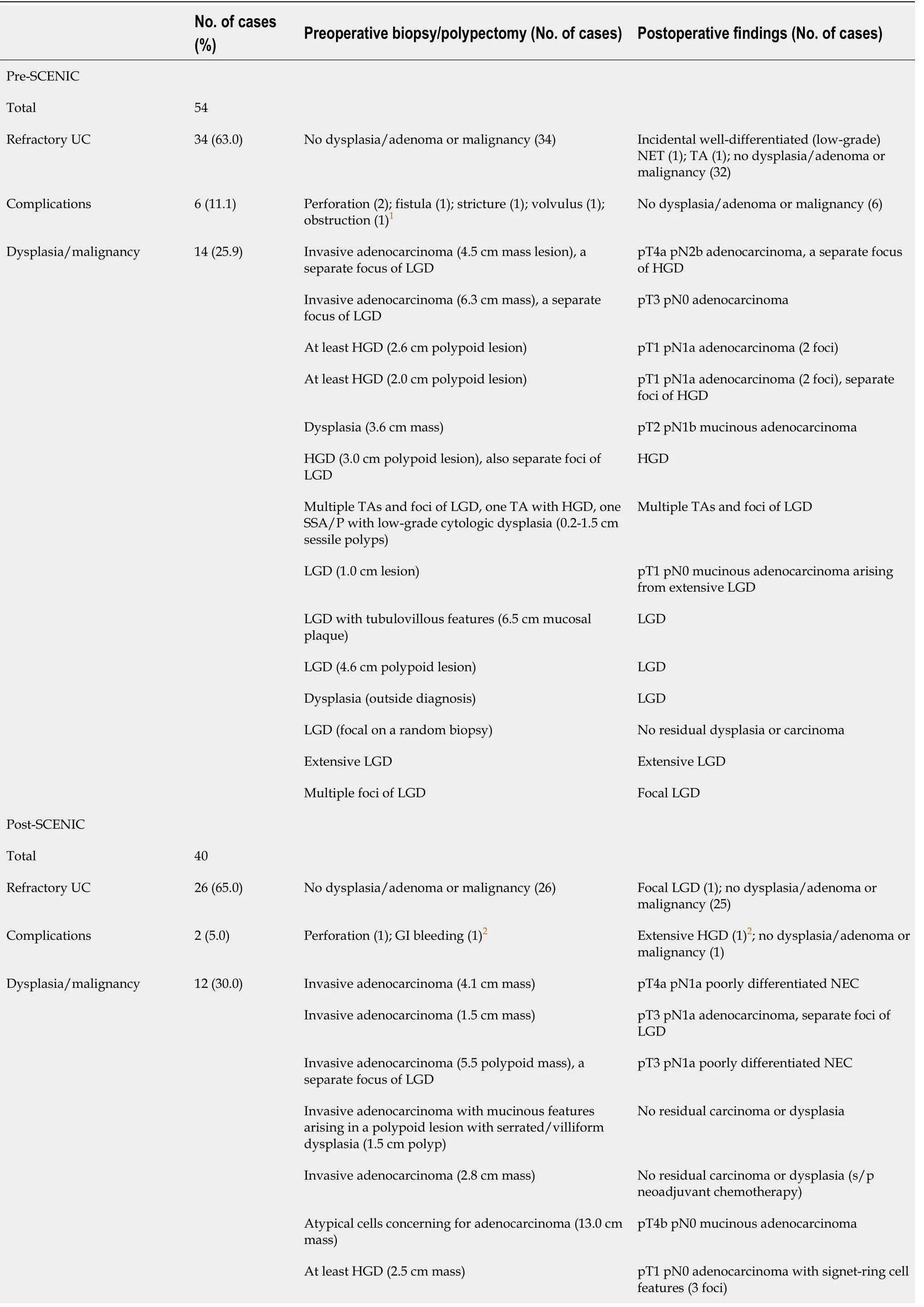

During 2016-2018,40 patients underwent total colectomies,28 (70.0%) of which were done for refractory colitis (
= 26) or nonneoplastic complications (
= 2).These patients did not have a prior history of dysplasia or neoplasia.On resection specimens,focal LGD was incidentally found in one case.There was another case where surveillance biopsy showed a focus indefinite for dysplasia but the resection specimen showed extensive HGD.Twelve (30.0%) patients had colectomies for carcinoma,dysplasia or large adenomas detected on surveillance colonoscopies.Invasive carcinoma was found in resection specimens in 7 (58.3%) cases,among which 2 were poorly differentiated neuroendocrine carcinomas.Two cases with preoperative diagnosis of adenocarcinoma showed no residual carcinoma or dysplasia in resection specimens.One case had a 1.5 cm polyp that was completely removed by endoscopic polypectomy prior to surgery.The other case was treated with neoadjuvant chemotherapy prior to surgery with complete response.
DlSCUSSlON
There was no significant difference in the frequency of dysplasia diagnosed on random biopsies between the pre- and post-SCENIC periods (1.4%
1.3%;
> 0.05).However,the terminologies used for the diagnosis appeared to be more consistent during the post-SCENIC period in comparison to the pre-SCENIC period.
In 2015,the SCENIC recommendations were published,which incorporated the latest understanding on surveillance and management of dysplasia in IBD[10].According to this consensus,dysplastic lesions can be simply classified as endoscopically visible and invisible.Visible dysplasia,by definition,is histopathologically proven dysplasia on a targeted biopsy of a concerning area recognized on colonoscopic examination.Invisible dysplasia is histopathologically proven dysplasia on a random biopsy from a visually unremarkable colonic mucosa[10].For endoscopically visible lesions,the determination of endoscopic resectability,rather than the distinction between adenoma-like and non-adenoma-like or between IBD-associated dysplasia and sporadic adenoma,becomes important according to the consensus recommendations.Therefore,the term “DALM” becomes no longer useful and should be abandoned.For endoscopically visible and resectable lesions,either polypoid or non-polypoid,complete endoscopic polypectomy or excision followed by continued surveillance is a sufficient treatment,though the borders of non-polypoid lesions may be difficult to delineate and complete excision can be technically challenging.For patients with endoscopically invisible dysplasia,referral to an experienced IBD specialist with further examination using chromoendoscopy with high-definition colonoscopy is suggested[10,16,17].If dysplasia is still invisible,management will depend on the grade of dysplasia.While the SCENIC consensus provides recommendations for surveillance and management of dysplasia in IBD patients,no specific suggestions are made on diagnostic terminologies that pathologists should use when reporting dysplastic lesions in IBD patients.
I want to be a lawyer when I group up, a trial lawyer in fact. I know I d be good at that. I would be responsible for researching the crime, examining the evidence and truthfully presenting the case.
We were curious about whether the SCENIC recommendations had any influence on the terminologies used by pathologists in their reports for the diagnosis of dysplastic/adenomatous lesions detected in IBD patients.According to our single institutional experience,the diagnostic terms used by pathologists were more uniform and consistent in the post-SCENIC period.Specifically,more polypoid dysplastic lesions were directly diagnosed as adenomas (with or without HGD) in the post-SCENIC period (97.1%) in comparison to the pre-SCENIC period (65.0%).In the pre-SCENIC period,approximately one-third of polypoid dysplastic lesions were diagnosed as “LGD” or “HGD”,which could potentially be confused with invisible dysplasia diagnosed on random biopsies.These diagnostic terms have never been used again by pathologists in our institution for targeted biopsies or polypectomies on visible lesions after 2016.It is interesting to note that our pathologists made much less efforts to attempt to distinguish adenoma-like DALM from sporadic adenoma in their practice in the post-SCENIC period.This is evidenced by a dramatic reduction in the number of pathology reports that included a diagnostic comment on the distinction between sporadic adenoma and DALM.In fact,the few cases that had a comment in the post-SCENIC period were all diagnosed in 2016,with only one in early 2017.None of the cases diagnosed after early 2017 carried a diagnostic comment.These changes in practice indicate that pathologists were much less struggling once the stress of distinguishing IBD-associated dysplasia from sporadic adenoma was relieved.It is also interesting to note that in the pre-SCENIC period,only one of 60 (1.7%) polypoid dysplastic lesions was directly diagnosed as “DALM” and only 5 of 23 (21.7%)cases with a comment were favored to be “DALM”,further indicating how cautious the pathologists were in making such a diagnosis given its potential clinical consequence.
It was like Granddad to be saying that. He was trying to make it easier. He had pretended all along that he wanted to go away to the great brick building—the government place. There he d be with so many other old fellows, having the best of everything. . . . But Petey hadn t believed Dad would really do it, not until this night when he brought home the blanket.
During 2012-2014,9 of 1203 (0.7%) biopsies from UC patients had a diagnosis of SSA/P with variable terms used by pathologists (Table 4).These included “SSA” (
= 5),“SSP” (
= 1),“SSA/P” (
= 2),and“SSA/P with low-grade cytologic dysplasia” (
= 1).Three (33.3%) cases,biopsied from “thickened fold”,had a comment in pathology reports on the significance of serrated polyps in the setting of IBD.Seven (77.8%) cases had follow-up colonoscopic biopsies (
= 5) or surgical resections (
= 2).Of the 2 resection cases,one case that showed SSA/P with cytologic dysplasia and multiple synchronous tubular adenomas (TA) on surveillance biopsies still showed adenomas in resection specimen.No HGD orinvasive carcinoma was identified.The other case had resection for prior diagnosed dysplasia and sigmoid stricture.No dysplasia,adenoma or invasive carcinoma was identified in resection specimen for this case.The remaining 5 cases had no dysplasia or adenoma identified in the follow-up biopsies.
Colorectal serrated polyps,which include hyperplastic polyp,SSA/P and traditional serrated adenoma,have been implicated in the pathogenesis in a subset of CRC.SSA/P in general population has been widely studied[20] and the serrated neoplasia pathway has been thought to be responsible for at least 20% of sporadic CRC[21,22].These polyps are distinct from conventional adenomas as they frequently harbor
mutations and show CpG island methylation.There is evidence,though limited,to support the notion that the clinicopathologic and molecular characteristics of SSA/P found in IBD patients are similar to those in general population[23-25].Similar to conventional adenomas,these serrated lesions are endoscopically detectable as polyps and thus can be easily removed by polypectomy.No correlation of occurrence of these lesions with the background inflammation has been reported[25,26].The changes in our pathology reports also reflected this recognition.During 2012-2014,before SCENIC consensus,variable diagnostic terms had been used including SSA,SSP and SSA/P.A diagnosis comment was included in 1/3 of pathology reports on the nature of the lesion.Since 2016,however,the term SSA/P was consistently used,with no further comment.
SEC,previously called hyperplastic change,is the currently preferred term to describe mucosal changes similar to SSA/P or hyperplastic polyp on biopsies from non-polypoid colonic mucosa from IBD patients.Histologically,it is recognized by distorted architecture but lacks typical features of cytologic dysplasia.It is typically found on random biopsies during surveillance colonoscopy and characterized by serrated crypt architecture,usually involving the upper half of the crypt,and without cytologic features of dysplasia[27].When endoscopically visible,SEC is typically flat or shows nodular mucosa without a discrete polypoid configuration[28].Whether SEC carries a risk of progression to dysplasia and CRC is currently unknown,but several studies have suggested that the finding of SEC in IBD patients may be associated with higher rates of colonic synchronous and metachronous neoplasia[27,29,30].Our limited data also showed a high association of SEC with synchronous and metachronous neoplasia in UC patients.Specifically,of the 81 patients who had a SEC diagnosis,38 (46.9%) had synchronous or metachronous adenomas.There was no significant difference between the pre-SCENIC and post-SCENIC periods.Further controlled studies are needed to determine whether SEC is indeed a preneoplastic marker in IBD patients.
There are a couple of limitations in this retrospective study.First,this is a single institutional study.Our experience might not be the same as that in other institutions.Second,all data were collected from previous pathology reports signed by different pathologists.It is understandable that different pathologists might have used different diagnostic criteria for various entities and might have different thresholds for the diagnosis of dysplasia even though they were practicing in the same institution.Nonetheless,these limitations did not appear to affect the conclusions of the study.
CONCLUSlON
Although the SCENIC recommendations were aimed to address management issues,they had a significant impact on the terminologies pathologists used in their practice based on our institutional experience.Specifically,the recommendations relieved pathologists from the burden of distinguishing“DALM” from sporadic adenoma in IBD patients,which is an extremely challenging and stressful differential.Currently,all polypoid or visible dysplastic lesions are simply diagnosed as “adenoma” in our institution,irrespective of whether or not they are IBD-associated because of the same management approaches.The term “dysplasia” is reserved only for invisible lesions found in random biopsies.The consistent use of the diagnostic terminologies may help reduce potential confusions to clinicians and patients.
Wang HL designed the research,supervised data analysis and manuscript preparation; Li Y collected and analyzed the data,and wrote the manuscript.
There are no conflicts of interest to report.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
United States
Yuan Li 0000-0001-9338-2463; Hanlin L Wang 0000-0003-1409-5234.
Chen YL
A
When the kids came in, he took them for walks along the pier21 near their office. Often she went along and watched Eric, who was becoming a master of sign language, talk and laugh with her boys as no one else had before.
Chen YL
1 Munkholm P.Review article: the incidence and prevalence of colorectal cancer in inflammatory bowel disease.
2003; 18 Suppl 2: 1-5 [PMID: 12950413 DOI: 10.1046/j.1365-2036.18.s2.2.x]
2 Ibraheim H,Dhillon AS,Koumoutsos I,Gulati S,Hayee B.Curriculum review: colorectal cancer surveillance and management of dysplasia in IBD.
2018; 9: 271-277 [PMID: 30245789 DOI:10.1136/flgastro-2017-100919]
3 Goetz M.Endoscopic Surveillance in Inflammatory Bowel Disease.
2018; 34: 66-71 [PMID: 29594172 DOI:10.1159/000485019]
4 Blackstone MO,Riddell RH,Rogers BH,Levin B.Dysplasia-associated lesion or mass (DALM) detected by colonoscopy in long-standing ulcerative colitis: an indication for colectomy.
1981; 80: 366-374 [PMID: 7450425]
5 Bernstein CN,Shanahan F,Weinstein WM.Are we telling patients the truth about surveillance colonoscopy in ulcerative colitis?
1994; 343: 71-74 [PMID: 7903776 DOI: 10.1016/s0140-6736(94)90813-3]
6 Odze RD.Adenomas and adenoma-like DALMs in chronic ulcerative colitis: a clinical,pathological,and molecular review.
1999; 94: 1746-1750 [PMID: 10406230 DOI: 10.1111/j.1572-0241.1999.01201.x]
7 Rutter MD,Saunders BP,Wilkinson KH,Kamm MA,Williams CB,Forbes A.Most dysplasia in ulcerative colitis is visible at colonoscopy.
2004; 60: 334-339 [PMID: 15332019 DOI: 10.1016/s0016-5107(04)01710-9]
8 Odze RD,Farraye FA,Hecht JL,Hornick JL.Long-term follow-up after polypectomy treatment for adenoma-like dysplastic lesions in ulcerative colitis.
2004; 2: 534-541 [PMID: 15224277 DOI:10.1016/s1542-3565(04)00237-x]
9 Wanders LK,Dekker E,Pullens B,Bassett P,Travis SP,East JE.Cancer risk after resection of polypoid dysplasia in patients with longstanding ulcerative colitis: a meta-analysis.
2014; 12: 756-764 [PMID:23920032 DOI: 10.1016/j.cgh.2013.07.024]
10 Laine L,Kaltenbach T,Barkun A,McQuaid KR,Subramanian V,Soetikno R; SCENIC Guideline Development Panel.SCENIC international consensus statement on surveillance and management of dysplasia in inflammatory bowel disease.
2015; 81: 489-501.e26 [PMID: 25708752 DOI: 10.1016/j.gie.2014.12.009]
11 Rubio CA,Befrits R,Jaramillo E,Nesi G,Amorosi A.Villous and serrated adenomatous growth bordering carcinomas in inflammatory bowel disease.
2000; 20: 4761-4764 [PMID: 11205214]
12 Torres C,Antonioli D,Odze RD.Polypoid dysplasia and adenomas in inflammatory bowel disease: a clinical,pathologic,and follow-up study of 89 polyps from 59 patients.
1998; 22: 275-284 [PMID: 9500769 DOI:10.1097/00000478-199803000-00001]
13 Odze RD,Brien T,Brown CA,Hartman CJ,Wellman A,Fogt F.Molecular alterations in chronic ulcerative colitisassociated and sporadic hyperplastic polyps: a comparative analysis.
2002; 97: 1235-1242 [PMID:12014733 DOI: 10.1111/j.1572-0241.2002.05696.x]
14 Mueller E,Vieth M,Stolte M,Mueller J.The differentiation of true adenomas from colitis-associated dysplasia in ulcerative colitis: a comparative immunohistochemical study.
1999; 30: 898-905 [PMID: 10452501 DOI:10.1016/s0046-8177(99)90242-3]
15 Odze RD,Brown CA,Hartmann CJ,Noffsinger AE,Fogt F.Genetic alterations in chronic ulcerative colitis-associated adenoma-like DALMs are similar to non-colitic sporadic adenomas.
2000; 24: 1209-1216 [PMID:10976694 DOI: 10.1097/00000478-200009000-00003]
16 Gaidos JK,Bickston SJ.How to Optimize Colon Cancer Surveillance in Inflammatory Bowel Disease Patients.
2016; 22: 1219-1230 [PMID: 26926040 DOI: 10.1097/MIB.0000000000000685]
17 Soetikno R,Kaltenbach T,McQuaid KR,Subramanian V,Kumar R,Barkun AN,Laine L.Paradigm Shift in the Surveillance and Management of Dysplasia in Inflammatory Bowel Disease (West).
2016; 28: 266-273 [PMID:26866420 DOI: 10.1111/den.12634]
18 Magro F,Gionchetti P,Eliakim R,Ardizzone S,Armuzzi A,Barreiro-de Acosta M,Burisch J,Gecse KB,Hart AL,Hindryckx P,Langner C,Limdi JK,Pellino G,Zagórowicz E,Raine T,Harbord M,Rieder F; European Crohn’s and Colitis Organisation [ECCO].Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis.Part 1: Definitions,Diagnosis,Extra-intestinal Manifestations,Pregnancy,Cancer Surveillance,Surgery,and Ileo-anal Pouch Disorders.
2017; 11: 649-670 [PMID: 28158501 DOI: 10.1093/ecco-jcc/jjx008]
19 American Society for Gastrointestinal Endoscopy Standards of Practice Committee,Shergill AK,Lightdale JR,Bruining DH,Acosta RD,Chandrasekhara V,Chathadi KV,Decker GA,Early DS,Evans JA,Fanelli RD,Fisher DA,Fonkalsrud L,Foley K,Hwang JH,Jue TL,Khashab MA,Muthusamy VR,Pasha SF,Saltzman JR,Sharaf R,Cash BD,DeWitt JM.The role of endoscopy in inflammatory bowel disease.
2015; 81: 1101-21.e1 [PMID:25800660 DOI: 10.1016/j.gie.2014.10.030]
20 Snover DC,Jass JR,Fenoglio-Preiser C,Batts KP.Serrated polyps of the large intestine: a morphologic and molecular review of an evolving concept.
2005; 124: 380-391 [PMID: 16191506 DOI:10.1309/V2EP-TPLJ-RB3F-GHJL]
21 Sweetser S,Smyrk TC,Sinicrope FA.Serrated colon polyps as precursors to colorectal cancer.
2013; 11: 760-7; quiz e54 [PMID: 23267866 DOI: 10.1016/j.cgh.2012.12.004]
22 Snover DC.Update on the serrated pathway to colorectal carcinoma.
2011; 42: 1-10 [PMID: 20869746 DOI:10.1016/j.humpath.2010.06.002]
23 Ko HM,Harpaz N,McBride RB,Cui M,Ye F,Zhang D,Ullman TA,Polydorides AD.Serrated colorectal polyps in inflammatory bowel disease.
2015; 28: 1584-1593 [PMID: 26403785 DOI: 10.1038/modpathol.2015.111]
24 Shen J,Gibson JA,Schulte S,Khurana H,Farraye FA,Levine J,Burakoff R,Cerda S,Qazi T,Hamilton M,Srivastava A,Odze RD.Clinical,pathologic,and outcome study of hyperplastic and sessile serrated polyps in inflammatory bowel disease.
2015; 46: 1548-1556 [PMID: 26297256 DOI: 10.1016/j.humpath.2015.06.019]
25 Jackson WE,Achkar JP,Macaron C,Lee L,Liu X,Pai RK,Lopez R,Burke CA,Allende DS.The Significance of Sessile Serrated Polyps in Inflammatory Bowel Disease.
2016; 22: 2213-2220 [PMID: 27508509 DOI:10.1097/MIB.0000000000000895]
26 Yang C,Tarabishy Y,Dassopoulos T,Nalbantoglu I.Clinical,Histologic,and Immunophenotypic Features of Serrated Polyps in Patients With Inflammatory Bowel Disease.
2018; 11: 355-360 [PMID: 30344807 DOI:10.14740/gr1064w]
27 Parian A,Koh J,Limketkai BN,Eluri S,Rubin DT,Brant SR,Ha CY,Bayless TM,Giardiello F,Hart J,Montgomery E,Lazarev MG.Association between serrated epithelial changes and colorectal dysplasia in inflammatory bowel disease.
2016; 84: 87-95.e1 [PMID: 26709112 DOI: 10.1016/j.gie.2015.12.010]
28 Parian AM,Lazarev MG.Serrated Colorectal Lesions in Patients With Inflammatory Bowel Disease.
2018; 14: 19-25 [PMID: 29491757]
29 Kilgore SP,Sigel JE,Goldblum JR.Hyperplastic-like mucosal change in Crohn's disease: an unusual form of dysplasia?
2000; 13: 797-801 [PMID: 10912940 DOI: 10.1038/modpathol.3880138]
30 Johnson DH,Khanna S,Smyrk TC,Loftus EV Jr,Anderson KS,Mahoney DW,Ahlquist DA,Kisiel JB.Detection rate and outcome of colonic serrated epithelial changes in patients with ulcerative colitis or Crohn's colitis.
2014; 39: 1408-1417 [PMID: 24779703 DOI: 10.1111/apt.12774]
 World Journal of Gastrointestinal Oncology2022年8期
World Journal of Gastrointestinal Oncology2022年8期
- World Journal of Gastrointestinal Oncology的其它文章
- Colitis and colorectal tumors should be further explored and differentiated
- Exosomes:Promising biomarkers and targets for cancer
- Acute or chronic inflammation role in gastrointestinal oncology
- Ewing sarcoma of the ileum with wide multiorgan metastases:A case report and review of literature
- RASSF1A methylation as a biomarker for detection of colorectal cancer and hepatocellular carcinoma
- Evaluation of the diagnostic value of serum-based proteomics for colorectal cancer