Full recovery from chronic headache and hypopituitarism caused by lymphocytic hypophysitis: A case report
2022-03-07 13:06:38YangMGCaiHQWangSSLiuWangCM
World Journal of Clinical Cases 2022年3期
INTRODUCTION
Histologically, lymphocytic hypophysitis (LYH) is the most common type of primary autoimmune hypophysitis (PAH), accounting for approximately 70% of all causes of PAH, and LYH is characterized by extensive lymphocytic and plasma cell infiltration in the pituitary gland with varying degrees of pituitary dysfunction[1-3]. LYH is a rare disease with an annual incidence of only 1 case per 9 million[1,4]. However, the prevalence of LYH is related to how the diagnosis is made, and the calculation of the incidence of LYH may be inaccurate due to the use of different clinical or pathological diagnostic bases[1,5]. Most LYH patients are young women, and 60% of the cases are diagnosed during pregnancy, especially during the third trimester and early postpartum period[6]. Given its presence as a pituitary adenoma on radiographic images, LYH is misdiagnosed as pituitary adenoma in approximately 40% of patients[7]. This situation represents a common diagnostic dilemma for neurosurgeons with controversial management. Although histopathological examination is the gold standard for the diagnosis of LYH, biopsy and surgery have the potential of adverse events, such as further deterioration of pituitary function[8]. A clinical diagnosis can be made based on a combination of the presenting symptoms, hormonal changes and magnetic resonance imaging (MRI) features[9]. The characteristic manifestations of LYH are often symptoms of sellar mass effects, such as headache, visual field defects,hypopituitarism, diabetes insipidus, and hyperprolactinemia[10]. It has been reported that headaches are often caused by the mass effect of the enlarged pituitary gland and typically resolve permanently after pituitary reduction[11,12]. Here, we report a case of a rare recurrence of headaches following a significant reduction in the pituitary volume with concomitant partial recovery to complete remission of hypopituitarism.
CASE PRESENTATION
Chief complaints
A 56-year-old female patient presented with an intermittent throbbing headache located in the left temporal region. She was admitted to our hospital for neurosurgery.
History of present illness
Two months before hospitalization, the patient did not complain about headache. One month before hospitalization, the headache worsened and became more pronounced at night, and she experienced vision loss with bilateral temporal visual field defects.
由于瀝青混凝土攤鋪施工一旦進行不允許中途中斷,因而需要選用適宜的運輸設備,保障拌和料等能夠及時送至運輸現場,同時最大程度地減少運輸次數與運輸成本,因此需要使用如下公式計算運輸車輛的具體裝卸能力以及運輸次數:
History of past illness
The patient had a history of hypertension for more than 20 years. There was no family history of autoimmune disease.
Personal and family history
科學的課程設置是提高教學質量的前提條件。現有的大學英語課程設置單一,有綜合英語、聽力和口語。綜合英語每周一次,聽力和口語隔周一次,全由一個老師負責。學生的學習受老師影響很大。學生逃課或上課不認真聽講情況時有發生,嚴重影響教學質量。本文以寧波諾丁漢大學英語課程成功的教學案例為例,對建立動態的大學從英語課程設置進行探索。
Physical examination
The patient presented with a height of 160 cm, a weight of 65 kg, a temperature of 36.5°C, and a blood pressure of 140/108 mmHg. The clinical neurological examination showed no abnormalities. Our initial clinical diagnosis was cellar area occupancy.
Laboratory examinations
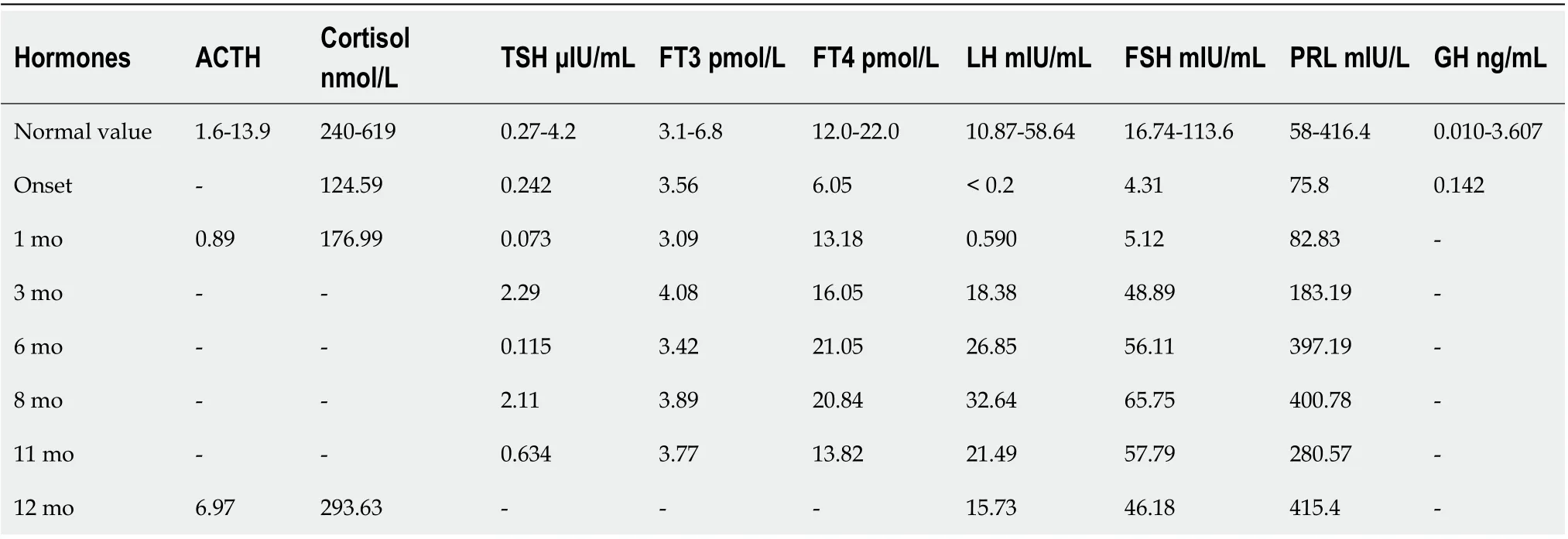
The laboratory data showed a potassium level of 3.2 mmol/L, uroprotein-, and a urinary specific gravity of 1.025. The patient was negative for antinuclear antibodies,immunoglobulin G (IgG), IgM, IgA, and IgG4, which did not support IgG4-related hypophysitis, and no antithyroid antibodies were detected. The remaining biochemical and coagulation test results were unremarkable. The cortisol, adrenocorticotropic hormone (ACTH), follicle-stimulating hormone (FSH), luteinizing hormone (LH),prolactin (PRL), growth hormone (GH), thyroid-stimulating hormone (TSH), free triiodothyronine 3 (FT3), and free triiodothyronine (FT4) levels were measured(Table 1). A water deprivation test was not performed because the patient did not have polyhydramnios or polyuria.
Imaging examinations
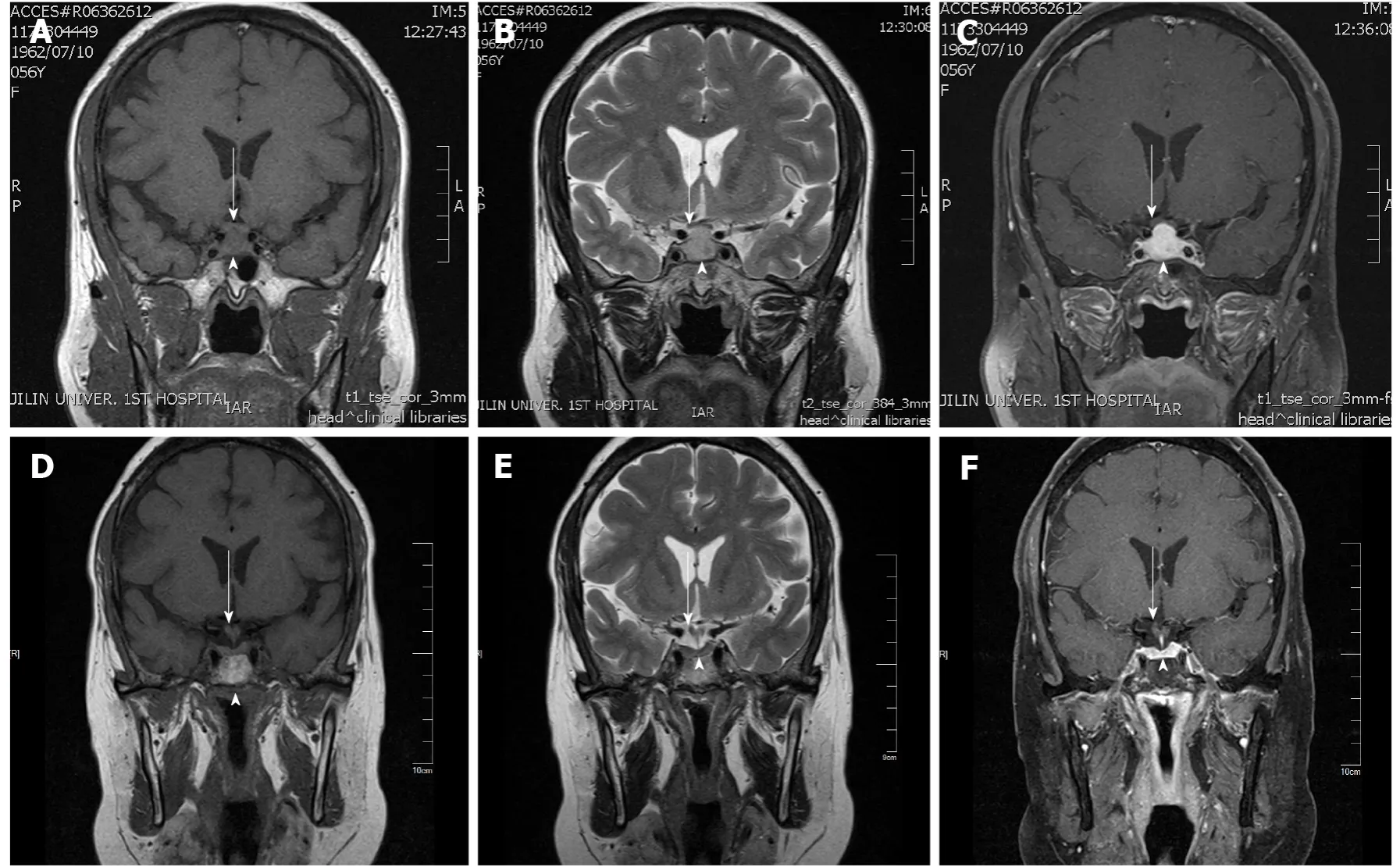
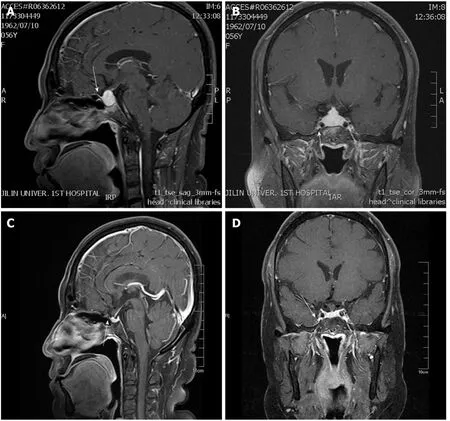
The chest computerized tomography was normal. The electrocardiography was characterized by a flatwave. The MRI of the pituitary gland showed symmetrical enlargement with suprasellar extension in a dumbbell shape with significant homogeneous enhancement after gadolinium enhancement (Figure 1), high signal in the posterior pituitary lobe in the T1 sequence, low signal in the anterior pituitary gland in the T1 sequence and high signal in the T2 sequence. The pituitary stalk was thickened, but not deviated, approximately 3.1 mm at the optic cross and approximately 3.1 mm at the pituitary insertion with an elevation of the optimal crossing(Figure 1). The lesion grew bilaterally toward the cavernous sinuses and encircled the bilateral internal carotid arteries, and the parasternal dural caudal sign was visible(Figure 2), all of which are specific MRI manifestations consistent with LYH.According to the scoring system by Gutenberg[7], our patient was -8, strongly suggesting the diagnosis of LH.
MULTIDISCIPLINARY EXPERT CONSULTATION
Ophthalmologic assistance was requested for the examination, and the assessment suggested temporal visual field defects in both eyes, a corrected visual acuity of 0.5 in the left eye and a visual acuity of 0.8 in the right eye.
FINAL DIAGNOSIS
Considering the rapid progression of hypopituitarism and the combination of the MRI features, laboratory tests, clinical manifestations and epidemiological features, LYH was strongly considered.
TREATMENT
Glucocorticoid therapy was administered in conjunction with an endocrinology consultation, starting with a daily intravenous infusion of 50 mg hydrocortisone. This treatment was changed to 30 mg/d combined with 25 μg/d levothyroxine tablets after 3 d and 20 mg/d after 4 d. The patient's symptoms significantly improved, but the pituitary function did not significantly improve upon reassessment at 1 wk of the steroid treatment. The pituitary-adrenal axis and pituitary-thyroid axis were improved, but the pituitary-gonadal axis did not recover (Table 1). After an evaluation of thepituitary function, the treatment was changed to continuous 120 mg/d- methylprednisolone pulse therapy due to the poor treatment effect and then 80 mg/d after 5 d.Subsequently, pulse therapy was continued for 1 mo and finally discontinued; the headache was significantly relieved, and the visual field returned to normal, suggesting LYH rather than pituitary adenoma.
生:量角器的形狀與角的形狀不一樣,角是尖的,兩條邊是直直的,而量角器有那么多線,沒有“尖”角,一條邊還是曲的,“曲的”怎么能量“直的”呢?
OUTCOME AND FOLLOW-UP
This rare headache regression suggests that patients with chronic headaches should also be alerted to the possibility of LYH.
DISCUSSION
LYH is the most common subtype of PAH and is characterized by diffuse lymphocytic and plasma cell infiltration with fibrosis in the pituitary gland[13], and the pathological process involves inflammatory changes, edema and enlargement of the pituitary gland, followed by destruction of pituitary cells, parenchymal fibrosis and,ultimately, pituitary atrophy with hypopituitarism[5]. However, the natural course of LYH is poorly understood, and the condition may spontaneously resolve or deteriorate rapidly[14]. In addition, the clinical presentation can widely vary de-pending on the course of the disease[5].
民生水利建設加快發展。完成15891座重點小(2)型病險水庫除險加固任務。中小河流治理重點縣綜合整治和河湖水系連通試點建設力度加大。安排解決6343萬農村人口飲水安全問題。50處大型灌區、153處中型灌區和50處大型灌排泵站完成規劃投資任務。啟動第五批400個小型農田水利重點縣建設。區域規模化高效節水灌溉發展勢頭強勁。農村水電增效擴容改造全面實施。山洪災害防治非工程措施項目進展順利。重大水利工程建設加快推進。
However, the most common complaint in 60% of patients with LYH is headache[15], followed by amenorrhea/erectile dysfunction (59%) and diplopia (27%)[9].Headache is also the most common complaint in the first neurosurgical consultation,with an incidence of 89%[15]. LYH has been reported to present as frontal, temporal,or occipital headache[16-18], severe dull or progressive headache[18], or even trigemino-autonomic cephalalgia[17]. Our patient initially presented with intermittent headaches and later with persistent frontal pain that fluctuated in nature that was characterized by a long duration. The diagnosis of chronic postintracranial disorder headache (CPIDH) is reasonable when the etiologic disease is effectively treated or resolves on its own, but the headache does not resolve or significantly improve after 3 mo[19]. Our patient's headache persisted and repeatedly worsened for more than 8 mo and could be considered CPIDH. It has been suggested that headache is associated with cerebrospinal fluid lymphocytosis, but Honegger[20] did not identify a clear correlation between the degree of headache and the cerebrospinal fluid leukocyte count. It has been suggested that pituitary masses causing cavernous sinus involvement and mechanical pulling of the dura are potential pathological mechanisms underlying secondary headaches associated with LYH[11]. Meningeal and dural compression[21] and cavernous sinus involvement that can cause headache[22] are frequently reported. It has also been reported that headache is combined with hyperprolactinemia in 50% of LYH patients[19], but this was not a problem in our case. It has also been reported that the severity of symptoms and the speed of onset of LYH manifestations are typically not related to the degree of pituitary enlargement and compression of peripheral structures but are related to endocrine cell destruction mediated by autoimmune factors[5,22], and the long-term chronic headache manifestations in our patient may be related to this pathological feature.
觀察兩組對象的睡眠時間及生活質量,生活質量評分主要包含總體健康、生理功能、精神健康等8個方面進行評價,記錄兩組睡眠時間。
ACTH deficiency is the most common endocrine disorder in LYH (60%), followed by TSH deficiency, gonadotropin deficiency and hyperprolactinemia[23]; thus, the pattern of ACTH > TSH > LH/FSH > GH axis deficiency and the specific vulnerability of ACTH secretion to LYH have been suggested in several reports[5,24]. Our patient exhibited ACTH, TSH, and LH/FSH deficiency, which is consistent with the above reports. Another feature of LYH is that the degree of hypopituitarism is disproportionate to the size of the mass, which is also supported by findings in some cases[25].One case report describes pituitary inflammation with pituitary enlargement exhibiting hypopituitarism with a long delay in onset[26]. However, this phenomenon was not significantly represented in the present report.
In recent years, the application of MRI in the sellar region has contributed to the feasibility of clinical diagnosis[8] and has become the preferred modality for the study of pituitary lesions. Typical MRI of LYH shows symmetrical enlargement of the pituitary gland with suprasellar extension with marked homogeneous enhancement,thickening of the pituitary stalk without deviation, disappearance of the bright spot of the pituitary gland in the T1 sequence, and the dural tail sign[20,27-30]. A lingual suprasellar and retrosellar extension of the saddle mass in contact with the basal hypothalamus and even infiltration of the basal hypothalamus is a relatively typical finding in granulomatous pituitary inflammation[20], but this feature was not present in our patient. These features have been confirmed in a larger number of cases, rendering the clinical diagnosis of LYH increasingly simple[31]. However, as an increasing number of cases have been reported, pituitary MRI features, including heterogeneity and ring enhancement, which may also be found on pituitary MRI of LYH, are being updated[25]. Relatively low signals on T1-weighted images and relatively high signals on T2-weighted images may also be MRI manifestations of LYH[14]. The MRI findings of different types of PAH are similar, and it is difficult to differentiate it from pituitary adenoma based only on MRI[32]. The scoring system by Gutenberg[7] can distinguish between nonsecretory pituitary tumors and LYH with a sensitivity of 92% and specificity of 99%, which aids in the differential diagnosis of LYH. Our patient's score was -8, favoring a diagnosis of LYH, although granulomatous hypophysitis could also present with similar sellar infiltration; however,granulomatous hypophysitis is very rare and often found by autopsy[33]. The patient did not agree to biopsy of the pituitary gland and pancreas, and case reports of IGg4-related diseases suggest that the pituitary gland is the least involved[34]. Therefore,although it cannot be excluded, it cannot be diagnosed as IGg4-related hypophysitis temporarily according to the corresponding diagnostic criteria[34]. Necrotizing hypophysitis present with a lack of contrast enhancement and sudden-onset hypopituitarism[35], diabetes insipidus and radiologic findings of the ischemic pituitary are three characteristics of necrotizing hypophysitis[35]. Our patient presented with marked homogeneous anterior pituitary enhancement without ischemic manifestations. Xanthomatous hypophysitis commonly exhibits cystic enlargement and peripheral ring enhancement after contrast[36,37] and is rarely known to improve in response to glucocorticoid therapies[38]. This situation is inconsistent with our patient's findings; thus, necrotizing hypophysitis and xanthomatous hypophysitis were not considered.
The objective of LYH treatment is to rectify the hormone deficiency and relieve the symptoms associated with the effects of the mass. Although glucocorticoids are the preferred pharmacological treatment for LYH, surgery may be considered in the presence of severe neurological or ophthalmic manifestations or the absence of a response to pharmacological treatment[39]. In 2015, Khare[24] described 15 patients from western India with pituitary masses that regressed with conservative treatment. Therefore, unless the symptoms are severe or progressively worsen, conservative treatment may be considered[40]. In addition, postoperative hypopituitarism may occur, and deterioration caused by surgery or biopsy may be avoided[9]. Surgical treatment may contribute to the permanent relief of headache, and headache and visual field defects usually improve shortly after surgery[12]. However, considering the risk of hypopituitarism associated with surgery[41], we did not perform surgery but adhered to long-term glucocorticoid treatment and follow-up, and the outcome was good[42]. Although some patients with LYH may show spontaneous recovery, it is also too late to initiate glucocorticoid therapy 3 mo after symptom onset[7,24]. Our time window for initiating glucocorticoid therapy was 2 mo. Thus, the pituitary function completely recovered, and the headaches, despite the longer duration, were eventually relieved. One study indicates that the first pulse of methylprednisolone was the most effective at less than 6 mo of onset[42], and Wang[23] reported a lower relapse rate associated with longer steroid administration because these authors found a significant difference in relapse rates with steroid drug dose administration times of 6 and < 6 mo. Fortunately, in the absence of significant efficacy with short-term hydrocortisone pulse therapy combined with continuous oral hydrocortisone treatment, the endocrinologist administered long-term methylprednisolone pulse therapy shortly after the onset of the disease to the patient in this case study, and the pituitary function significantly improved until it completely recovered. However, the headache recurred before eventually disappearing completely due to early detection and timely management, and the patient was satisfied with the outcome[5].
CONCLUSION
Grade C (Good): C, C
There was no personal or family history.
We thank the patient and appreciate the help of all family members who participated in this study.
猜你喜歡
中小學實驗與裝備(2021年4期)2021-09-03 02:27:50
少先隊活動(2021年4期)2021-07-23 01:46:22
甘肅教育(2020年18期)2020-10-28 09:06:20
華人時刊(2019年17期)2020-01-06 12:08:10
時代人物(2019年29期)2019-11-25 01:35:16
攝影之友(影像視覺)(2019年3期)2019-03-30 01:36:50
人間(2015年10期)2016-01-09 13:12:54
人間(2015年10期)2016-01-09 13:12:52
沈陽醫學院學報(2015年1期)2015-12-27 13:44:40
醫學教育管理(2015年3期)2015-12-01 06:43:16
 World Journal of Clinical Cases2022年3期
World Journal of Clinical Cases2022年3期
- World Journal of Clinical Cases的其它文章
- Mycoplasma hominis meningitis after operative neurosurgery: A case report and review of literature
- Recurrence of sigmoid colon cancer–derived anal metastasis: A case report and review of literature
- New method to remove tibial intramedullary nail through original suprapatellar incision: A case report
- Metastasis to the thyroid gland from primary breast cancer presenting as diffuse goiter: A case report and review of literature
- Gastric submucosal lesion caused by an embedded fish bone: A case report
- Epibulbar osseous choristoma: Two case reports