Special type of Wernekink syndrome in midbrain infarction: Four case reports
2022-06-22 08:49:18YunZhouYangWenXiaHuHongJiangZhai
World Journal of Clinical Cases 2022年15期
INTRODUCTION
Wernekink commissural syndrome (WCS) is a distinct midbrain syndrome that involves the caudal tegmentum of the midbrain and selectively damages the cerebellar superior crural commissure(Wernekink commissure), resulting in characteristic clinical manifestations. Signs and symptoms associated with WCS include persistent bilateral cerebellar dysfunction, eye movement disorder,internuclear ophthalmoplegia, and, rarely, delayed palatine myoclonus. Due to the small number of cases, there are no data on the epidemiology of the disease and only a few case-reports in the literature describing the features of this syndrome[1,2]. Considering the rarity of the syndrome, we hereby present clinical manifestations and imaging results of 4 patients with WCS. Our report may improve clinicians'understanding of the syndrome and provide reference for clinical diagnosis.
At first, the prayers were mechanical. When I would hear their voices in class, I would pray, Dear God, please bless so-and-so . . . But as I continued, I began to think of the kids more often. I especially thought of the girl who got on my nerves the most. I began to think of her more and more, and in my quiet time at home I would ask God to bless her and the rest of my classmates. As time went on, my classmates became more than just annoying kids to me. There was something growing inside my heart for them, something that wasn t there before. They began to feel like family, and I was learning to love them in a way I never thought possible.
CASE PRESENTATION
Chief complaints
Dizziness for 1 wk.
Sudden dizziness since 4 d.
Sudden ptosis of left eyelid and dizziness since 2 d.
Specific signs and symptoms of WCS in our patients are presented in Table 1.
Repeated chest tightness and shortness of breath since 2 d.
So often he would console2 himself and go sit amongst the unables. Of course the able loomploys thought this just punishment. One of the unables would cuddle near him. Although it could not speak, it would gently touch him now and then. Time went by and Tibley looked forward to being with the unables and his special little friend. Then one day Tibley noticed his little friend was extra quiet and no longer reached to touch him. His little friend was sick. Tibley noticed the little unable s coat had holes in it from long wear and he knew that warmth was the only thing that could bring his little friend back. So Tibley after many years became a true able. He sat down and sewed the most beautiful coat the loomploy world had ever seen. Hurriedly he put it on his little friend but nothing happened. A tear came to his eye and a great ache within him but the little friend did not move.
History of present illness
A 55-year-old male patient was hospitalized in our institute with complaints of sudden ptosis of left eyelid and dizziness since 2 d. On examination, the blood pressure was 140/90 mmHg. Patient was conscious and well-oriented, with normal speech. There was obvious ptosis of left eyelid. Left pupil was dilated with absence of pupillary reflex. There was restriction in the movement of the left globe in superior and downward gaze but not on abduction. Right pupil was normal. Bilateral nasolabial sulcus was symmetrical. The muscle strength and muscle tension of the limbs were normal with normal tendon reflexes. Neck was soft and Kirschner's and Brinell's sign were negative. Respiratory, cardiovascular,and abdominal examinations were normal. There was no edema in both lower limbs. Blood and stool routine test, liver and kidney function, and electrolyte, blood lipid, homocysteine, immune, and coagulation profile were all within normal limits.
WCS was diagnosed based on cranial magnetic resonance imaging (MRI), cervical vascular color Doppler ultrasound, and routine blood and biochemical investigations. Blood homocysteine levels were elevated to 20 mcmol/L, while blood counts, liver and kidney function tests, serum glucose, lipid and electrolyte levels were normal.
A 77-year-old male patient was hospitalized in our institute due to sudden dizziness since 4 d.On admission, patient’s blood pressure was 140/85 mmHg, and the patient was conscious and welloriented. There was drooping of right upper eyelid. On ocular examination, pupils were circular, equal in size, and reactive to light but with limited right eyeball adduction and poor visual acuity in superior gaze. The nasolabial sulci were symmetrical, and there was no deviation of tongue on protrusion. The muscle strength and tension of the limbs were normal with normal tendon reflexes. Neck was soft, and Kirschner's sign and Brinell's sign were negative. Respiratory, cardiovascular, and abdominal examinations were normal. There was no edema in both lower limbs. The National Institutes of Health Stroke Scale was 1 point. Blood investigation revealed increased total cholesterol (5.75 mmol/L), triglycerides(2.17 mmol/L), and blood glucose (6.19 mmol/L); decreased serum alanine; and increased serumhomocysteine (18.95 mcmol/L). The percentage of neutrophils were decreased (48.9%), and monocytes were increased (11.4%).
A 55-year-old male patient reported to our institute with a main complaint of dizziness for 1 wk.On examination, the patient was conscious, was welloriented, and had a blood pressure of 190/110 mmHg. Bilateral pupils were circular, equal in size, and reactive to light. There was restricted adduction of the globe towards the right side. Bilateral nasolabial sulci were similar in depth. There was right side deviation of the tongue, normal muscle strength of both limbs, abnormal left finger nose and left heel knee tibia test, and normal right finger nose and heel knee tibia test. The closed eye sign was positive.The tendon reflex of limbs was decreased or even absent. Acupuncture sensation, tactile sensation, and joint position sensations were normal bilaterally but without pathological reflex and meningeal stimulation sign. Respiratory, cardiovascular, and abdominal examinations were normal.
A 68-year-old female patient was hospitalized in our institute with complaints of repeated chest tightness and shortness of breath for 3 years that had aggravated since 2 d. On admission the patient was afebrile with blood pressure of 136/92 mmHg, conscious, and well-oriented. Bilateral pupils were circular, equal in size, and reactive to light. There was no enlargement of any superficial lymph nodes and thyroid gland. The trachea was centered, and jugular vein was dilated. Respiratory sounds were thick but without any rales. On percussion, cardiac boundary was expanded. Heart rate was 91 beats/min with grade 2/6 systolic murmur heard between the second intercostal space at the right edge of the sternum. Abdominal examination was normal. Bilateral swelling was seen in the lower limbs with prominent varicose veins. Tendon reflexes and muscle strength were normal. Patient was initially treated with antihypertensive, hypoglycemic, cardiotonic, and diuretic drugs to improve myocardial remodeling. However, in 2 d the patient developed dizziness, drowsiness, nausea, vomiting, and unclear speech. Pupils were normal is size but with sluggish light reflex. There was limited adduction of right eye. The patient also showed signs of ataxia. Muscle power of lower limbs was reduced. Right pulmonary arterial pressure sign was positive but with negative meningeal stimulation sign. On blood investigation, liver and kidney function, myocardial enzyme, coagulation function, blood routine, urine routine, and stool examination were normal. Troponin levels and B-type natriuretic peptide levels were increased while serum potassium was reduced.
Imaging examinations
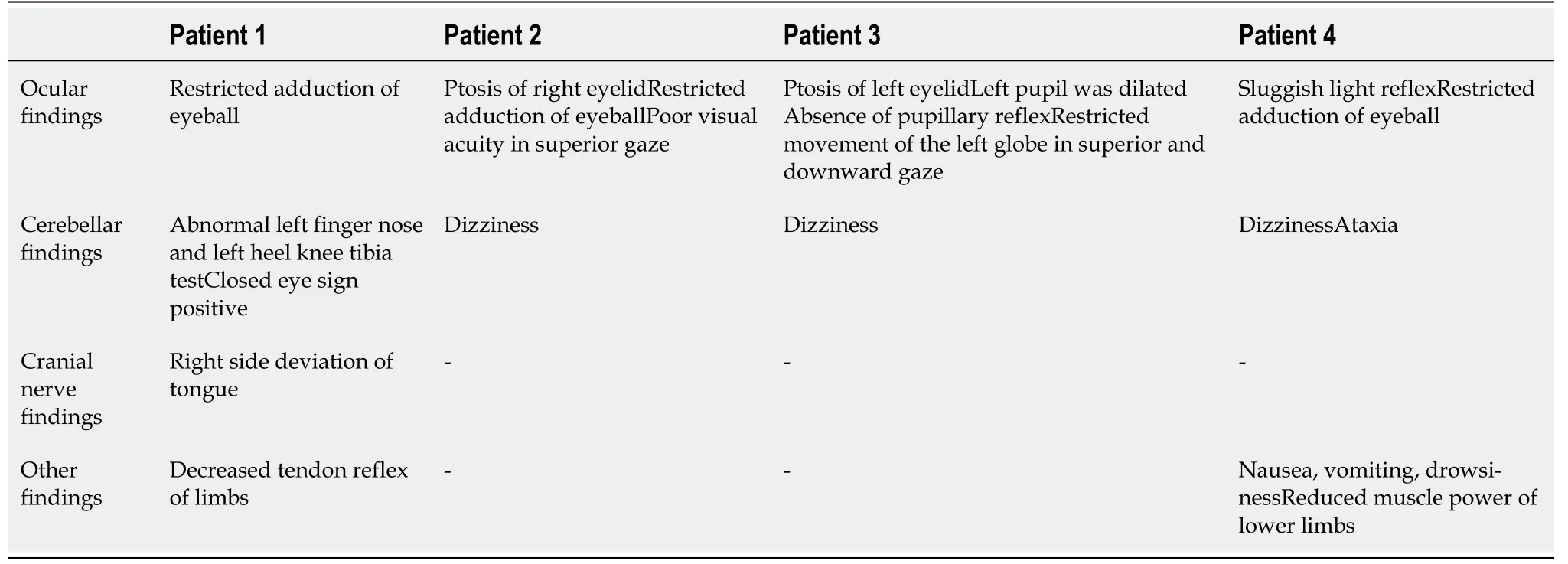
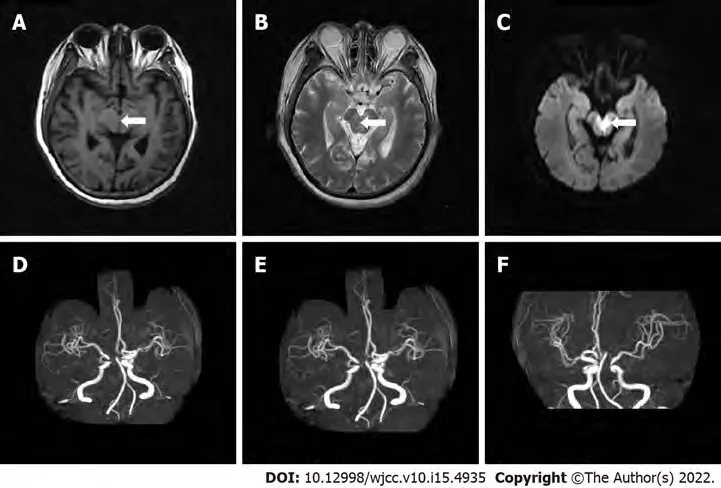
Color Doppler ultrasound of carotid and vertebral arteries showed no obvious abnormalities.Brain MRI demonstrated multiple cerebral infarctions (fresh lesion on the right cerebral foot) and demyelination of cerebral white matter (Figure 1A-C). Electrocardiogram showed T-wave anomaly.Echocardiogram showed thickened left ventricular wall, decreased left ventricular diastolic function,mild mitral regurgitation, and mild tricuspid regurgitation. On computed tomography angiogram(CTA) of head and neck, there was mild atherosclerosis of bilateral carotid arteries and left subclavian artery (Figure 1D-F).
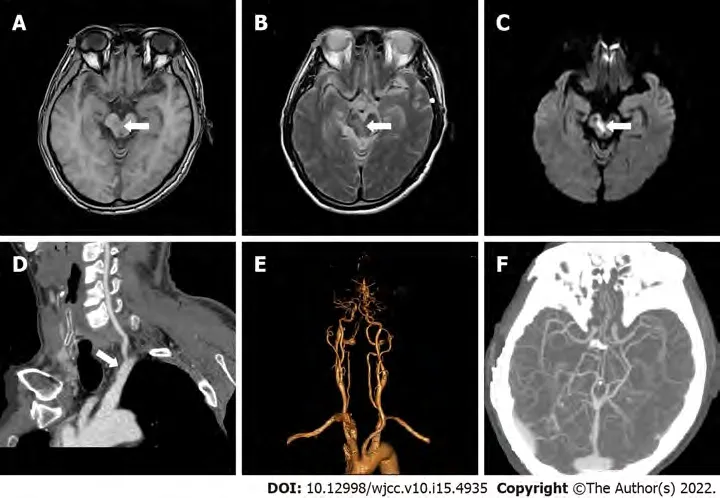
Brain MRI showed multiple cerebral infarctions (fresh lesions in the right cerebral foot),demyelinating changes in white matter, and formation of local softening focus near the left ventricle(Figure 2A-C). Chest X-ray showed that the heart was enlarged. Cerebrovascular CTA revealed a few mixed plaques at the bifurcation of the right common carotid artery (Figure 2D-F).
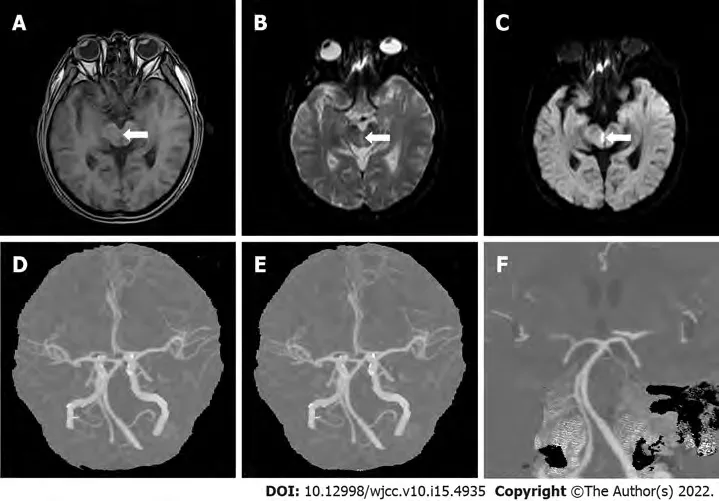
Brain MRI showed multiple cerebral infarction (fresh brainstem lesions), suggesting the recovery of bilateral basal ganglia hemorrhage (Figure 3A-C). Color Doppler echocardiography showed left atrial enlargement, left ventricular hypertrophy, and decreased left ventricular diastolic function.Electrocardiogram, chest X-ray, and color Doppler ultrasound of neck blood vessels were normal. Head and neck CTA revealed multiple moderate stenoses of basilar artery and multiple mild to moderate localized stenoses of bilateral middle cerebral artery (Figure 3D and E).
Chest X-ray showed enlarged heart. Cardiac ultrasound indicated moderate mitral stenosis with mild to moderate mitral regurgitation; mild aortic stenosis with mild aortic regurgitation; pulmonary hypertension with mild tricuspid regurgitation; distended left atrium, and no obvious left atrial mural thrombosis.
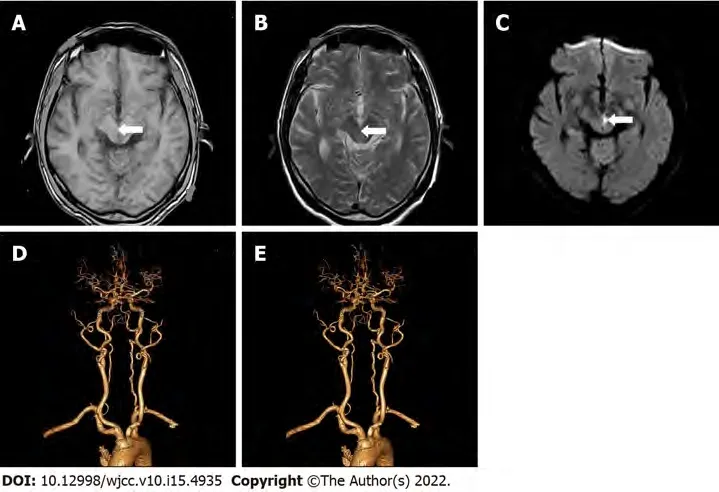
Brain MRI revealed multiple cerebral infarction and thin posterior cerebral arteries bilaterally(Figure 4A-C). CTA suggested right basal ganglia and left occipital lobe infarction (Figure 4D-F).
FINAL DIAGNOSIS
All 4 cases were WCS.
TREATMENT
Patient was started on anti-platelets and anti-plaque agents to protect brain function along with stabilization of blood pressure.
Patient was started on anti-platelets, anti-arteriosclerosis drugs, free radical clearance, and symptomatic treatment.
That was terrible to hear, and he said it in such a tone ofconviction; he described hell to them as a miserable6 hole where allthe refuse of the world gathers. There was no air beside the hotburning sulphur flame, and there was no ground under their feet; they,the wicked ones, sank deeper and deeper, while eternal silencesurrounded them! It was dreadful to hear all that, for the preacherspoke from his heart, and all the people in the church were terrified.Meanwhile, the birds sang merrily outside, and the sun was shiningso beautifully warm, it seemed as though every little flower said: God, Thy kindness towards us all is without limits. Indeed,outside it was not at all like the pastor s sermon.
Patient was started on anti-platelets and anti-arteriosclerosis drugs, with regulation of blood sugar and blood pressure.
Patient was started treatment on anti-platelets, anti-arteriosclerosis drugs, and free radical clearance.
OUTCOME AND FOLLOW-UP
At discharge, the patient had no dizziness with improvement in visual acuity.
Bottigheimer writes that sudden and unanticipated reward after ceaseless labor seems to represent a constant dream at least among Western laborers19, and probably among laboring20 people worldwide, a dream of eternal release from endless grinding toil21 (Tatar, Annotated Grimms, 183)
Considering the anatomic location, any damage to the commissure results in bilateral cerebellar dysfunction along with dysarthric speech, truncal ataxia, and ataxic movements of all four limbs.Ophthalmoplegia of varying degree is also commonly seen with the syndrome and corresponds to the degree of damage[5]. Lesions at the Wernekink commissure seen on an MRI often lead to definitive diagnosis, as seen in our cases. Differential diagnosis for the syndrome can be acute cerebellar encephalitis, which, however, is seen in younger age groups.
At the time of discharge, the patient's dizziness and visual acuity improved slightly; he could eat, but complained of poor sleep at night.
They were immensely surprised at her appearance, but her charming face, and the deplorably ragged17 condition to which the thorns and briers had reduced her once elegant attire18, speedily won their compassion19; they recognised her as a companion in misfortune, and the Queen welcomed her heartily20, and begged her to share their simple repast
A paper outlining the discovery and the properties of this new mineral will be published in the July issue of the journal American Mineralogist, and is available online now
The patient’s condition improved steadily, but he still complained of unclear vision, which was better than initial presentation.
Patient’s condition improved gradually, and she was subsequently discharged.
DISCUSSION
Due to the fact that the midbrain receives overlapping blood supply from the posterior cerebral artery,basilar artery, and superior cerebellar artery, the frequency of midbrain lacunar strokes is not high. The reported rate of midbrain infarction in literature varies from 0.6%-2.3% of all ischemic strokes[1,2].While mesencephalic syndromes like Weber’s syndrome, Claude’s syndrome, and Benedikt’s syndrome are well-known amongst clinicians, WCS is a relatively uncommon mid-brain syndrome that was first described by Lhermitte[3] in 1958. It derives its name from the Wernekink commissure where it manifests (Supplementary Figure 1).
Initially called “the horseshoe-shaped commissure of Wernekink” based on the name of Friedrich Wernekink (a German anatomist), the commissure is a decussation of the brachium conjunctivum. It consists of the two major white matter tracts, namely the ascending dentato-rubro-thalamic tract and the descending dentato-rubro-olivary tract. The ascending tract joins the dentate nucleus of the cerebellum
the superior cerebellar peduncle to the contralateral red nucleus and thalamus. The descending tracts join the dentate and interposed nuclei of the cerebellum
the superior cerebellar peduncle and the inferior olivary nucleus in the medulla to the opposite red nucleus[4]. The Wernekink commissure is present just anterior to the aqueduct and is located at the paramedian area of upper brainstem. The anatomical areas abutting the commissure include medial longitudinal fascicle, reticular formation, and the trochlea and oculomotor nuclei.
They could all speak quite well when they were in the street, but as soon as they came inside the palace door, and saw the guards in silver, and upstairs the footmen in gold, and the great hall all lighted up, then their wits left them! And when they stood in front of the throne where the princess was sitting, then they could not think of anything to say except to repeat the last word she had spoken, and she did not much care to hear that again
CONCLUSION
To conclude, our case series highlights the signs and symptoms of WCS, which is a rare neurological disorder. Clinicians should include WCS in the differential diagnosis in case of patients presenting with bilateral cerebellar ataxia with or without ophthalmoplegia and palatal tremors. MRI is necessary for confirmatory diagnosis of WCS.
FOOTNOTES
Yang YZ and Hu WX reviewed the literature and contributed to manuscript drafting; Zhai HJ analyzed and interpreted the imaging findings; Yang YZ and Hu WX reviewed the literature and drafted the manuscript; Yang YZ and Zhai HJ were responsible for the revision of the manuscript for important intellectual content; All authors issued final approval for the version to be submitted.
8. Terribly dark, and raining so heavily and blowing so hard: In other words, it was a dark and stormy night, the now cliched setting for a story.Return to place in story.
Informed written consent was obtained from the patient for publication of this report and any accompanying images.
The authors declare that they have no conflict of interest.
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
But the children were awake, and had heard the conversation. When the old people were asleep Hansel got up, and wanted to go out and pick up pebbles again, as he had done the first time; but the woman had barred the door,27 and Hansel couldn t get out. But he consoled his little sister, and said: Don t cry, Gretel, and sleep peacefully, for God is sure to help us.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
China
Yun-Zhou Yang 0000-0002-8604-1748; Wen-Xia Hu 0000-0002-4143-8573; Hong-Jiang Zhai 0000-0003-1273-3255.
Zhang H
Filipodia CL
Prince Vivien attacked it gallantly and a fierce combat ensued, which, however, ended before long in the Prince s dealing91 his adversary92 a terrific blow which felled him to the earth
Zhang H
1 Bogousslavsky J, Maeder P, Regli F, Meuli R. Pure midbrain infarction: clinical syndromes, MRI, and etiologic patterns.
1994; 44: 2032-2040 [PMID: 7969955 DOI: 10.1212/wnl.44.11.2032]
2 Kim JS, Kim J. Pure midbrain infarction: clinical, radiologic, and pathophysiologic findings.
2005; 64: 1227-1232 [PMID: 15824351 DOI: 10.1212/01.WNL.0000156520.46056.6B]
3 Lhermitte F. [The cerebellar syndrome: anatomo-clinical study in the adult].
1958; 98: 435-477 [PMID:13615069]
4 Voogd J, van Baarsen K. The horseshoe-shaped commissure of Wernekinck or the decussation of the brachium conjunctivum methodological changes in the 1840s.
2014; 13: 113-120 [PMID: 24078481 DOI:10.1007/s12311-013-0520-9]
5 Liu H, Qiao L, He Z. Wernekink commissure syndrome: a rare midbrain syndrome.
2012; 33: 1419-1421[PMID: 22307446 DOI: 10.1007/s10072-012-0966-4]
 World Journal of Clinical Cases2022年15期
World Journal of Clinical Cases2022年15期
- World Journal of Clinical Cases的其它文章
- Diet and intestinal bacterial overgrowth: Is there evidence?
- Spontaneous liver rupture following SARS-CoV-2 infection in late pregnancy: A case report
- Metastasis of liver cancer to the thyroid after surgery: A case report
- Solitary primary pulmonary synovial sarcoma: A case report
- Knot impingement after arthroscopic rotator cuff repair mimicking infection: A case report
- Clear aligner treatment for a four-year-old patient with anterior crossbite and facial asymmetry: A case report