Ankylosing spondylitis complicated with andersson lesion in the lower cervical spine:A case report
2022-06-23 02:06:50YuJianPengZhuangZhouQianLiangWangXiaoFengLiuJunYan
World Journal of Clinical Cases 2022年11期
lNTRODUCTlON
Andersson lesion (AL) are characterized by nonneoplastic bone destruction, which is an uncommon phenomenon in late-stage ankylosing spondylitis (AS) and often appears as erosive focal changes with sclerosis widely distributed in the region of the vertebral end plate[1,2]. The prevalence of ALcomplicating AS ranges from 1.5% to > 28%[3,4]. With the development of AL, these pathological and destructive changes of the spine may lead to progressive, localized and pain-intolerable kyphosis deformities and even neurological defects, which must be treated in severe cases[5,6]. AS is a chronic active nonunion state with unstable posterior column fractures or unfused facet joints associated with vertebral lesion[7]. Since nonspecific inflammation is the main pathological manifestation, Andersson lesion commonly occur in the region of the thoracic and lumbar spine but rarely in the cervical spine[8].We successfully treated a patient with nonneoplastic and noninfectious bone destruction of the C6 vertebral body, who had a history of ankylosing spondylitis for decades, which resulted in nonunion involving the middle and posterior columns, characteristics of an Andersson lesion. To the best of our knowledge, this is the first report of unstable fractures of AS with C6 aggressive bone destruction and accumulation of three columns of the cervical spine.
CASE PRESENTATlON
Chief complaints
A 78-year-old male farmer was admitted to our hospital with neck pain, worsened numbness and increased disability due to an accidental fall a month prior. He had neck pain and a limited range of motions, but he had no symptoms of fever, night sweats or increased nocturnal pain.
History of present illness
This patient had a history of AS and mobility impairments for decades. He had progressive symptoms of neck pain for 3 mo complicated with left upper limb pain and numbness without obvious cause.
History of past illness
He had no history of diabetes, tuberculosis or tumour. He had undergone thoracolumbar fracture surgery more than ten years ago.
The second stood still and looked at him from head to foot, but then she said, How can I accept a husband who no longer has a human form? The shaven bear that once was here and passed itself off for a man pleased me far better, for at any rate it wore a hussar s dress and white gloves
Personal and family history
In summary, AL constitutes a relatively infrequent nonneoplastic bone destruction in patients with AS.Our report provides a meaningful reference for the diagnosis, differential diagnosis, treatment and prognosis of AL. Surgery is a more reasonable choice to treat AL with unstable cervical fracture,especially for patients with kyphosis and dysfunction caused by nerve compression. Fusion is critical,and complete decompression is fundamental in the treatment of Andersson lesion.
Physical examination
“There is a very wonderful bird mentioned here, called a nightingale,” said the emperor; “they say it is the best thing in my large kingdom. Why have I not been told of it?”
Laboratory examinations
Routine blood analysis revealed a slight increase in the neutrophil ratio (77.4%) with normal haematocrit and leukocyte counts. Prothrombin and partial thromboplastin times were almost normal,and d-dimers were increased at 1.56 μg/mL. Serum C-reactive protein was increased at 55.6 mg/dL(normal range <10 mg/dL). The blood serum tumour marker analysis showed that ferroprotein increased at 516 ng/mL (normal range 30-400 ng/mL), and prostate-specific antigen marginally increased to 8.53 ng/mL (normal range < 4 ng/mL).
Imaging examinations
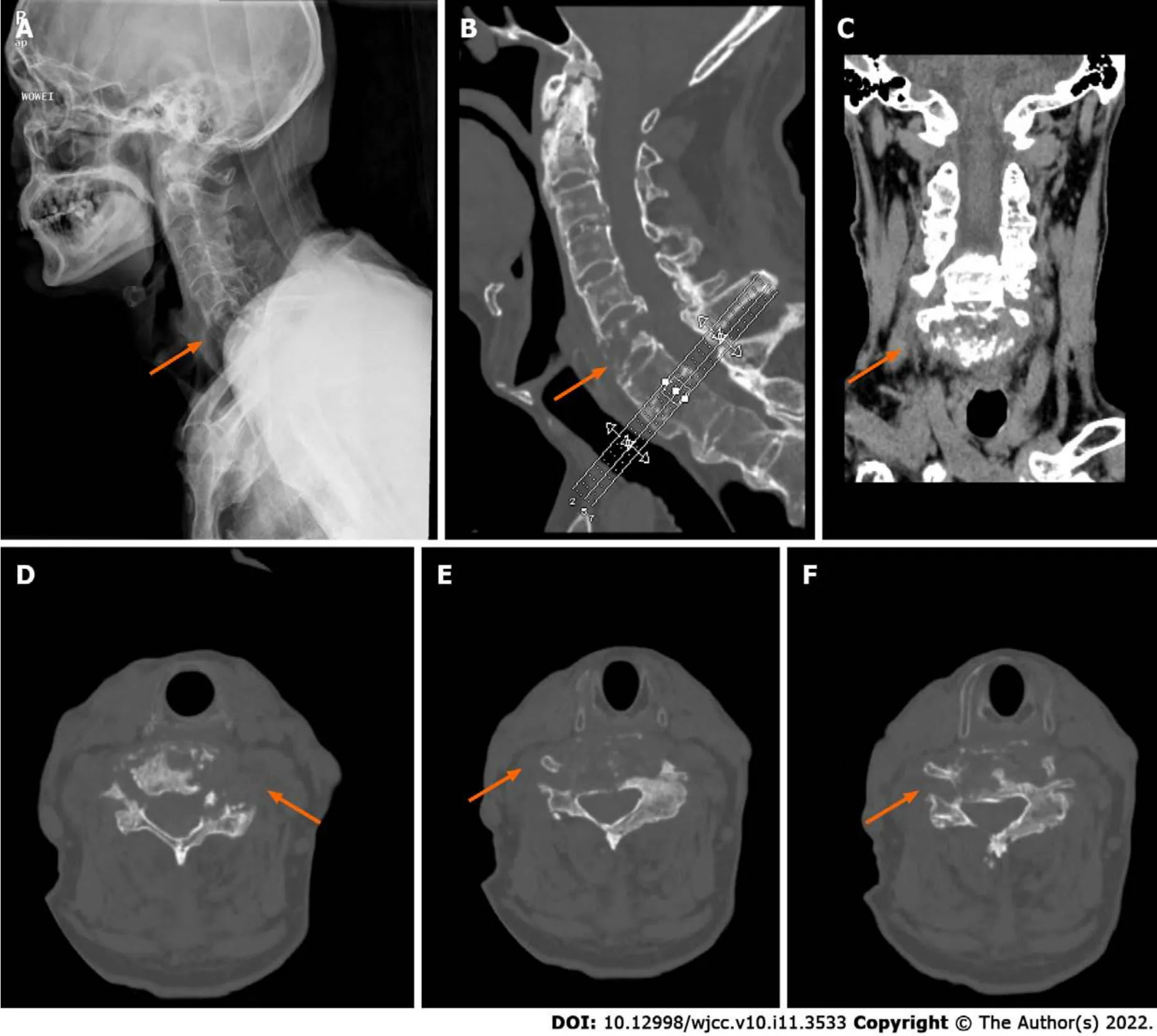
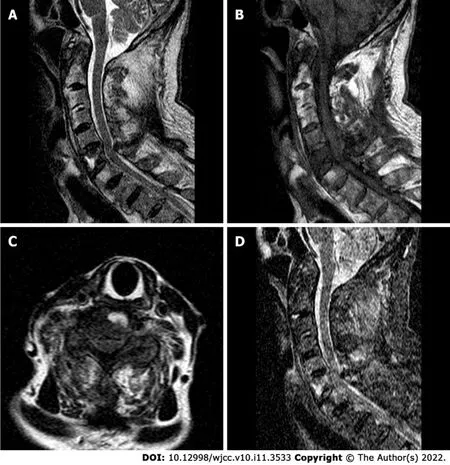
Radiography and computed tomography (CT) scans revealed typical ankylosing spondylitis in the entire spine,, bamboo-like changes; a pathological fracture changed from the C6 vertebra and accumulated at the upper and lower endplates to spinous processes (Figure 1). Magnetic resonance imaging (MRI) showed C6 new-onset vertebral compression fractures and oedema spread from the anterior region of the C6 spinal centrum to the spinous process and supraspinous ligaments, which were complicated by the degenerative cervical instability and compression of the spinal cord due to the injured cervical spinal stenosis (Figure 2).
FlNAL DlAGNOSlS
The final diagnosis of the presented case was Andersson lesion in the lower cervical spine.
TREATMENT
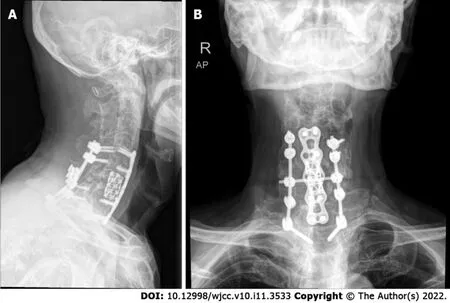
The patient underwent surgery for instrumented stabilization through anterior combined posterior approaches. First, the patient's body temperature was normal throughout the examination. Second, he was convinced that he had no history of tuberculosis or malignant visceral tumours, and all tuberculosis-related laboratory tests or tumour markers were negative. To restore cervical stability, we performed a combined posterior and anterior fixation approach with pedicle screws under a C-arm perspective (Figure 3). In brief, after exposure of C4-T2 with a posterior midline incision, part of the C5 and C6 Laminae were removed using an ultrasonic osteotome; the structure in the spinal canal was exposed, and posterior spinal canal decompression was completed. Under the guidance of C-arm fluoroscopy, the lateral mass or pedicle screws (8 in total, brand:Medtronic) were placed after positioning, drilling and sounding on the side mass of C4, C5 and C7 and the pedicle of T2; a connecting rod (Brand:Medtronic) was used to connect the fixing screws. Next, anterior surgery in the supine position was performed to expose the C6 vertebral body. Under the microscope, the C6 vertebral body and the upper and lower endplates were scraped with a curette. Then, we removed the granulation tissue for pathological examination and bacterial culture, and a short titanium mesh (Brand:Medtronic)was used to support and fix between the C5 Lower endplate and the C6 residual vertebral body.Anterior cervical plates and screws (Brand:Medtronic) were placed in front of C4-T1. To prevent screw loosening caused by osteoporosis, we used bone cement to strengthen the nail channels.
OUTCOME AND FOLLOW-UP
Based on the imaging findings for this patient, AL might be easily misdiagnosed for spinal tuberculosis or spinal metastasis because these conditions are mostly identified by bone destruction. In addition, both AL and spinal tuberculosis may be characterized by the narrowed intervertebral space,hyperosteogeny and late sclerosis[13]. Unlike AL, most patients with spinal tuberculosis have low fever,night sweats and other systemic symptoms in the early stage, and the anti-tuberculosis treatment is effective. Similarly, patients with spinal metastases often have symptoms in primary organs, such as gastrointestinal tumours and prostate cancer. Spinal metastases are common in the thoracolumbar spine, and cervical metastases are rarely reported. With detailed physical examination and previous AS
DlSCUSSlON
Andersson first described the characteristics of destructive lesion of the vertebral body and/or intervertebral disc in patients with ankylosing spondylitis in 1937[8]. Since then, they have been known as Andersson lesion, spondylodiscitis, spinal pseudarthroses and destructive spondylopathy[9,10]. This uncertainty in the naming of AL is mainly due to the lack of consistency in the ethology and pathology of the characteristics of these lesions. To date, two mainstream possible mechanisms have been reported.First, these lesions are considered to have a chronic nonspecific inflammatory nature and are attributed to the disease characteristics of ankylosing spondylitis. The other explanation is that they originate from traumatic injury and are characterized by constitute mechanical stress fracture, spinal nonunion or pseudarthroses after trauma[11-13]. Generally, the entire spine of patients with ankylosing spondylitis is susceptible. However, clinically, the most common site of this lesion is the thoracic and lumbar spine,especially the thoracolumbar transition area,T10-L2, possibly since this area is defined as the transition area of high stress in anatomy and biomechanics[14-16].
Previous reports on AL mainly involved the thoracic vertebrae and lumbar vertebrae regions, but there were almost no reports of AL in the cervical vertebrae. This is the first study to show nonneoplastic destructive lesion in the lower cervical vertebrae and the induction of cervical trauma injury.
This patient had a recent history of trauma, and the destructive lesion in the C6 vertebra was almost consistent with the characteristics of imaging, pathology and biomechanics of the Andersson lesion(bone destruction caused by chronic compression). Thus, we suspected that these unstable lower cervical spine fractures resulted from trauma with Andersson lesion, although the location was different from that previously reported (mainly in the thoracic and lumbar vertebrae). Most AL patients have been middle-aged and elderly men with or without AS symptoms for decades. The common clinical manifestations are local intolerable and progressive pain of the thoracolumbar spine and local severe pain after mild trauma with dysfunction[12].
Physical examination revealed a restricted cervical range of motion. The muscle power of the left upper limbs was grade IV with slightly decreased sensation. The Hoffman signs of both upper limbs were negative, and bilateral Babinski signs were negative in the lower extremities.
Then I spotted11 a broomstick standing12 in the kitchen corner. Maybe I could make a costume, I thought. Outside, a sheet and pillowcase billowed on the clothesline. I could be a witch or a ghost. Then my gaze fell on the back of the cellar door. My father s old plaid work shirt, faded overalls13, jacket and cap were hanging right where he had left them.
When combined with spinal cord nerve injury, some patients have serious symptoms such as numbness, muscle weakness, incomplete paralysis or even paraplegia. X-ray examination can preliminarily detect the degree of erosive bone destruction. Computed tomography is more accurate and stereoscopic than X-ray in displaying bone lesion, especially in assessing the location of spinal cord compression, the involvement of the spinal canal, the severity of vertebral destruction and the injury mechanism. In addition, MRI can provide information about the involvement of soft tissue around the spine, and the state of the spinal cord and nerve is clearer.
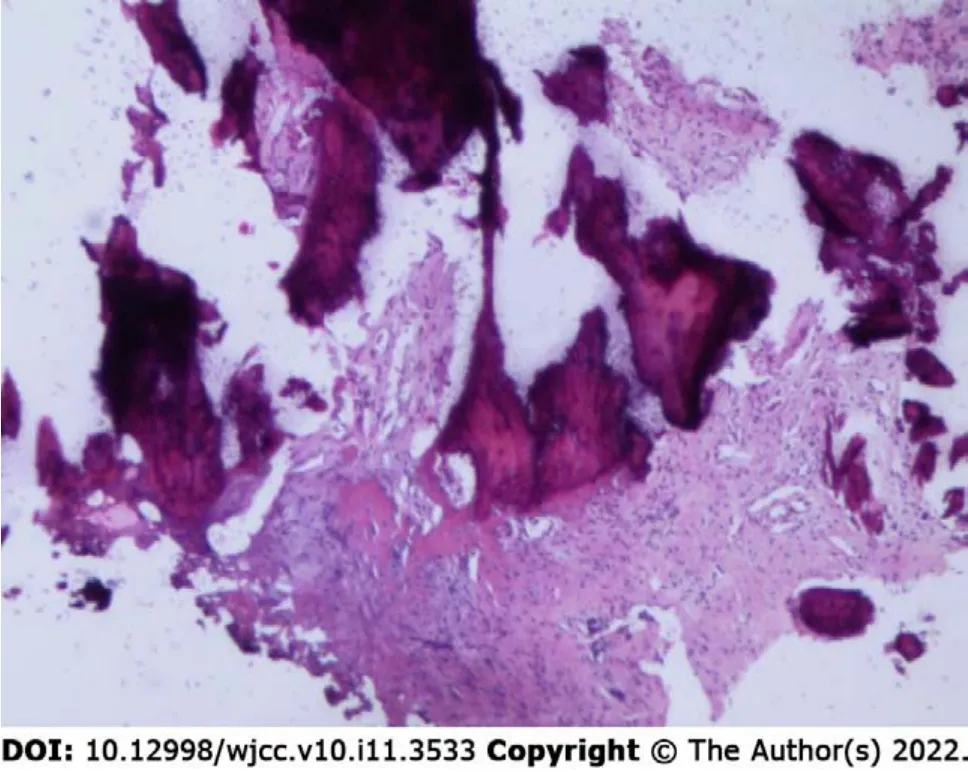
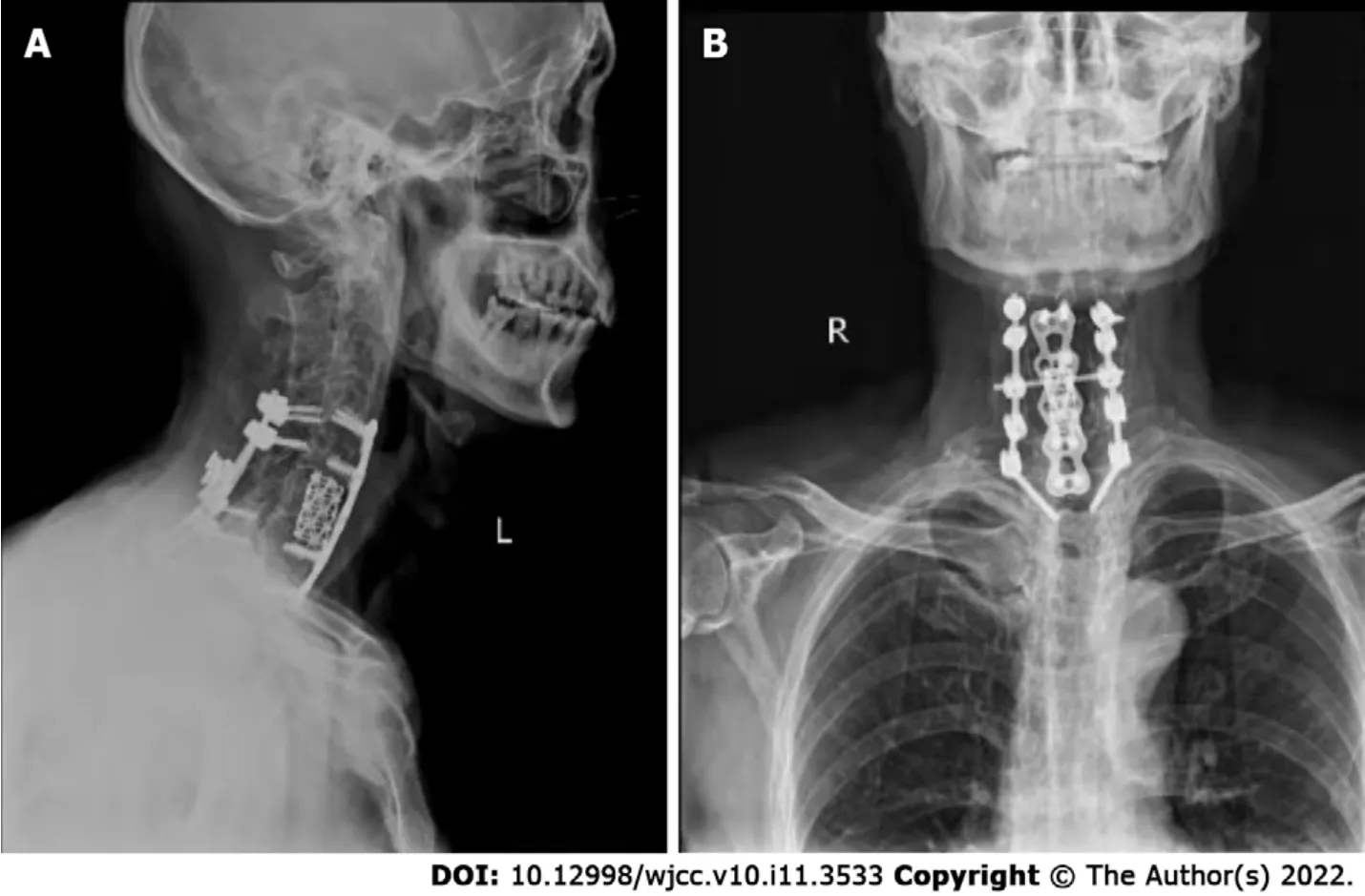
The operation was very successful, and the pathology indicated hyperplastic and fibrous bone tissue with dead bone reaction with no indications of tumour cells and negative bacterial culture results(Figure 4). A postoperative double-check CT scan revealed that the internal fixation device was firm and reliable, and the stability of the cervical spine recovered well. Six months after the operation, the patient reported that the symptoms of pain and numbness were notably relieved and almost returned to normal. The follow-up X-ray images of the cervical spine AL showed that the balance of the coronal plane and sagittal plane recovered well (Figure 5).
One slipper3 was nowhere to be found; the other had been laid hold of by an urchin5, and off he ran with it; he thought it would do capitally for a cradle when he some day or other should have children himself. So the little maiden6 walked on with her tiny naked feet, that were quite red and blue from cold. She carried a quantity of matches in an old apron7, and she held a bundle of them in her hand. Nobody had bought anything of her the whole livelong day; no one had given her a single farthing.3
I was such a fine gentleman, so stiff with starch4! I had a boot-jack and a hair-brush, which I never used! You should just have seen me then! Never shall I forget my first love! She was a girdle, so delicate and soft and pretty! She threw herself into a wash-tub for my sake! Then there was a widow, who glowed with love for me
To the best of our knowledge, there are no exact and consistent guidelines on how to systematically treat AL[17]. Conservative treatment, including NSAIDs and anti-TNF-α therapy, is often initially suggested, and some researchers have confirmed that conservative treatment is safe and effective[8].Nevertheless, there is still no recognized evidence that these drugs can help the treatment of symptomatic AL, although they have been proven to be effective in patients with ankylosing spondylitis. Therefore, surgical treatment is recommended to reduce unbearable pain, kyphosis deformity, biomechanical instability or neurological deficits caused by trauma[18-21]. Our patient had a mild traumatic fracture involving three columns of the cervical spine secondary to Andersson lesion. To reconstruct the stability of the cervical spine and fully decompress the spinal canal, we chose the posterior with the anterior approach for surgery. According to our experience, successful interbody fusion through surgery (one-stage internal fixation) is the safest and most effective choice to treat AL.
CONCLUSlON
The patient denied family history.
disease history, laboratory markers, X-ray, CT and magnetic resonance examination are vitally important for the diagnosis of AL.
He stood looking at her, and when he had looked for some time, he said: Let that be enough, wife, now that you are king! Now we have nothing more to wish for
Peng YJ performed the study, collected data, and drafted the manuscript; Zhou Z and Wang QL collected data, performed literature searches and interpreted the data; Liu XF and Yan J made critical revisions to the manuscript; all authors have read and approved the version of the article presented for publication
the National Natural Science Foundation of China, No. 81902239 and the Natural Science Foundation of Jiangsu Province, No. BK20191169.
Written informed consent was obtained from the patient for the publication of this case report and the accompanying images.
The authors have no conflicts of interests to disclose.
He has eaten our children and sleeps after it; he must die, said the father-bird, and flew back to the hills and clawed up a huge stone which he meant to let fall on the prince s head
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See:https://creativecommons.org/Licenses/by-nc/4.0/
China
Yu-Jian Peng 0000-0001-6927-6599; Zhuang Zhou 0000-0002-9050-2578; Qian-Liang Wang 0000-0002-0785-2594; Xiao-Feng Liu 0000-0003-3405-1247; Jun Yan 0000-0003-3640-1714.
She took care not to be noticed as she reached the ship, and directly she got on board she once more changed to her former lovely appearance and told the prince that her luggage was now all on board, and that they need wait for nothing more
Ma YJ
A
Ma YJ
 World Journal of Clinical Cases2022年11期
World Journal of Clinical Cases2022年11期
- World Journal of Clinical Cases的其它文章
- Pleomorphic adenoma of the left lacrimal gland recurred and transformed into myoepithelial carcinoma after multiple operations:A case report
- Thyrotoxicosis after a massive levothyroxine ingestion:A case report
- Contrast-enhanced ultrasound manifestations of synchronous combined hepatocellular-cholangiocarcinoma and hepatocellular carcinoma:A case report
- Papillary thyroid microcarcinoma with contralateral lymphatic skip metastasis and breast cancer:A case report
- Del(5q) and inv(3) in myelodysplastic syndrome:A rare case report
- Ultrasound-guided local ethanol injection for fertility-preserving cervical pregnancy accompanied by fetal heartbeat:Two case reports