Cervical spondylotic myelopathy with syringomyelia presenting as hip Charcot neuroarthropathy: A case report and review of literature
2022-03-07 13:06:46LuXiangJYShiCYLiJBGuHCLiuYeGY
World Journal of Clinical Cases 2022年3期
INTRODUCTION
Charcot neuroarthropathy (CN), or Charcot joint, is a systemic disease characterized by progressive bone loss and destruction of the joints and/or spine usually accompanied by dysfunctions of sensitive and autonomic nerves and is reported to be closely associated with diabetes mellitus, HIV, chronic alcoholism, end-stage renal disease, gigantism, intra-articular steroid injections, peripheral neuropathy,meningomyelocele, multiple sclerosis, myelodysplasia, leprosy, amyloidosis, and congenital pain insensitivity[1-3]. However, CN caused by syringomyelia accounts for approximately 5% of CN cases[4]. A retrospective study showed that syringomyeliaassociated CN most often involves the shoulder (17 of 33, 50.0%) and elbow (17 of 33,50.0%), while the hip joint is rarely involved (1 of 33, 2.94%)[5]. To date, a few cases of CN associated with syringomyelia have been reported, but a case report of CN of the hip caused by syringomyelia secondary to cervical spondylotic myelopathy (CSM) has never been published. Therefore, the purpose of this report is to discuss this rare pathological association and to provide new insights into the surgical treatment of CN.
CASE PRESENTATION
Chief complaints
A 76-year-old male patient presented to the Department of Orthopedics of our hospital complaining of worsening progressive right hip pain, a limp when walking and weakness of the right hip. He was admitted to our hospital.
History of present illness
The patient’s symptoms started four years ago with recurrent swelling of the right hip with mild pain, which had worsened in the last 48 h.
History of past illness
The patient initially presente d with neck pain and weakness in all four limbs 16 years ago and was diagnosed with cervical spondylosis, which was treated conservatively.
Personal and family history
The patient had an unremarkable personal and family history.
Physical examination
The patient reported mild pain with flexion and extension of the cervical spine and activity limitation. Apparent swelling was observed in the left hip, and more than 110 mL of clear yellowish joint fluid was extracted. The active range of motion of the right hip was recorded as follows: flexion 90°, abduction 30°, internal rotation 20°, and external rotation 35°, with pain in all directions. The visual analog score was 6/10 points, and the Harris hip score (HHS) was 56 points. Neurologically, the sensation of pain and temperature in the upper and lower extremities was decreased, and proprioception and position sensation were normal. A pathologic reflex was not elicited. Both upper limbs and the right lower limb exhibited weakness with a muscle strength of 4/5, the muscle strength of the left lower limb was normal at 5/5, the right abductor had a muscle strength score of 5/5, and the modified Japanese Orthopedic Association score for CSM was 9/17 points. The bone mineral density (BMD) of the hip was 0.45 g/cm, and the T score was -2.9. Laboratory results were nonspecific.
產銷差率是指銷售水量和供給水量的比值。有研究表明,全球產銷差率平均在27%左右,歐美、日本等發達國家的產銷差率比較低,在10%以下。而非洲、拉丁美洲等發展中國家產銷差率高,達到了40%以上[1]。
Laboratory examinations
Blood biochemistry and urine analyses were normal. Electrocardiogram, chest X-ray and arterial blood gases were also normal. The BMD of the hip was 0.45 g/cm, and the T score was -2.9.
Imaging examinations
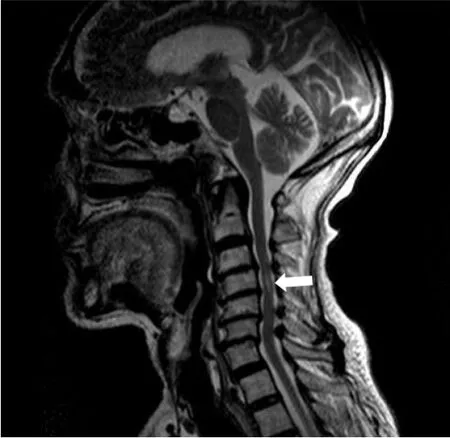
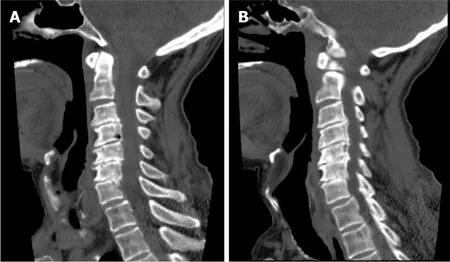
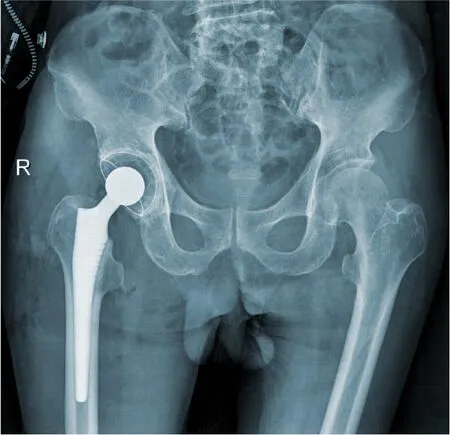
Magnetic resonance imaging (MRI) of the cervical spine showed cervical syringomyelia at C4, cervical disc herniation and spinal canal stenosis from the C3 to the C7 levels (Figure 1). Cervical computed tomography (CT) revealed destruction of the vertebral body at C4 and C5–7 vertebral body assimilation (Figure 2). Threedimensional CT reconstruction, CT scans, and X-rays of the right hip joint showed joint space loss, articular surface collapse, and destructive changes in the acetabulum and femoral head (Figure 3A-C). T2W1 MRI of the right hip showed articular cartilage loss, degeneration of the joint, disordered soft tissue, and apparent joint fluid(Figure 3D).
FINAL DIAGNOSIS
The final diagnosis was CN of the hip associated with syringomyelia and CSM

TREATMENT
● 遙控:自動或手動遠程控制路燈的開/關/調光,可依據路燈的用途、馬路類型分別配置不同的開、關、調光時間。

OUTCOME AND FOLLOW-UP
September 1, 2021
DISCUSSION

CN is considered a multifactorial disease that may lead to progressive bone resorption and destruction of the joints and further develop into joint instability, deformity, and structural collapse with or without pain[6,7]. The possible pathogenesis includes the following: (1) Inflammatory cascading reactions caused by excessive expression of proinflammatory cytokines lead to an increase in osteoclastogenesis; (2) Abnormal neurovascular reflexes at joints promote osteoclast activation, leading to osteopenia;and (3) Painful sensory neuropathy and local temperature increases lead to the accumulation of microtrauma, resulting in joint dislocation and collapse[8,9]. Diabetes is considered the most common cause of CN and usually affects the foot and ankle joints[10]. However, syringomyelia-associated CN accounts for only approximately 5%of CN cases and easily causes upper limb CN[4,11], which most frequently involves the shoulder and elbow joints[3,12]. Only a few studies have reported that CN of the hip and knee joint is a rare complication of lumbar syringomyelia caused by epidural anesthesia[13,14].
Syringomyelia is a chronic progressive condition in which cystic tubular cavitation of the spinal cord is commonly caused by disorders of normal cerebrospinal fluid(CSF) flow dynamics. The possible mechanisms of syringomyelia include: (1) CSF transfer from the fourth ventricle to the central canal[15,16]; and (2) CSF filtration through medullary channels through perivascular and interstitial metastasis[17].While the etiology of syringomyelia is not completely understood, Chiari 1 malformation is generally considered the most significant etiology. Other possible causes include Chiari 2 malformation, myelomeningocele, tethered cord syndrome,hydrocephalus, infection, inflammatory conditions, trauma, extramedullary tumors,arachnoid cysts and spinal canal stenosis[18,19]. As a rare factor, CSM associated with syringomyelia is scarcely reported in the literature[20]. Four potential pathologic mechanisms have been considered for cervical syringomyelia secondary to CSM:Ischemia causing degeneration, microtrauma caused by persistent oppression,hydrodynamic changes in CSF, and the dynamic pincer effect[21]. In addition,enhanced blood flow signals in compressed segments of the cervical spinal cord suggest that dyskinesia of CSF movement may play a role in the process of lesion development[22,23]. The typical clinical manifestation of syringomyelia is weakening or loss of pain and temperature sensation, but proprioception and position sensation are maintained, which is known as "free anesthesia", with muscular atrophy and undernourishment at the level of lesions. With loss of the normal protective reflex,joints may suffer from unrecognized trauma or repeated injury, eventually leading to the occurrence of CN.
In this case, the patient had no significant previous medical history except for CSM diagnosed 16 years prior. According to the MRI results, we found that the patient had CSM and cervical syringomyelia at C4, without other special lesions. Therefore, we suspected that cervical syringomyelia at C4 was associated with long-term CSM,although this is an extremely rare pathological association. Meanwhile, a typical X-ray showed severe hip deterioration, bone loss, and destruction. Interestingly, we carried out systemic physical, laboratory and imaging examinations on the patient, which confirmed that the patient's blood glucose and laboratory results were normal,indicating no other systemic diseases. Therefore, we excluded the differential diagnoses of congenital pain insensitivity, infection and inflammatory joint disease.Finally, after discussion with neurologists and radiologists, the patient was diagnosed with CN of the right hip caused by cervical syringomyelia secondary to CSM.
縣域電力通信網作為最末端的電力通信網,承載電網與用戶的信息交互,是電網業務向服務化轉型的最前沿。而現有的低壓側通信大都采用無線公網技術,尚不能承載如此龐雜的信息量,如何應對用戶側的信息交互是電力通信網研究中的一個難題,還需要考慮此類信息的儲存問題。智能電網發展將為電力通信網帶來新的挑戰,也是電力通信網全面發展的契機。
We suggest a possible etiological association between CSM and syringomyelia, which may reflect a potential pathogenesis of CN. A differential diagnosis should be established for patients with joint swelling, pain and limited mobility, especially patients with chronic shoulder and neck pain. Imaging examinations should be actively performed to rule out the possibility of syringomyelia secondary to CSM.Therefore, the key to successful treatment of patients with CN is comprehensive medical history acquisition, examination and early diagnosis. In addition, arthroplasty may no longer be an absolute contraindication to surgical treatment of CN. Reasonable selection of the surgical strategy can markedly improve the clinical symptoms and quality of life of patients.
Grade C (Good): 0
易開裂區為計算拉應力超過材料抗拉強度的區域,表明易開裂區如圖10所示,內部易開裂區如圖11所示。由于動力條件下廊道應力值較靜力條件下增大在15%以內,而混凝土動強度比靜強度有所提高,所以地震工況下廊道易開裂區沒有顯著增大。在進行廊道材料和結構設計時,只要滿足其靜力工況下的材料強度要求,就能保證滿足設計地震工況下材料強度要求。
綜上所述,UV法結合金屬離子沉淀法操作簡便、準確,精密度、穩定性、重復性好,可用于米索硝唑pH敏感脂質體中主成分的含量測定,其結果與HPLC法含量測定結果一致。
Therefore, adopting reasonable precautions to provide a fixed prosthesis and increase the stability of the hip joint is particularly important to avoid early complications, including: (1) The use of a larger diameter femoral head to reduce the risk of postoperative dislocation; (2) The use of a highly cross-linked polyethylene lining to reduce wear; (3) The use of 3D CT template software to produce femoral stems with appropriate anteversion and femoral offset; (4) The use of a CT navigation system to reproduce the preoperative plan as much as possible; (5) Judicious use of dual mobility constructs; and (6) Revision of the acetabular component and the use of multiple acetabular screws to enhance the firmness of the component[26,29,30]. In addition, we should adhere to conservative treatments during the perioperative period, such as weight-bearing, immobilization, passive stretching, physical therapy and nonsteroidal anti-inflammatory drugs[5].
In our case, the patient refused to undergo cervical decompression surgery. To relieve the pain in the hip joint and restore the motor function of the limbs, we performed right THA. In the preoperative evaluation, the patient suffered from osteoporosis and bone fragmentation and loss around the hip. We suspect that the mass and strength of bone around the hip joint cannot provide sufficient stability at the bone-implant interface if a biotype acetabular cup is adopted. Moreover, the cement-type prosthesis possesses a short curing time, and strong fixation is achieved immediately after curing. Two to three days postoperatively, the patient can begin to bear partial weight with support, which reduces perioperative complications. During the operation, to reduce the risk of dislocation, we used the Hardinge approach to preserve the external rotator muscle group, which can reduce hip joint stability impairment with close suturing of the joint tendon. The cement-type Lubinus antidislocation acetabular cup and a biological fully coated biconical femoral stem were used to improve stability and promote bone ingrowth. After surgery, the patient's symptoms improved, without complications such as recurrent dislocation, loosening of the femoral prosthesis, and fracture around the prosthesis.
CONCLUSION
Early CN is difficult to distinguish from other diseases due to a lack of characteristic clinical manifestations, typical X-ray findings, laboratory tests, and severe underlying neurological disease that can facilitate clinical diagnosis. The management goal for CN patients is early diagnosis and intervention to maintain joint and limb function and active treatment of primary underlying diseases. The surgical strategy for CN of the hip remains controversial.
1.1 儀器 LC-20A HPLC(日本島津公司);AB SCTEX QTRAP 5500 串聯質譜(美國AB公司);T25 D高速勻漿機(德國IKA公司);MS3 D S25渦旋混合儀(德國IKA公司);BSA224S - CW 萬分之一電子天平(德國 Sartorius公司);LDZS - 2 高速離心機(北京京立離心機公司);0.22 μm 有機系微孔濾膜(北京科瑞海科學儀器有限公司)。
We thank the staff at the Department of Radiology and the Department of Pathology in Yunnan Provincial Hospital of Traditional Chinese Medicine.
冰層與閘門牢固結凍后,當氣溫升高時,閘門將受到靜冰壓力影響;當水位升降時,冰層會產生上抬力或下拉力,特別是兩種力同時反復發生時,將導致閘門產生變形,閘墩產生裂縫。每當冬季來臨,我國北方寒冷地區的水庫都存在冰壓力對閘門產生破壞的現象。所以必須采取防冰措施,以盡量避免和減少閘門前的冰壓力,確保閘門安全越冬。
 World Journal of Clinical Cases2022年3期
World Journal of Clinical Cases2022年3期
- World Journal of Clinical Cases的其它文章
- Mycoplasma hominis meningitis after operative neurosurgery: A case report and review of literature
- Recurrence of sigmoid colon cancer–derived anal metastasis: A case report and review of literature
- New method to remove tibial intramedullary nail through original suprapatellar incision: A case report
- Metastasis to the thyroid gland from primary breast cancer presenting as diffuse goiter: A case report and review of literature
- Gastric submucosal lesion caused by an embedded fish bone: A case report
- Epibulbar osseous choristoma: Two case reports