Efficacy of gabapentin for low back pain at a tertiary hospital: A prospective observational study
2022-07-02 05:53:00NavaneethaKrishnanSubramanianVVRameshChandraKarthikeyanElumalaiNarahariPaleiTiruveediKusumaVadlamuriVenkataPrasadYellantiBalaVenkataBhargavPhaniMungaraYeshwanthSaiPradeepBattulaAnnaBalaji
Journal of Acute Disease 2022年3期
Navaneetha Krishnan Subramanian, VV. Ramesh Chandra, Karthikeyan Elumalai, Narahari N Palei, Tiruveedi Kusuma, Vadlamuri Venkata Prasad, Yellanti Bala Venkata Bhargav Phani,Mungara Yeshwanth Sai, Pradeep Battula, Anna Balaji
1Department of Pharmacology, Dr. Kalam College of Pharmacy, Periyanayagipuram 614623, India
2Department of Neurosurgery, Sri Venkateswara Institute of Medical Sciences, Tirupati 517102, India
3Faculty of Pharmacy, Bharath Institute of Higher Education and Research, Selaiyur 600073, India
4School of Pharmacy, the Neotia University, Sarisha 743368, India
5Department of Pharmacy Practice, Sree Vidyanikethan College of Pharmacy, Tirupati 517102, India
6Departments of Pharmacy Practice, Santhiram College of Pharmacy, Nandyal 518501, India
7Departments of Pharmaceutics, Sree Vidyanikethan College of Pharmacy, Tirupati 517102, India
ABSTRACT
KEYWORDS: Gabapentin; Low back pain; Sleep; Pittsburgh Sleep Quality Index; Visual Analogue Scale
1. Introduction
Low back pain (LBP) has emerged as a serious health and socioeconomic issue, as well as cause of disability and productivity loss. Most of the population experience LBP at some point of time in their lives[1]. In the area of evidence-based medicine, global researches focus on new therapeutic modalities, both conservative and surgical[2]. A PubMed search of “LBP” returned 193 665 articles, of which one-third have emerged in the past 5 years.
According to the Global Burden of Disease Study 2016, LBP is the highest on record of years lived with disability (YLD), accounting for 57.6 million (40.8-75.9 million) of total YLDs, due to an aging and growing global population. LBP has increased by more than 50% in low- and middle-income countries since 1990. Back and neck discomfort is the second major cause of YLD in India, after iron deficiency anemia[3]. According to reports, the estimated prevalence of LBP in India ranges between 42% and 83%[4,5]. Ganesan et al.recently reported LBP prevalence in young Indian people aged 18 to 35 years as 42.4% per year and 22.8% per week[6]. Medications that are widely used to treat LBP include muscle relaxants, non-steroidal anti-inflammatory drugs, opioid analgesics, anti-depressants, and systemic steroids either used alone or in combination. Physical modalities, rehabilitation methods, and spinal manipulation are among other alternative treatments. When all other options have been exhausted, surgery is sometimes the final resort, and the results might be poor. So more recent focuses shift towards conservative care rather than surgical treatment[2]. Gabapentin is an anti-seizure drug that was first developed and approved as adjunctive therapy for the treatment of partial seizures. It is now often used to treat neuropathic pain. It is a gamma-aminobutyric acid analog that binds to the α2-δ site of voltage-dependent calcium channels, decreasing neurotransmitter release[7]. A high number of LBP patients are treated with conventional analgesic medicines with poor outcomes,prompting regular exploration of second-line alternatives, including gabapentinoids. Gabapentin is commonly recommended for chronic back pain syndromes in both primary care and specialty pain clinics,especially when the pain radiates into the upper or lower legs[8,9].In India, very few studies have been done concerning this issue.With this in mind, the goal of this research is to assess the safety and effectiveness of gabapentin in LBP patients.
2. Patients and methods
2.1. Study design
This prospective observational study was undertaken to study the effectiveness of gabapentin in the treatment of LBP over 6 months,this self-funded study was done from February 2021 to August 2021.

Figure 1. The study flowchart. LBP: Low back pain; VAS: Visual Analogue scale; PQSI: Pittsburgh sleep quality index.
2.2. Inclusion and exclusion criteria
Patients who were over 18-year-old had been diagnosed with conservative LBP as outpatients, and were willing to participate in and adhere to therapy were included in this study.
Patients who underwent surgery, pregnant women, lactating women,and those below 18 years of age were excluded from this study.
2.3. Data collection
The patients’ data were collected using a pre-designed structured data collecting form. The data collection form includes patient sociodemographic information and past medical history. The impact of gabapentin on patient pain management is based on Visual Analogue Scale pain scores; there are five levels of pain: mild 1-3, moderate 4-6, severe 7-9, excruciating pain 10, and no pain zero. The effects of gabapentin on the Pittsburgh Sleep Quality Index (PSQI) score were broadly divided into four categories, such as very good 0-5, fairly good 6-9, fairly bad 10-14, and very bad 15. Therapy, the pain and sleep scores were recorded before and after therapy, and a follow-up was performed three weeks later. The follow-up was completed in the last 2 months of the study duration.
2.4. Ethical statement
All the procedures followed in this study were per institutional ethical standards. The institutional ethics committee granted ethical clearance,and the IEC No: 1093 was acquired from the same study site, and consent was secured.
2.5. Statistical analysis
We assumed a standard deviation shift of 9.9 on the Oswestry Disability Index and a clinically significant difference of 8.012 on the Oswestry Disability Index. The sample size was determined as 90 patients at a 5%level of significance and an 80 percent power of a test,βof 0.2. An extra 10% was added to compensate for patients who were lost to follow-up. As a result, the sample size was determined to be 100 patients.
Microsoft Excel 2016 was used. Arithmetic meaning and standard deviation were used to present numerical variables, while frequencies were used to present descriptive variables. Adjusted Chi-square test was applied to compare categorical data between the two groups, while paired t-test was used to compare numerical data between the two groups[9,10]. The significant level of this study was set at α=0.05.
3. Results
3.1. Socio-demographic details
All 100 patients who agreed to take part in the study were given questionnaires in the Out-patient Ward of the Neurosurgery Department (Figure 1). Sixty-five patients were females, while 35 patients were males. The patients’ mean age was (39.0±10.5) years,with the majority falling between 36 and 45 years. The majority of surveyed patients worked 8 to 12 h per day (40%), 81% were married, and 69% were employed. The majority of LBP patients(63%) followed Hinduism; the majority of patients (41%) had some university education, and they were primarily from urban areas (58%). The non-radiating LBP was predominant accounting for 40%, with the remaining radiated LBP concentrated in the right lower limb of 30%, the left lower limb of 10%, and both of 20%.The characteristics of the participants are shown in Table 1.

Table 1. Patients characteristics.
3.2. Impact of gabapentin on pain management and quality of sleep score
The pain score was reduced for all LBP patients after gabapentin administration (χ2=59.08, P<0.001), and 32 patients reported no pain (Table 2). Sleep quality was significantly improved in the majority of the gabapentin-treated patients (P<0.001) (Table 3).
3.3. Effect of gabapentin on overall pain and sleep score assessments
The mean sleep score before using gabapentin was 10.95±5.02 and the mean sleep score after using gabapentin were 4.90±2.20,and the difference was significantly different (t=14.25, P=0.001).And before gabapentin, the mean pain score was 7.70±1.91,whereas, after gabapentin, the mean pain score was 2.75±1.79, and the difference was significantly different (t=27.08, P=0.001).
3.4. Assessment of LBP patients’ satisfaction after gabapentin therapy
The results indicated that 62% patients were strongly satisfied after using gabapentin and no side effects or adverse reactions occurred; 31% patients were just satisfied and 7% patients were strongly dissatisfied with the gabapentin therapy.
4. Discussion
Beginning at a young age, LBP could reduce quality of life[10]. The mean age of onset is 39.10 years, with people in their third and fourth decades of life falling mostly between the ages of 35 and 45. This may be due to obesity, a heavy workload, and poor posture. The findings agree with those of Rishabh et al., who reported that LBP is most common in the third and fourth decades of life[11,12].
The prevalence of LBP is higher in females (65%) as compared to in males (35%). Our findings are consistent with those of Linton et al. and Thomas et al., who found that chronic backache has a higher incidence in females than in males[13,14]. Hoy et al. found a higher prevalence of LBP in females in a meta-analysis[15]. In the study, the majority of patients (41%) worked for 8-12 h a day, most were homemakers(81%), and had a university education (41%). Excessive working hours, poor working posture, and physical exhaustion are all possible causes[16,17]. Furthermore, the findings are consistent with Nazeer et al. who conducted an epidemiological study and found that housewives constituted the majority of cases[18].

Table 2. Pain status of low back pain patients.
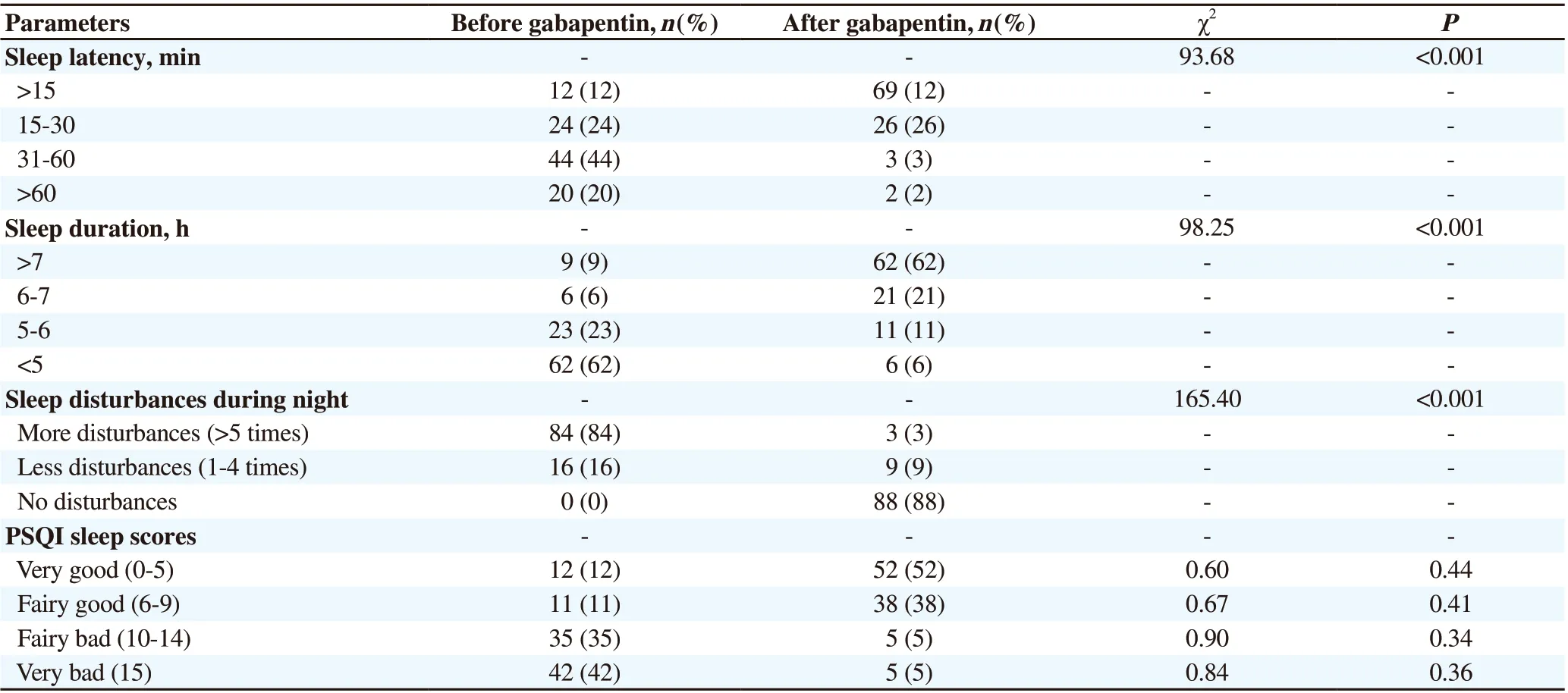
Table 3. Quality of sleep of the patients before and after gabapentin treatment.
In the current study, most of the patients were employed (62%). The findings were also supported by Weiner et al. and Goumeoens et al.Occupational LBP has a complex etiology, as well as a high incidence and prevalence. Occupational LBP affects the economically active population. It leads to work incapacity, costs associated with lost productivity, days off work, medical and legal expenses, insurance payments for invalidity, and social security. It should be considered not only as a medical issue but also as a social and economic problem[19,20].
Most of the patients were urban residents (58%) and were Hindu community members (63%). The level of urbanization in our study has some relation to LBP based on a previous study[21]. The Hindu religion is predominantly followed in India. As a consequence, more Hindu religious individuals (63%) attended the hospital and were diagnosed with LBP than other religious people, which might be ascribed to the fact that more Hindu populations lived in the study areas. Gabapentin,an anticonvulsant, was prescribed to all patients to evaluate pain scores and quality of sleep. Gabapentin improves sleep efficiency by enhancing slow-wave sleep[22] and decreasing sleep awakenings[23].Gabapentin could reduce spontaneous arousals during sleep and episodes of wakefulness after sleep onset[24].
Our study found that gabapentin can improve the quality of life in patients with neuropathic pain, as well as pain scores and pain-related sleep interference. Before gabapentin treatment, the mean pain score was 7.70±1.91, whereas after the treatment, the mean pain score was 2.75±1.80, and the difference was significantly different (t=27.08,P=0.001). Our study is in agreement with a study by Kapustina et al.[25]. However, different results were reported by Enthoven et al., and their study found that there were no differences in pain intensity after using NSAIDs in the treatment of LBP[26]. In our study, out of 100 patients, 62% of patients were strongly satisfied after using gabapentin for LBP with no side effects or adverse reactions and the rest 31% of patients were just satisfied and 7% of patients were strongly dissatisfied with the therapy. In patients with LBP, gabapentin demonstrated significant symptomatic pain relief and improved sleep quality.Simultaneously, the healthcare professional team should be aware of the dangers of misusing gabapentin and should be able to assist in optimizing gabapentin therapy while minimizing side effects[27].During the whole study, no single patient complained of any adverse reactions due to the usage of gabapentin.
The current study has some limitations. First, patients were only followed up for a small duration. Second, the sample size was small to deduce the significance. Finally, we were unable to get individuals who had surgery for LBP to achieve satisfactory outcomes.
To sum up, gabapentin can improve sleep quality and reduce lower back pain as measured by the VAS and PQSI. The efficacy of this drug is relatively good, but further improvement is required.
Conflict of interest statement
The authors report no conflict of interest.
Funidng
This study received no extramural funding.
Authors’ contributionsN.K.S. and V.V.R.C. prepared the protocol and wrote the article.K.E., T.K., and N.N.P. also contributed to the literature search and data collection. V.V.P., Y.B.V.B.P., M.Y.S., and P.B. did the biostatistical analysis. A.B. supervised the whole project.
 Journal of Acute Disease2022年3期
Journal of Acute Disease2022年3期
- Journal of Acute Disease的其它文章
- A rare fatal case of rabies coexisting with COVID-19
- Ophthalmovigilance in COVID-19: Retinal vascular occlusion
- Lymphocyte count and A-DROP score in COVID-19 patients: A retrospective observational study
- Knowledge, attitude, and practice of house officers towards COVID-19: A multicentered crosssectional study in Egypt
- Comparison of impact of adjuvant treatment of midazolam, fentanyl, and magnesium sulfate with intrathecal bupivacaine on block characteristics and postoperative analgesia in knee arthroplasty: A randomized clinical trial
- Efficacy of propofol versus ketamine in modified electroconvulsive therapy: A prospective randomized control trial