Optical coherence tomography evaluation of retinal nerve fiber layer thickness in non-arteritic anterior ischemic optic neuropathy and primary open angle glaucoma: a systematic review and Meta-analysis
2022-08-10 01:39:50YuXinTongXinYuZhangYiHeZongLinChenBingJiang
INTRODUCTION
(2)定量分析結(jié)合定性分析:對定性化文獻(xiàn)資料歸整,以制度工作任務(wù)轉(zhuǎn)換為調(diào)研體系維度,通過層次分析法等確定維度權(quán)重,設(shè)置公眾角度評價問卷以量化考量看法,探究各變量間內(nèi)在關(guān)系與變化規(guī)律,尋找制度實(shí)施各項(xiàng)具體工作的滿意測度,提出優(yōu)化建議。
Evaluation of the peripapillary retinal nerve fiber layer(pRNFL) thickness enables clinicians to assess the degree and the pattern of the damage to the RGC axons coursing toward the ONH. Multiple quantitative retinal imaging techniques comprising scanning laser polarimetry, Heidelberg retinal tomography, as well as optical coherence tomography(OCT)
, have been utilized to measure RNFL thickness.Among them, spectral-domain optical coherence tomography(SD-OCT), which is the latest generation of OCT, provides a high-resolution and enhance-depth visualization of the retina and the ONH
.
7.在浦東新區(qū)的保稅區(qū)內(nèi),允許外商貿(mào)易機(jī)構(gòu)從事轉(zhuǎn)口貿(mào)易,以及為區(qū)內(nèi)外商投資企業(yè)代理本企業(yè)生產(chǎn)用原材料、零配件進(jìn)口和產(chǎn)品出口業(yè)務(wù)。對保稅區(qū)內(nèi)的主要經(jīng)營管理人員,可辦理多次出入境護(hù)照,提供出入境的方便。
Primary open angle glaucoma (POAG) is an age-related neurodegenerative optic neuropathy characterized by the progressive deterioration of retinal ganglion cells (RGCs)and their axons
, followed by the excavation of the optic nerve head (ONH) and impaired visual field (VF)
. Nonarteritic anterior ischemic optic neuropathy (NAION) is a nonglaucomatous optic neuropathy that presents with the sudden painless loss of vision, optic disc edema with resolution after several weeks and optic disc pallor at the atrophic stage
.Similar to POAG, NAION also results in the loss of RGCs and their axons. However, the pathophysiological mechanisms underlying the different ONH configuration changes in these two diseases are not completely understood
.
With the utilization of SD-OCT in daily routine diagnosis,several studies have demonstrated that the attenuation of average pRNFL thickness is common in NAION and glaucoma
,where NAION may mimic with POAG
. However, the pattern and severity of sectoral pRNFL thickness thinning were inconsistent
, which may help reveal the different underlying mechanisms that induce optic damage in these two ophthalmic neuropathies and help differentiate NAION from POAG in a non-invasive manner.
Therefore, we performed this systematic review and Metaanalysis to compare the average and sectoral pRNFL thickness in patients with NAION and those with POAG with similar VF mean deviation (MD), facilitating a better understanding of the biomechanisms that lead to the different patterns of neurodegeneration.
MATERIALS AND METHODS
The present systematic review and Meta-analysis were performed according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA)Statement and the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines
. Three individual investigators (Tong YX, Zhang XY, and He Y) independently conducted the literature search, qualification, data extraction,quality evaluation by Agency for Healthcare Research and Quality (AHQR) checklist, and risk of bias assessment. The present study was registered in PROSPERO (registration number: CRD42020220934).
Literature search was conducted from inception to October, 2021 in PubMed, Cochrane Library and Embase databases. The following search terms were used:“non-arteritic anterior ischemic optic neuropathy”, “NAION”,“glaucoma”, “retinal nerve fiber layer”, “RNFL”, “optical coherence tomography”, “OCT” with no restriction. The search strategies were modified by the requirements of the different databases. Potential eligible articles were included by detailed screening of full-text versions of the literature.
Despite no difference in average pRNFL thickness, the superior pRNFL was significantly thinner in NAION eyes(
=0.031), whereas the inferior sector was significantly thicker(
≤0.001) when the MD of the VF was similar between NAION and POAG. These findings could be explained in several aspects. First, studies have reported that the inferior altitudinal VF defect was more common in NAION patients,although the VF defects tended to be less diffuse compared to POAG, while the superior hemifield loss was more commonly seen in glaucoma patients
. Moreover, the superior altitudinal VF defects can result from the loss of inferior RNFL thickness since structural deterioration can precede VF defects in glaucoma
. These structure-function relationship findings are in line with our findings that the superior pRNFL is significantly thinner in NAION eyes, whereas the inferior pRNFL thickness is significantly thinner in POAG eyes.Second, a longitudinal study revealed that RNFL thickness was lowest superiorly at 6mo from the onset of NAION, indicating that peripapillary structure attenuation was most severe in the superior quadrant in NAION during this period
. Third, the loss of the neuro-retinal rim of glaucoma is shown to start from the inferior temporal to superior nasal sector
, which may account for the different progression patterns between these two diseases. In addition, the diagnostic ability of inferior pRNFL thickness is highest in glaucoma
. Recently, with the use of OCT angiography, a study reported a stronger correlation between inferior peripapillary capillary density and inferior pRNFL thickness in POAG patients compared with NAION patients, suggesting a higher susceptibility of inferior peripapillary capillary density that may contribute to the attenuation of inferior pRNFL in POAG
. Another study revealed that the inferior parafoveal deep vasculature in POAG eyes was lower than that in NAION eyes, indicating that the vulnerable regions of POAG were more susceptible to optic damage
.
陸游在梁益生活時所寫的作品以憂怨哀傷為主調(diào),回到故鄉(xiāng)山陰追憶梁益生活時所寫作品卻以歡喜快樂為主調(diào)。其主調(diào)的矛盾沖突不免令人產(chǎn)生疑問:哪種主調(diào)更真實(shí)?陸游在梁益地區(qū)到底過著怎樣的生活?他對梁益地域的書寫有多少真實(shí)性、可欣賞性?
Stata version 12.0 (StataCorp, Texas, USA)and Review Manager version 5.4.1 (Cochrane Collaboration,London, UK) were used for the statistical analyses. We used weighted mean difference (WMD) with a 95% confidence interval (CI) to pool the mean differences in average and sectoral pRNFL thickness between the NAION and POAG groups. A
value <0.05 was regarded to be statistically significant. Statistical heterogeneities among different groups were measured using Cochrane’s
test and quantified by
.We used a fixed-effects model when
<50%
, indicating the heterogeneity was acceptable; otherwise, we employed a random-effects model when
>50%. The stratified analyses were performed by the onset time of NAION and OCT device types. Egger
’s
and Begg
’s
tests were used to evaluate the potential publication bias. The “l(fā)eave-one-out”sensitivity analysis concerning the average and quadrant pRNFL thickness was performed to explore the sources of heterogeneity.
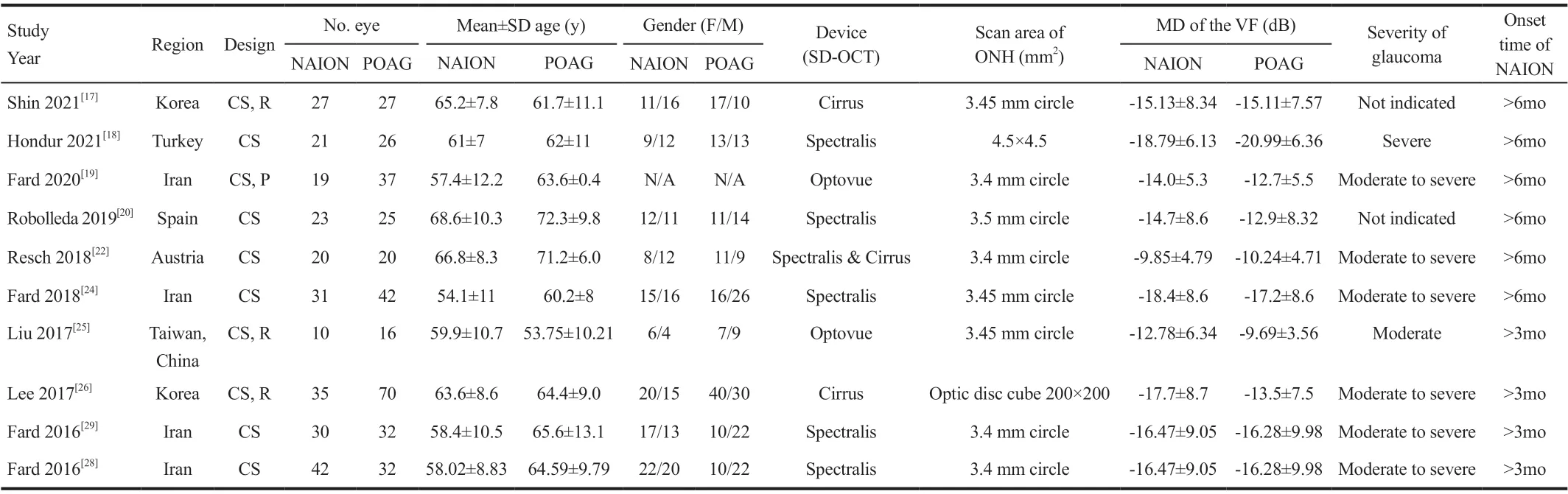
The following information was extracted and summarized: title, first author, publication year, region, study type, number of patients and eyes, source of patients, time periods for identifying patients, mean age of patients, female/male ratios, types of OCT devices, episode of NAION, types of glaucoma, diagnostic criteria, average and quadrant pRNFL thickness, scan protocol and area of ONH, MD of the VF,severity of glaucoma, onset time of NAION. Disagreements were resolved by discussing among all the authors.
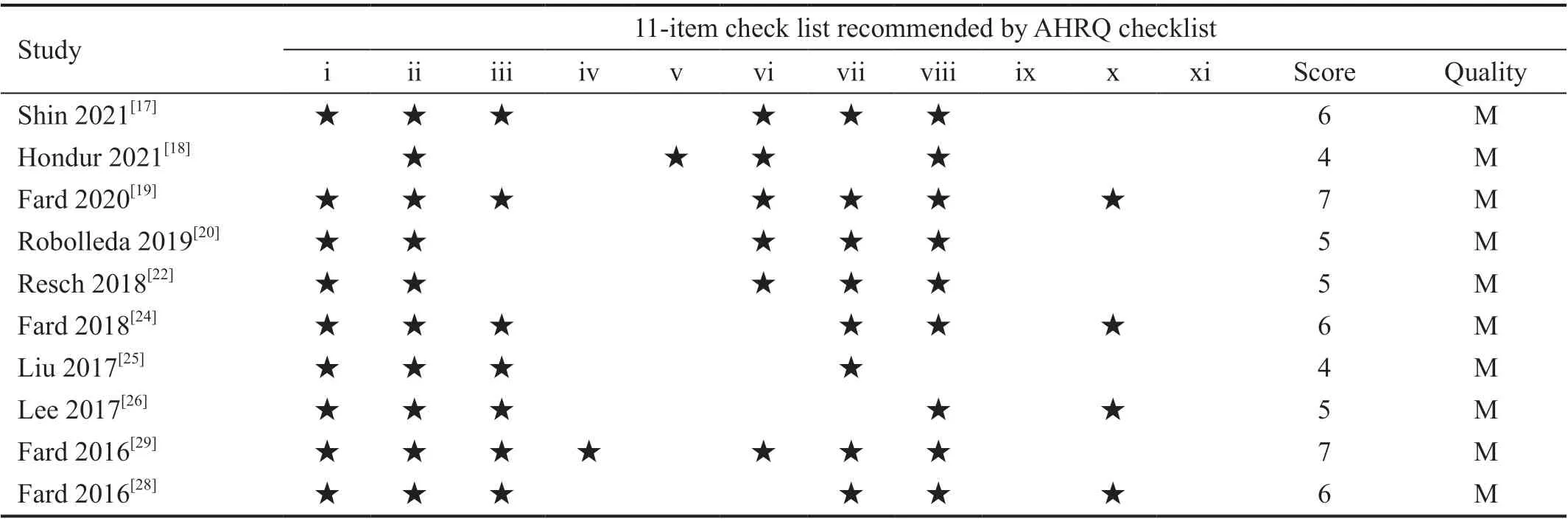
Ten included cross-sectional studies were evaluated based on the AHRQ methodology checklist.
(2)農(nóng)村面源污染和生活污水污染。農(nóng)業(yè)生產(chǎn)使用農(nóng)藥、化肥,利用率低,造成面源污染,以及生活污水均對漁業(yè)養(yǎng)殖水域造成不同程度的污染。
11月25—26日,水利部黨組中心組舉辦黨的十八屆三中全會精神(擴(kuò)大)學(xué)習(xí)班。水利部黨組書記、部長陳雷出席會議,并以《深入貫徹落實(shí)黨的十八屆三中全會精神 在新的歷史起點(diǎn)上譜寫水利改革新篇章》為題作了動員講話。
Exclusion criteria were: 1) conference abstracts, reviews, case reports and animal experiments; 2) enrollment of NAION at the acute stage; 3) different diagnostic standards; 4) noninclusion of SD-OCT based evaluation of pRNFL thickness;5) studies without extractable data.
In some studies, RNFL thickness was displayed by sixquadrant classification method, and in others the fourquadrants classification method was used. To transform the six-quadrant data to four-quadrant data (since the majority of the articles used four-quadrant classification method), we used a modified method as previously described
.
RESULTS
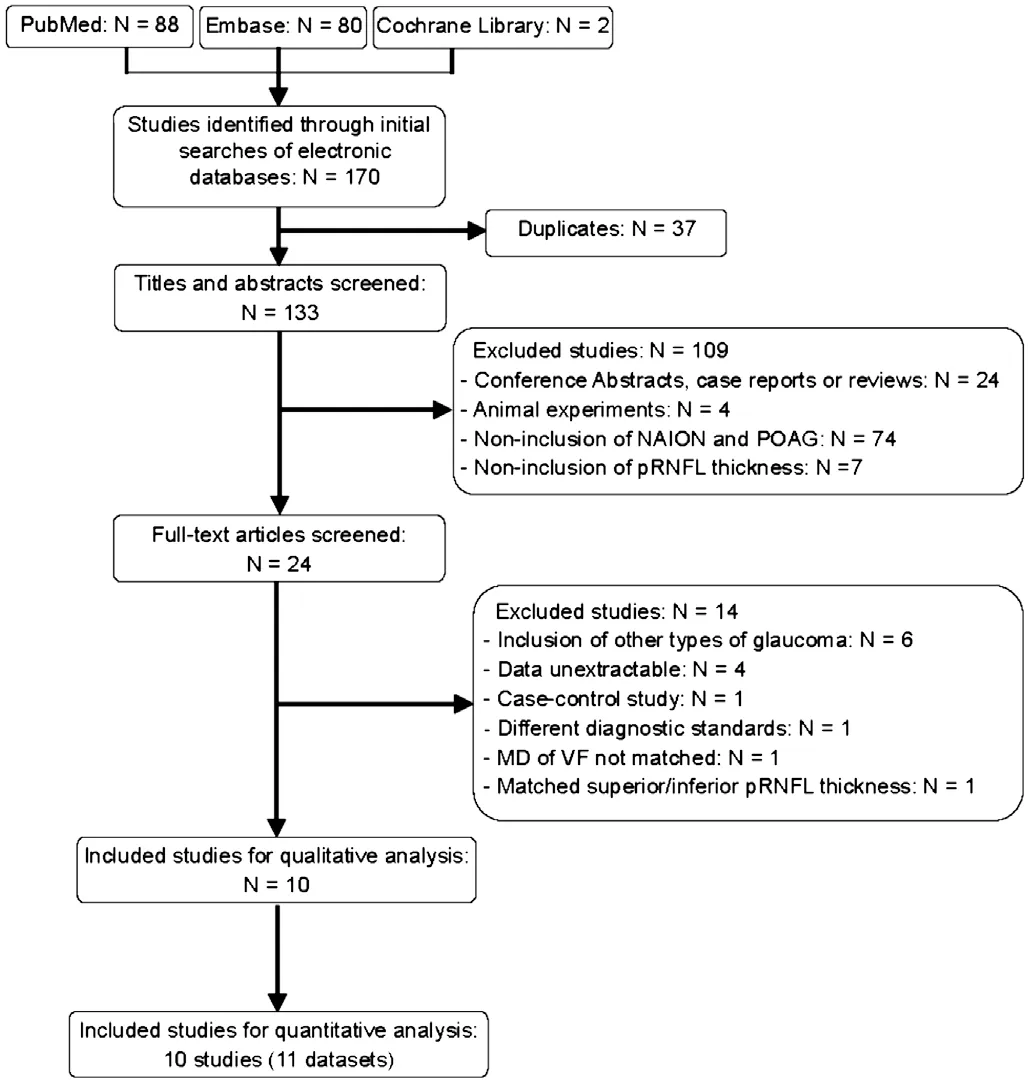
A total of 170 studies were initially identified, of which 37 duplicates were removed. Of the remaining 133 articles, 109 were excluded after screeningthe titles and abstract: 74 did not include NAION and POAG patients; 24 were conference abstracts, case reports, or reviews;seven lacked SD-OCT-based pRNFL thickness data; and four performed animal experiments. With full-text screening,another 14 studies were removed: six included other types of glaucoma rather than POAG, four reported unextractable data, one was a case-control study, one used different diagnostic standards, one included NAION and POAG with un-matched MD of VF, and one included NAION and POAG with matched superior or inferior pRNFL thickness. Thus, 10 eligible articles were included in the qualitative analysis, and 10 studies (11 datasets) were integrated in the quantitative analysis. A flow diagram of the literature search is shown in Figure 1.
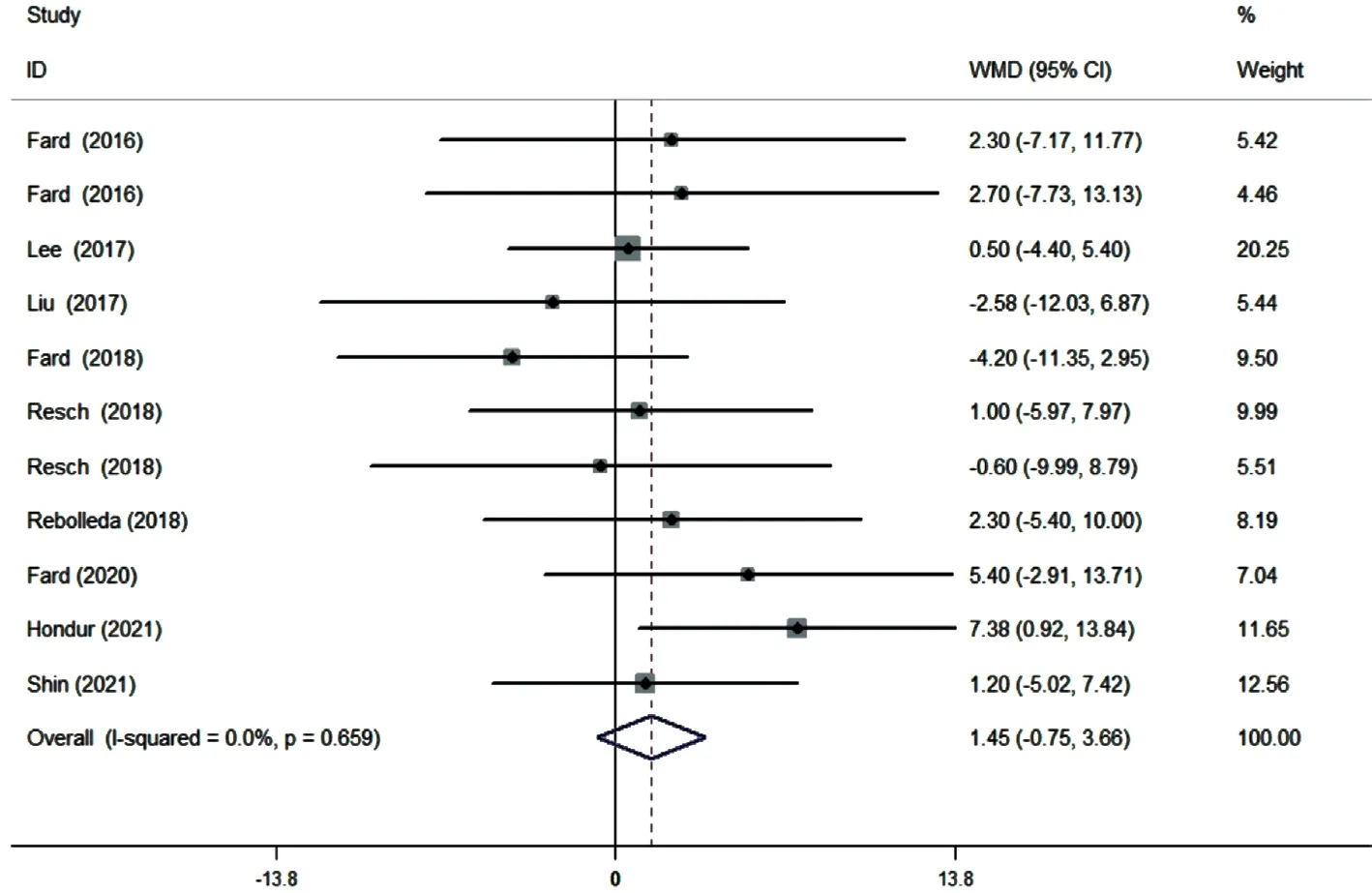
Ten studies (11 datasets) assessing the average pRNFL thickness showed no heterogeneity (
=0). The pooled results demonstrated that no difference in average pRNFL thickness between NAION and POAG eyes (WMD=1.45, 95%CI:-0.75 to 3.66,
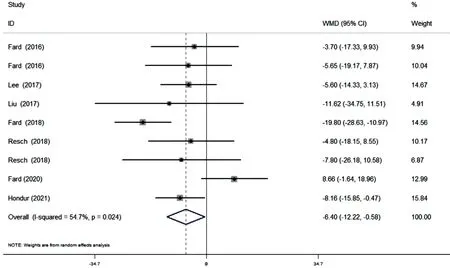
=0.196; Figure 2). However, eight studies(nine datasets) evaluating the sectoral pRNFL thickness demonstrated that the superior pRNFL thickness was significantly lower in NAION patients than in POAG patients(WMD=-6.40, 95%CI: -12.22 to -0.58,
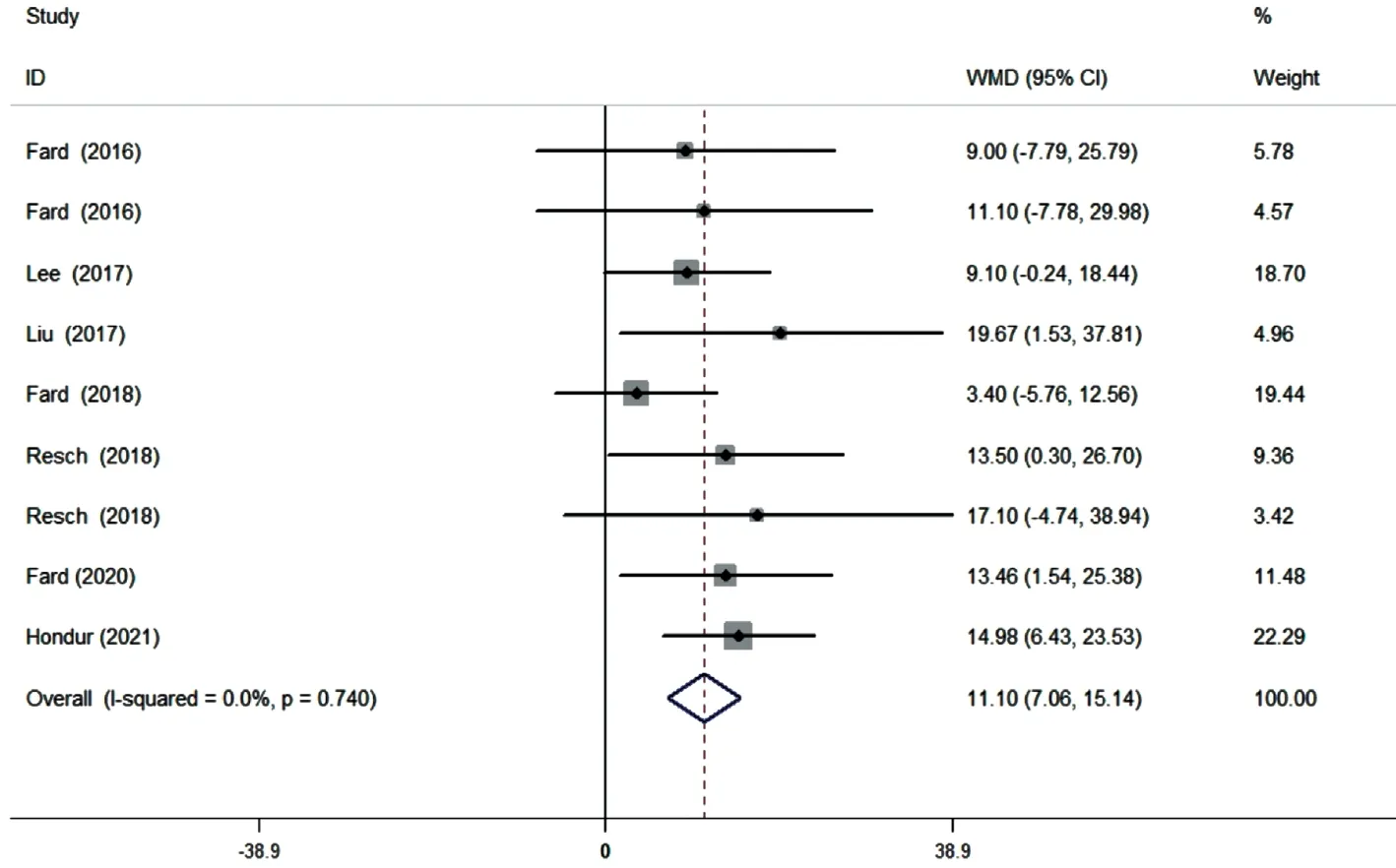
=0.031; Figure 3),whereas the inferior pRNFL was significantly thinner in POAG eyes (WMD=11.10, 95%CI: 7.06 to 15.14,
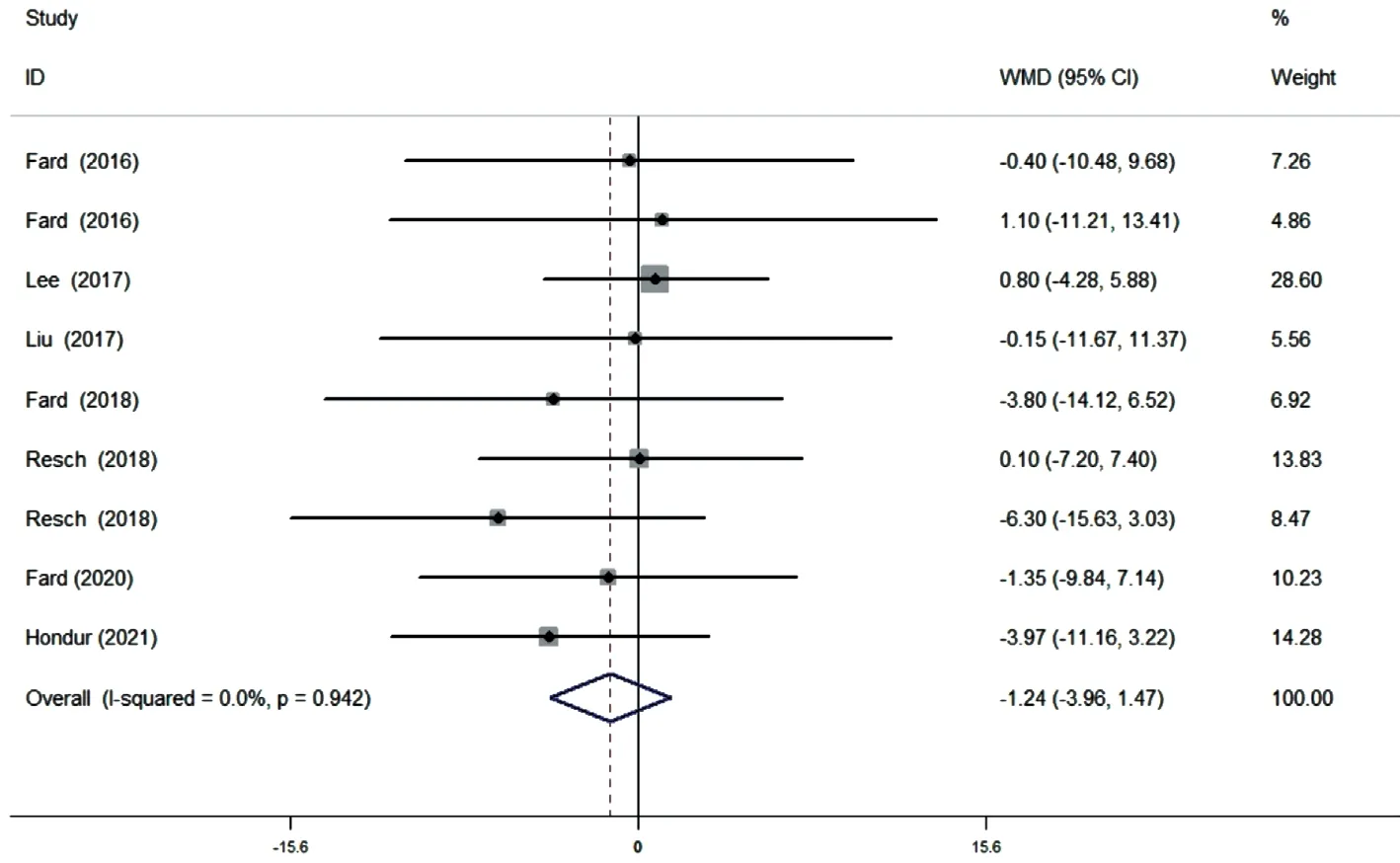
≤0.001; Figure 4).No difference in the nasal and temporal quadrants was found between NAION and POAG patients (nasal: WMD=-2.12,95%CI: -4.43 to 0.19,
=0.072; Figure 5; temporal: WMD=-1.24, 95%CI: -3.96 to 1.47,
=0.370; Figure 6).
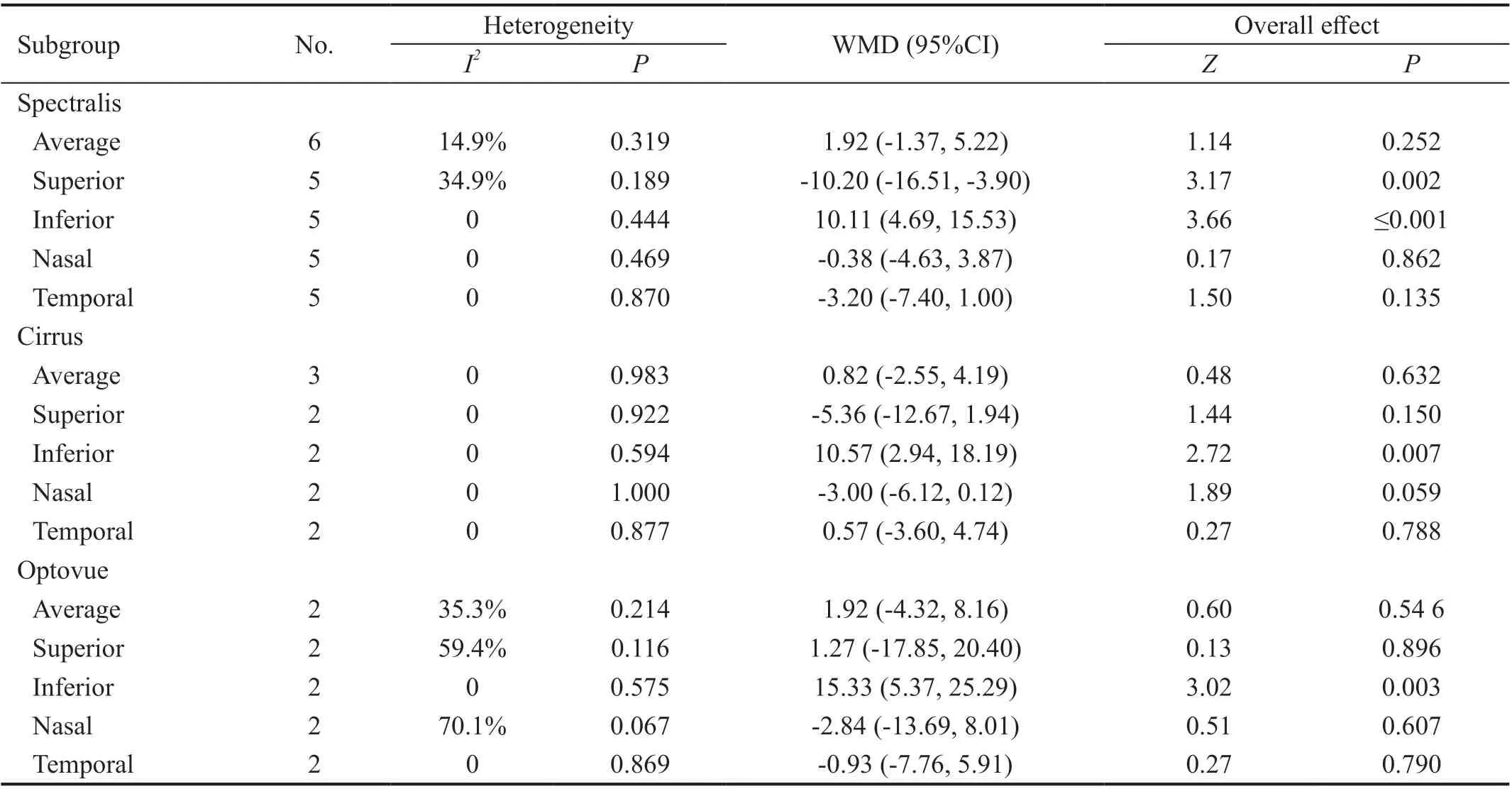
Stratified analysis according to the different types of SD-OCT(Table 4) also revealed that the inferior pRNFL was significantly thinner in POAG eyes when different SD-OCT devices were utilized (Spectralis: WMD=10.11, 95%CI: 4.69 to 15.53,
≤0.001; Cirrus: WMD=10.57, 95%CI: 2.94 to 18.19,
=0.007; Optovue: WMD=15.33, 95%CI: 5.37 to 25.29,
=0.003). The pooled results showed that the superior pRNFL was significantly thinner in NAION eyes than in POAG eyes when the Spectralis SD-OCT was used (WMD=-10.20,95%CI: -16.51 to -3.90,
=0.002), whereas no difference was demonstrated when Cirrus and Optovue SD-OCT were used (Cirrus: WMD=-5.36, 95%CI: -12.67 to 1.94,
=0.150;Optovue: WMD=1.27, 95%CI: -17.85 to 20.40,
=0.896).Similarly, no difference in the average, nasal, and temporal pRNFL thickness was indicated between NAION and POAG eyes regardless of SD-OCT type.
Ten included cross-sectional studies (11 datasets) comprising 625 eyes (278 NAION eyes, 347 POAG eyes) were published between 2016 and 2021 across different regions (Turkey, Iran,Spain, Austria, Korea, and Taiwan, China). The mean age varied from 54.1 to 68.6y in NAION patients and 53.75 to 72.3y in POAG patients. The pRNFL thickness was detected by using three types of SD-OCT devices: Spectralis, Cirrus,and Optovue. Most of the scan protocols were centered at the 3.4-3.5 mm circle around the ONH. Moreover, the MD of the VF was comparable between NAION and POAG eyes, and the majority of the included studies enrolled patients with moderate to severe POAG patients. The included studies recruited NAION patients with time from the onset of more than 3 or 6mo. The detailed characteristics are summarized in Table 1.
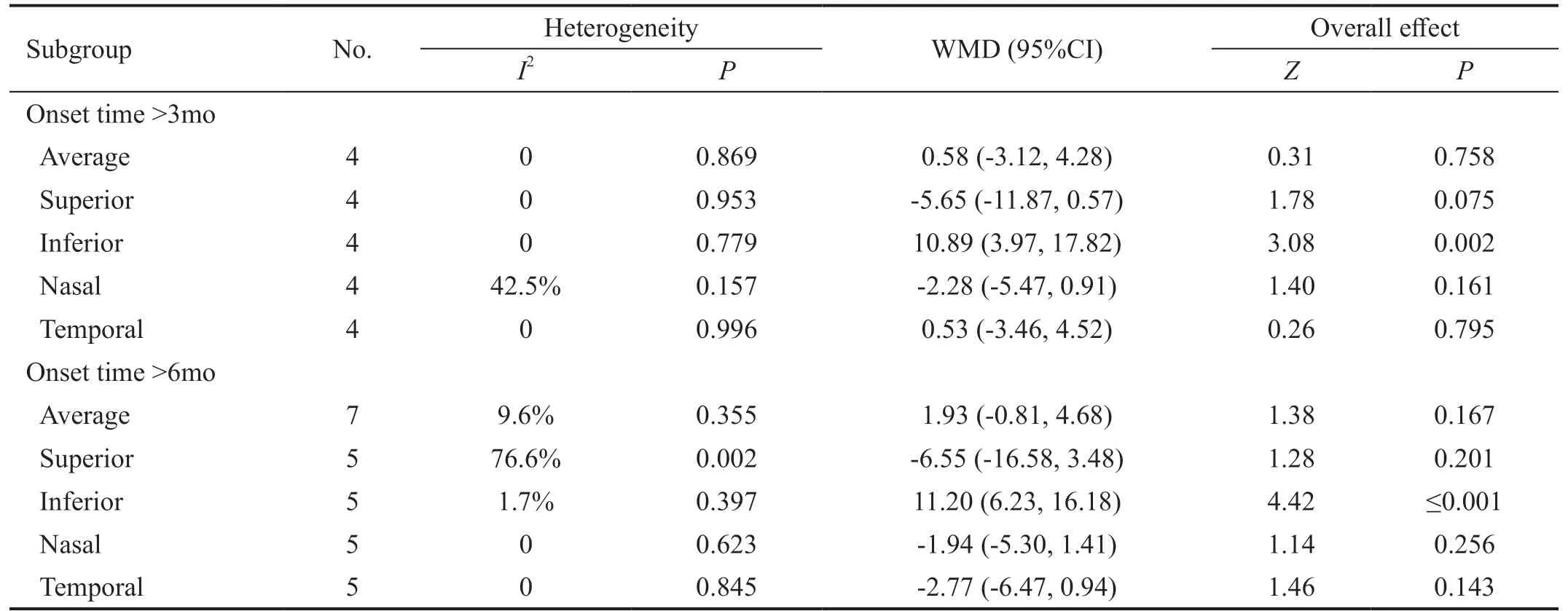
The subgroup analysis regarding the onset time of NAION (Table 3) also demonstrated that the inferior pRNFL thickness was significantly lower in POAG eyes than in NAION eyes (onset time >3mo: WMD=10.89, 95%CI:3.97 to 17.82,
=0.002; onset time >6mo: WMD=11.20,95%CI: 6.23 to 16.18,
≤0.001). However, in contrast to the combined pooled data, significant difference in the superior pRNFL thickness was not found between the NAION eyes and POAG eyes regardless of the onset time of NAION (onset time>3mo: WMD=-5.65, 95%CI: -11.87 to 0.57,
=0.075; onset time >6mo: WMD=-6.55, 95%CI: -16.58 to 3.48,
=0.201).Similarly, no difference in the average, nasal, and temporal pRNFL thicknesses was noted.
In terms of evaluating methodological quality, the AHRQ scores of all included studies were more than 3, indicating adequate quality (Table 2).

Results of Begg’s test and Egger’s test demonstrated no significant risk of publication bias in the average and sectoral pRNFL thickness (
>0.05; Table 5).
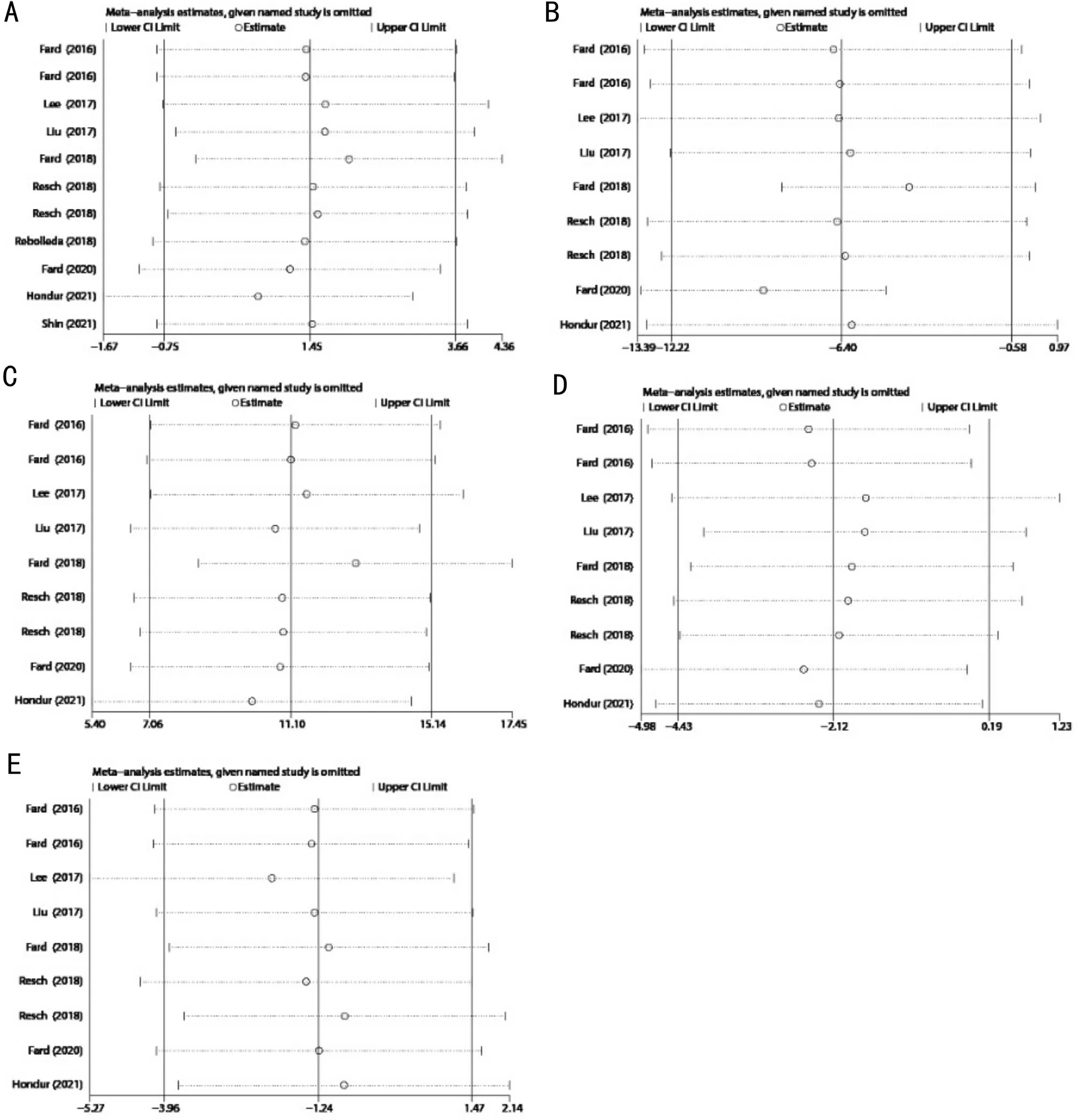
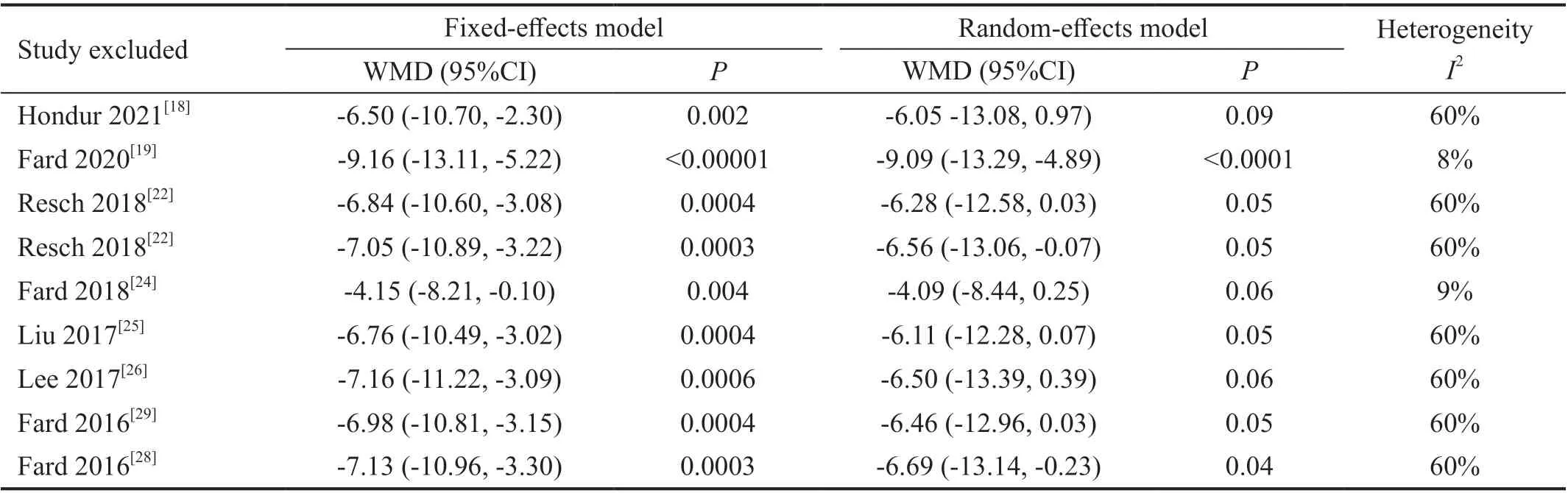
No obvious change in the results was noted after excluding each study (Figure 7), demonstrating the stability and reliability of our results. Two studies by Fard
were found to contribute most to the heterogeneity of the superior pRNFL thickness (Table 6).
DISCUSSION
In the present study, we pooled the average and quadrant pRNFL thickness in NAION and POAG patients. Our data demonstrated no significant difference in the average pRNFL thickness between the NAION and POAG eyes(
=0.196). This finding is consistent with those of previous studies
. Currently, POAG has been reported to be associated with multiple risk factors including race,age, elevated intraocular pressure, family history, myopia,and diastolic perfusion pressure,
. In glaucomatous neurodegeneration, the increase in intraocular pressure or imbalance of trans-laminar cribrosa pressure continuously stresses the RGCs and their supporting glia, leading to the progressive loss of RGCs and axons
. In contrast to glaucoma, NAION is presumed to be correlated with factors that can disrupt vascular autoregulation, such as nocturnal hypotension and other predisposed conditions such as smallto-disc ratio,
. Transient infarction of the anterior segment of the optic nerve nourished by the posterior ciliaryartery circulation also results in the deterioration of RGCs and axons
, where NAION may mimic POAG with regard to the average pRNFL thickness.

We included cross-sectional studies if they met the following requirements: 1) original article; 2) inclusion of NAION at the atrophic stage where optic disc swelling had to occur at least 3mo prior to the documentation and has resolved at the time of the study; 3)inclusion of both NAION and POAG with the same diagnostic standards; 4) inclusion of NAION and POAG with similar severities in terms of the MD of the VF; 5) inclusion of pRNFL thickness assessed by SD-OCT.
To clarify the sources of heterogeneity, we performed a“l(fā)eave-one-out” sensitivity analysis. No obvious change in the average and sectoral pRNFL thickness was observed after excluding each study, demonstrating that our data were stable and reliable. However, the results indicated that the two studies by Fard
(more deviated from the estimate line; Figure 7B) contributed to the heterogeneity mostly of the superior pRNFL thickness (
=54.7%). Nevertheless, heterogeneity was largely reduced after excluding these two studies separately(the heterogeneity dropped from 54.1% to 9% when we excluded Fard
; the heterogeneity dropped from 54.1%to 8% when we excluded Fard
).
The loss of pRNFL thickness is reported to reach a plateau at 6mo from the onset of NAION, and to be more correlated with VF at the atrophic stage
. Similarly, the pRNFL decreases rapidly in early-to-moderate glaucoma, showing a “floor effect” where the pRNFL decreases relatively slower in the advanced stage
. For this reason, we included most of the studies that enrolled POAG patients at moderate or more severe stages with comparable MD of the VF to ensure the similar severities in these diseases. However, pRNFL thickness is also shown to decrease slowly 3mo after NAION onset
.Based on these findings, we performed a subgroup analysis attributed by the time from the onset of NAION. Our pooled results indicated a significant decrease of inferior pRNFL thickness in POAG eyes compared with that in NAION eyes,regardless of the onset time (onset time >3mo:
=0.002; onset time >6mo:
≤0.001). Nevertheless, unlike the combined data of the superior pRNFL thickness (
=9), there was no significant difference between NAION and POAG eyes (onset time >3mo,
=0.075,
=4; onset time >6mo,
=0.201,
=5).This may be due to the sources of heterogeneity introduced by Fard
when patients were enrolled at 6mo from the onset,and the relatively small sample size of this subgroup (
=5).
根據(jù)商務(wù)英語專業(yè)跨境電商方向人才培養(yǎng)目標(biāo)和對行業(yè)企業(yè)的調(diào)研,在全面分析跨境電商崗位所需知識結(jié)構(gòu)和崗位技能的基礎(chǔ)上,我們提出基于職業(yè)素養(yǎng)的崗位基本能力、崗位核心能力和拓展能力構(gòu)建跨境電商方向的課程體系。
登錄APP查看全文
猜你喜歡
小學(xué)科學(xué)(學(xué)生版)(2021年7期)2021-07-28 06:44:32
小學(xué)科學(xué)(學(xué)生版)(2020年6期)2020-08-13 07:47:12
當(dāng)代陜西(2019年7期)2019-04-25 00:22:18
領(lǐng)導(dǎo)決策信息(2018年26期)2018-10-12 02:18:26
特別文摘(2016年19期)2016-10-24 18:38:15
37°女人(2016年5期)2016-05-06 19:44:06
爆笑show(2016年1期)2016-03-04 18:30:28
爆笑show(2015年6期)2015-08-13 01:45:40
文理導(dǎo)航·科普童話(2015年6期)2015-07-29 16:46:21
都市麗人(2015年5期)2015-03-20 13:33:49
 International Journal of Ophthalmology
2022年8期
International Journal of Ophthalmology
2022年8期
- International Journal of Ophthalmology的其它文章
- Advances in the research of plant-derived natural products against retinoblastoma
- Acute bilateral anterior uveitis in paediatric inflammatory multisystem syndrome temporally associated with COVlD-19
- Metamorphopsia as the first clinical sign of renal cell carcinoma
- Sutureless contact lens-type amniotic membrane for persistent epithelial defects after infectious keratitis
- A case of conjunctival intraepithelial neoplasia with spheroidal degeneration: a clinicopathological study
- Risk of anxiety and depression in patients with uveitis: a Meta-analysis