Blunt aortic injury–traumatic aortic isthmus pseudoaneurysm with right iliac artery dissection aneurysm: A case report
2022-06-22 08:49:24XiaoXinFangXinHuiWuXiaoFengChen
World Journal of Clinical Cases 2022年15期
INTRODUCTION
Blunt aortic injury occurs in less than 1% of motor vehicle crashes but is responsible for 16% of deaths[1], and up to 80% of patients die before they arrive at the hospital. Of those who survive the initial injury, a majority die without definitive diagnosis[1,2] but are found and reported at autopsy. Approximately 15% of individuals with traumatic aortic rupture survive temporarily, and 90% die within four months[3,4]. A traumatic pseudoaneurysm is formed in survivors[4]. The natural course from aortic rupture to pseudoaneurysm formation with secondary rupture of the aneurysm may be brief or can extend over many years[2]. Clinical presentations of pseudoaneurysms include local mass, severe chest pain, myocardial ischemia, and heart failure secondary to valvular regurgitation or cardiac compression. The diagnosis of pseudoaneurysms with typical clinical manifestations is relatively easy,but nonobvious symptoms of pseudoaneurysms are prone to misdiagnosis or are missed[5]. For patients who survive the initial injury, rapid detection and diagnosis are critical.
At first Rapunzel was terribly frightened31 when a man came in, for she had never seen one before; but the Prince spoke11 to her so kindly,32 and told her at once that his heart had been so touched by her singing, that he felt he should know no peace of mind till he had seen her. Very soon Rapunzel forgot her fear, and when he asked her to marry him33 she consented at once.34 For, she thought, he is young and handsome, and I ll certainly be happier with him than with the old Witch. 35 So she put her hand in his and said:
CASE PRESENTATION
Chief complaints
A 76-year-old man transferred from the local hospital complained of chest pain after trauma for 3 mo that had been aggravated for half a month.
History of present illness
He had a history of a motor vehicle collision 3 mo prior to this admission. Continuous mild chest pain since he had been injured. After positive treatment in our hospital, he was transferred to the local hospital for rehabilitation treatment. Half a month ago, without obvious inducement, his chest pain was transiently aggravated, radiated to the back and was accompanied by chest tightness, which lasted approximately 20 min but resolved on its own. This emergency did not attract the attention of clinicians,and the clinicians did not pursue further diagnostics and treatments. Then, the same symptoms occurred again 5 d before admission. The local hospital performed thoracic aorta computed tomography angiography (CTA) and found that the CTA suggested a pseudoaneurysm in the initial descending segment of the aortic arch. For further treatment, the man was transferred to our hospital.
History of past illness
The patient had been diagnosed with diabetes for 2 years and hyperlipidemia for 10 years before this admission. Three months ago, he underwent partial resection of the small intestine and CT-guided screw fixation of the left sacroiliac joint after the trauma.
Personal and family history
He had a smoking history of 40 years, he smoked approximately 10 cigarettes a day, and he quit smoking more than 10 years prior to admission. He denied a history of alcohol consumption and any relevant family history.
Physical examination
He had a blood pressure of 161/75 mmHg, with a pulse rate of 79 beats
minute (bpm). He had clear lungs and normal heart sounds. Abdominal tenderness and rebound tenderness were not detected. All peripheral pulses were present, and no carotid or subclavian bruit was observed.
Laboratory examinations
The laboratory results showed normal routine laboratory parameters and normal blood biochemistry,and the patient’s troponin T (TnT), troponin I (TnI), myocardial enzymes, thrombin time (TT),prothrombin time (PT), activated partial thromboplastin time (APTT), fibrinogen (FIB), thromboelastogram (TEG), tumor abnormal protein (TAP), C-reactive protein (CRP), and procalcitonin (PCT) were all normal. An ECG suggested sinus bradycardia, and the patient’s heart rate was 57 beats
minute.
Imaging examinations
When thoracic and abdominal aorta CTA were used to evaluate the pseudoaneurysm in the initial descending segment of the aortic arch, a dissecting aneurysm of the right external iliac artery was unexpectedly found.
She grew more and more fond of human beings, and wished more and more to be able to wander about with those whose world seemed to be so much larger than her own
Hornyansky believes that Rumpelstiltskin is a devil character and thus unsympathetic despite the abuse he receives. There are only two beings in the universe who have secret names, unknown to all but the adept: one of them is God, whose holy Name must not be spoken; the other, over whom mortal man may gain power by pronouncing his mysterious proper name, is the devil (Hornyansky 1965, 130).
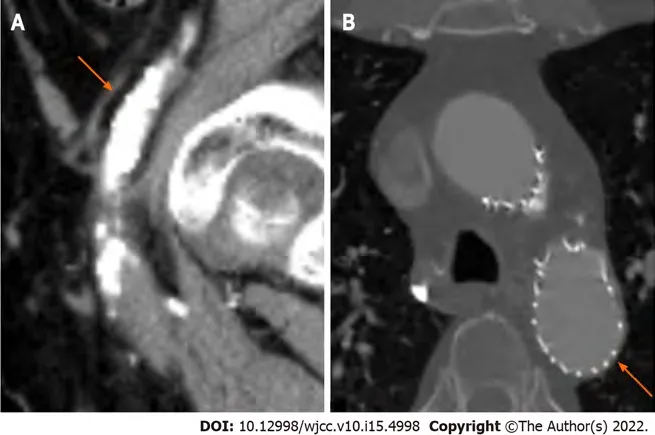
The former thoracic and abdominal aorta CTA images showed sagittal and transverse views of the traumatic aortic isthmus pseudoaneurysm. On the sagittal view (Figure 1A), bulging of the anterior wall of the aortic isthmus was observed. The base was approximately 1.1 cm wide, and the protruding height was approximately 1.5 cm. In the transverse view (Figure 1B), the lumen of the aorta, the crevasse, and the false lumen of this dissection vessel were observed.
His behavior often left us without funds for other more important things. After the dress incident, there was no money for the winter coat I really needed--or the new ice skates I wanted.

The patient we reported here had a deceleration injury from a motor vehicle collision and was admitted to the hospital 3 mo later due to continuous mild but transient aggravation of chest pain. The imaging examinations found pseudoaneurysm of the aortic isthmus, which was logical from the perspective of the course of blunt aortic injury. The patient's first visit to our hospital was 3 mo prior,and the patient complained of pain in multiple parts of his body after his trauma, especially in his abdomen and pelvis. Since his chief complaint was associated with nonthoracic symptoms and since routine screening plain chest radiography in the emergency department showed no obvious aortic injury, pseudoaneurysm or mediastinal abnormality, thoracic aortic CTA was not performed to evaluate whether a potential aortic vascular injury had occurred at that time.

FINAL DIAGNOSIS
The final diagnosis of this case was a traumatic aortic pseudoaneurysm and a traumatic right iliac artery dissection aneurysm.
TREATMENT
Clinical presentations of pseudoaneurysms include the presence of a local mass, severe chest pain,myocardial ischemia, and heart failure secondary to valvular regurgitation or cardiac compression[5].The mortality of aortic pseudoaneurysms is historically more than 95% if the injury is left untreated[13].
OUTCOME AND FOLLOW-UP
The patient’s pseudoaneurysm of the aortic isthmus was a grade 3 injury, and the aneurysm of right iliac artery dissection was a grade 1-2 injury. Endovascular stent graft repair was performed in the operating room. The patient was followed up for 4 years after the operation and eventually recovered well.
DISCUSSION
Blunt aortic injury is a rare but fatal condition associated with motor vehicle collisions, and there are multiple mechanisms involved with blunt aortic injuries. Despite the improved safety measures designed to minimize the occurrence of aortic injuries, the incidence of blunt aortic injury in fatal motor vehicle crashes has not decreased during the past decades[6].
Only 2% to 5% of aortic injuries develop into partial aneurysms or aortic pseudoaneurysms. More than 90% of aortic pseudoaneurysms involve the aortic isthmus[7-9]. Deceleration injury is the most common type of trauma, and the most commonly quoted cause is the differential forces that occur within the chest by deceleration in either the horizontal or vertical plane. The descending aorta remains fixed to the posterior chest wall, while the heart and ascending aorta swing forward and tear at the isthmus[5,10-12].
No obvious contraindications were found in the patient's preoperative auxiliary examination. With the informed consent of his family, endo-vascular stent graft repair was performed in the operating room.Half an hour before the operation, cefuroxime (1.5 g iv drip) was used once to prevent infection. The operation process was smooth. After the operation, a cefuroxime injection (1.5 g iv drip bid) was given for prophylactic anti-infection treatment.
The latter thoracic and abdominal aorta CTA images showed sagittal and coronal views (Figure 2) of the dissecting aneurysm of the right external iliac artery, and a double-lumen structure was observed.
According to Downing’s report[14], after reviewing 54 cases of thoracic aortic injury, all of the patients had other serious injuries-17% were neurological, 60% were abdominal, 35% were pelvic fractures, and 65% consisted of fractures that were elsewhere.
Fang XX and Wu XH collected the patient information; Fang XX drafted the manuscript; Wu XH reviewed the literature; Chen XF contributed to the revision; all authors have read and approved the final manuscript.
But the King s son thought often of the lovely maiden whom he had only seen for a moment, though she seemed to him much more fascinating than any lady of the Court
Our clinicians ignored the possibility of a chest injury due to excessive attention to the other injuries in the patient and because the patient had no signs of aortic injury on plain chest radiography. Even if the patient had persistently mild chest pain, no further imaging examinations, such as CTA or magnetic resonance imaging, had ruled out the possibility of blunt aortic injury. Finally, the intermittent aggravation of chest pain aroused the attention of clinicians, and a traumatic aortic isthmus pseudoaneurysm was found by thoracic CTA imaging. Preoperative thoracic and abdominal aorta CTA was used to evaluate the vascular condition, which accidentally found a right iliac artery dissection aneurysm,which was speculated to be caused by the extrusion effect of the motor vehicle collision. According to the Society for Vascular Surgery clinical practice guidelines for the management of blunt aortic injury proposed in 2009, traumatic aortic injury was classified into four categories based on the severity on CTA imaging. These included grade 1, intimal tear; grade 2, intramural hematoma; grade 3, aortic pseudoaneurysm; and grade 4, free rupture. Currently, surgical repair is recommended for grade 2-4 injuries. Since most grade 1 injuries heal spontaneously, expectant management with serial imaging is advised[15,16].
On the first day after the operation, the patient had a fever, the patient’s highest temperature was 38.1°C, his routine blood examinations were rechecked, his PCT and CRP were high, indicating a reaction after stent implantation, and his antibiotics were not adjusted. He still had a fever on the third day after the operation, and his highest temperature was 38.0 °C. Considering the possibility of infection after stent implantation, piperacillin sodium and tazobactam sodium 4.5 g IVGTT bid were used to strengthen the anti-infective treatment. After that, his fever symptoms were controlled, and the inflammatory indexes gradually decreased to normal. The patient was discharged on the 10
postoperative day and received long-term antiplatelet therapy. After 4 years, the follow-up CTA showed that the covered stent was well formed, and no obvious endo-leak was found (Figure 3).
CONCLUSION
Traumatic aortic injury has an incidence of less than 1% in all trauma patients but occurs in one-third of blunt traumatic fatalities, with the majority of deaths occurring at the scene[14]. Due to the extremely low incidence and high mortality, early diagnosis may be difficult but is very important to reduce mortality and improve the prognosis of patients with trauma. Emergency trauma centers should emphasize the identification with clinical cues, which include gross asymmetry in systolic blood pressure (between the two upper limbs or between the upper and lower limbs), widened pulse pressure(as in our case), and chest wall contusion (as in our case, the initial chest CT revealed a mediastinal hematoma). We need to be vigilant for symptoms persisting or developing, even when the initial screening results are negative. Dynamic thoracic and abdominal aortic CTA review should be performed if necessary.
And the fairies gave him these, and a wallet, and a shield, and belted the sword, which had a diamond blade, round his waist, and the cap they set on his head, and told him that now even they could not see him though they were fairies
Two or three days later the master said to him: The Porcelain Maiden is here: but, though she is as lovely as the dawn, she is so wicked that she scratches everyone that approaches her
FOOTNOTES
In a very real sense, each of us as human beings have been given an invisible5 golden box filled with unconditional6 love and kisses from our children, family, friends and God
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
The authors declare that they have no conflicts of interest.
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Xiao-Xin Fang 0000-0002-1354-9698; Xin-Hui Wu 0000-0001-8027-3882; Xiao-Feng Chen 0000-0002-0457-6854.
Fan JR
A
Fan JR
1 Neschis DG, Scalea TM, Flinn WR, Griffith BP. Blunt aortic injury.
2008; 359: 1708-1716 [PMID:18923173 DOI: 10.1056/NEJMra0706159]
2 Parmley LF, Mattingly TW, Manion WC, Jahnke EJ Jr. Nonpenetrating traumatic injury of the aorta.
1958; 17:1086-1101 [PMID: 13547374 DOI: 10.1161/01.cir.17.6.1086]
3 Nzewi O, Slight RD, Zamvar V. Management of blunt thoracic aortic injury.
2006; 31: 18-27[PMID: 16226902 DOI: 10.1016/j.ejvs.2005.06.031]
4 Beel T, Harwood AL. Traumatic rupture of the thoracic aorta.
1980; 9: 483-486 [PMID: 7425422 DOI:10.1016/s0196-0644(80)80309-x]
5 He S, Chen X, Zhou X, Hu Q, Ananda S, Zhu S. Sudden death due to traumatic ascending aortic pseudoaneurysms ruptured into the esophagus: 2 case reports.
2015; 94: e716 [PMID: 25881850 DOI:10.1097/MD.0000000000000716]
6 Schulman CI, Carvajal D, Lopez PP, Soffer D, Habib F, Augenstein J. Incidence and crash mechanisms of aortic injury during the past decade.
2007; 62: 664-667 [PMID: 17414344 DOI: 10.1097/TA.0b013e318031b58c]
7 Fattori R, Russo V, Lovato L, Di Bartolomeo R. Optimal management of traumatic aortic injury.
2009; 37: 8-14 [PMID: 19008125 DOI: 10.1016/j.ejvs.2008.09.024]
8 Meyer A, Bal A, Kuefner MA, Schmid A, Lang W. Aortic pseudo-aneurysm due to traumatic avulsion of an intercostal artery.
2011; 22: e40-e43 [DOI: 10.1016/j.ejvsextra.2011.06.009]
9 Numata S, Ogino H, Sasaki H, Ando M. Traumatic pseudoaneurysm located at distal descending aorta.
2003; 2: 452-453 [PMID: 17670093 DOI: 10.1016/S1569-9293(03)00110-5]
10 O'Conor CE. Diagnosing traumatic rupture of the thoracic aorta in the emergency department.
2004; 21:414-419 [PMID: 15208221]
11 Mouawad NJ, Paulisin J, Hofmeister S, Thomas MB. Blunt thoracic aortic injury - concepts and management.
2020; 15: 62 [PMID: 32307000 DOI: 10.1186/s13019-020-01101-6]
12 Lundervall J. The Mechanism of traumatic rupture of the aorta.
1964; 62: 34-46 [PMID:14197677 DOI: 10.1111/apm.1964.62.1.34]
13 Elganayni F, Abdulghaffar W, Sale HA, Abou-Issa AH, Abouelcibaa O, Bafaraj M, Bayomi MA. Acute traumatic injuries of thoracic aorta: role of 64-MDCTA in diagnosis and management.
2012; 43: 203-210 [DOI:10.1016/j.ejrnm.2011.12.010]
14 Downing SW, Sperling JS, Mirvis SE, Cardarelli MG, Gilbert TB, Scalea TM, McLaughlin JS. Experience with spiral computed tomography as the sole diagnostic method for traumatic aortic rupture.
2001; 72: 495-501;discussion 501 [PMID: 11515888 DOI: 10.1016/s0003-4975(01)02827-2]
15 Azizzadeh A, Keyhani K, Miller CC 3rd, Coogan SM, Safi HJ, Estrera AL. Blunt traumatic aortic injury: initial experience with endovascular repair.
2009; 49: 1403-1408 [PMID: 19497498 DOI: 10.1016/j.jvs.2009.02.234]
16 Lee WA, Matsumura JS, Mitchell RS, Farber MA, Greenberg RK, Azizzadeh A, Murad MH, Fairman RM. Endovascular repair of traumatic thoracic aortic injury: clinical practice guidelines of the Society for Vascular Surgery.
2011;53: 187-192 [PMID: 20974523 DOI: 10.1016/j.jvs.2010.08.027]
 World Journal of Clinical Cases2022年15期
World Journal of Clinical Cases2022年15期
- World Journal of Clinical Cases的其它文章
- Diet and intestinal bacterial overgrowth: Is there evidence?
- Spontaneous liver rupture following SARS-CoV-2 infection in late pregnancy: A case report
- Metastasis of liver cancer to the thyroid after surgery: A case report
- Solitary primary pulmonary synovial sarcoma: A case report
- Knot impingement after arthroscopic rotator cuff repair mimicking infection: A case report
- Clear aligner treatment for a four-year-old patient with anterior crossbite and facial asymmetry: A case report