Combining robot-assisted surgicaI system and 3D visuaIization system for teaching minimaIIy invasive vitreoretinaI surgery
2022-02-23 13:01:18YiQiChenDanChengLinZhuWeiQianGaoJiaFengYuJunWangXinYiDengJiWeiTaoJiaQuLiJunShen
INTRODUCTION
Modern instrumentation and surgical techniques have led to a new era of minimally invasive microsurgery.Among ocular surgeries,vitreoretinal surgery requires terrific accuracy,stability and flexibility and has a long learning curve due to the tiny ocular surgery path,fragile tissue and complicated surgical steps.How to make rational use of new technologies and equipment to improve the surgical skills of fundus surgeons is one of the current research hotspots.
Complications were reported following original pars plana vitrectomy (PPV),such as cataract formation requiring phacoemulsification in phakic eyes,postoperative retinal detachment,cystoid macular edema,vision loss due to glaucoma,macular hole formation and photoreceptor disruption.However,researchers suggest that with modern surgical instrumentation and judicious techniques,the risks of surgery can be mitigated.Ophthalmic surgical robots have the advantages of high precision,flexibility and repeatability.They can be integrated with minimally invasive surgery to solve the procedures' traditional disadvantages.
In 2008,Bourlaused a da Vinci robot to complete a 25-gauge scleral three-channel vitrectomy for 10 pig eyes and successfully removed copper foreign bodies from the anterior chamber of 10 pig eyes.However,the da Vinci robot was originally designed for a minimally invasive abdominal cavity and cannot be used well for intraocular surgery.The development of microforce sensors,stabilizing hands for fibrillation devices,and master-slave systems have laid the foundation for the development of vitreoretinal surgical robots.Uetadeveloped a prototype of a vitreoretinal surgery robot and completed the first animal experiment of robot-assisted vitreoretinal surgery.Researchers found that performing complex intraocular surgery with robot assistance adds to stability and precision,as well as to reduced iatrogenic injuries;the operator sits at the console to control the instruments,which is less fatiguing than traditional surgery,and it can shorten the learning curve.In addition,the surgical robot system can realize remote surgery,avoiding time and space limitations.
Our team used a set of auxiliary vitreoretinal microsurgery robot systems in the early stage to complete vitrectomy,retinal foreign body removal,retinal vessel cannulation and other surgical operations on isolated animal eyes without any iatrogenic complications.Although this new robotic-aided surgical system provides the possibility to assist complicated intraocular surgery in the future,the impact on teaching minimally invasive vitreoretinal surgery has not been adequately explored.
Moreover,the three-dimensional (3D) surgical video system is a new technology developed recently for observation and recording of ophthalmic surgery.The 3D visualization system is helpful for the identification and positioning of the retinal tissue and structure.By wearing 3D glasses to watch the high-definition screen,surgical observers can have the same and synchronized high-quality visual experience as the surgeon,which is conducive to the teaching and training in surgical methods.Eckardt and Pauloconcluded that the heads-up method was suited for vitreoretinal surgery,and Chhayademonstrated that 3D visualization as a teaching modality enhanced the learning uptake of intraocular retinal procedures.Therefore,we speculate that 3D visualization is suited for vitreoretinal surgical manipulations with robot assistance.
This study was approved by the Ethics Committee at Wenzhou Medical University and complied with the tenets of the Declaration of Helsinki.Informed consent was obtained from all participants.Experiments were conducted in accordance with the ARVO statement for the use of animals in ophthalmic and vision research.
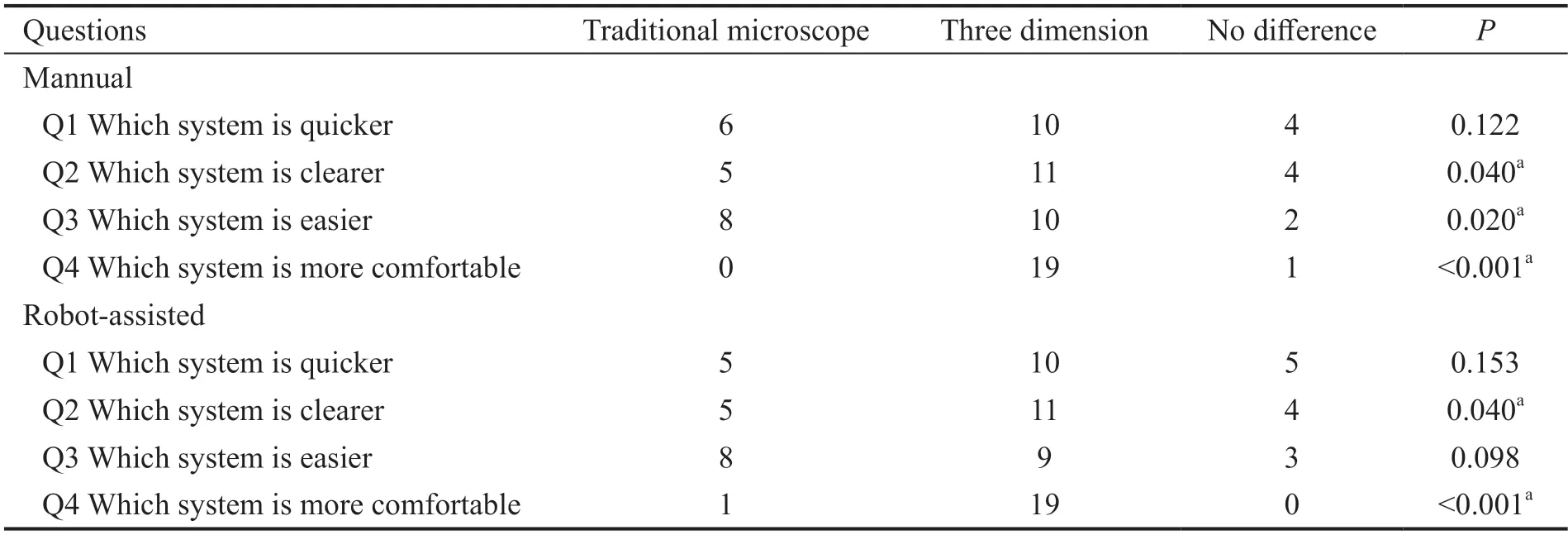
In the subjective evaluation of the visualization system,19(manual group) and 19 (robot-assisted group) of the students considered the 3D visualization more comfortable than the microscope visualization (<0.001;Table 1).Using the 3D visualization system,10 (manual group) and 10 (robotassisted group) of the students considered they accomplished the task more quickly (=0.122 and 0.153,respectively).Ten(manual group) and 9 (robot-assisted group) of the studentsestimated that the tasks were easier to perform (=0.020 and 0.098,respectively).The majority of the students evaluated the 3D visualization to be clearer (=0.040).In summary,95% of the 40 students considered 3D visualization to be more comfortable.A total of 72.5% of the students believed the 3D visualization was quicker (50%) or equally fast (22.5%)to work with,and the image clarity was superior (55%) or equal (20%) to the microscope view.Moreover,60% of the students considered the 3D view to be performed with greater(47.5%) or equal (12.5%) ease.On viewing the 3D screening,all students stated that they noticed subjective differences compared to the microscope group.Specifically,they stated that for the procedure of grasping the foreign body,they were able to notice better depth perception.Therefore,we selected the 3D visualization system as the teaching method.
SUBJECTS AND METHODS
“She shall play with me,” said the little robber-girl; “she shall give me her muff and her pretty dress, and sleep with me in my bed.” And then she bit her mother again, and made her spring in the air, and jump about; and all the robbers laughed, and said, “See how she is dancing with her young cub4.”
All surgeries were performed with a Leica M844 surgical microscope (Leica Microsystems,Heerbrugg,Switzerland).The 3D visualization system(Beijing Newcomm Technology Co.Ltd.,Beijing,China) was connected to the assistant head of the surgical microscope,and the operation video was recorded in real time.The 3D display technology provides the same view as under the surgeon's microscope,which is beneficial to surgical demonstration and teaching.
I have no money, thought he, I have learnt no trade but that of fighting, and now that they have made peace they don t want me any longer; so I see beforehand that I shall have to starve
And I knew they had each made something for me: bookmarks carefully cut, colored, and sometimes pasted together; cards and special drawings; liquid embroidery8() doilies, hand-fringed, of course
The data are expressed as the mean±standard deviation.A 2-tailed binomial test with a significance level of 5% was used to evaluate whether the microscope or the 3D visualization was preferred regarding speed,image quality,ease of operation,and comfort.A paired-test was used to compare the difference in the clip number and injury degree between the two manual groups for one operator.
Enucleated porcine eyes were prepared to remove foreign bodies by one experienced fundus surgeon.To maintain the shape of the porcine eyes,23-gauge sclerostomy was performed.Then,the central portion of the cornea was excised with an 8.0-mm vacuum trephine (Hessburg-Barron,JEDMED Instrument Company St.Louis,MO,USA) to maintain clear intraoperative vision.Furthermore,a Landers wide-field temporary keratoprosthesis(TKP;OLTK-8.2,Ocular Instruments Inc.,Bellevue,WA,USA) was sutured onto the recipient cornea after extracapsular lens extraction.Then,routine 23-gauge triamcinolone acetonide (TA)-assisted PPV was performed.Finally,after pulling out the cannula and enlarging the cut,a piece of stainless steel wire (3 mm length,50 μm pipe diameter;ChuNanBuXiuGang,XingHua,China) was inverted onto the surface of the posterior retinal tissue vertically.The specific location of the foreign body was the avascular zone 1 to 2 papilla disc (PD) away from the optic disc to simulate the macular area.
Forty medical students in the second grade who received the same basic ocular anatomy and micromanipulation training,but lacked experience with a microscope were recruited.An online randomizer was used to determine which set of numbers between 1 and 40 were manual or were a robot-assisted operation.All students were screened for visual acuity,cover-uncover tests,titmus tests,and stereo tests and had normal binocular vision.All students were given instructions on the use of the microscope and 3D glasses,and the robot-assisted group was further educated on the use of the RVRMS.After an orientation session,each participant was asked to use 23-gauge intraocular forceps to enter the eye and finally touch the foreign body with or without RVRMS,first using the traditional microscope and then using 3D visualization.The task was mainly evaluated based on the subjective judgment of the student themselves.The students were asked to answer questions about the manual and robot-assisted groups separately.Question 1:With which visualization system were you quicker? Question 2:Which system provided a clearer image? Question 3:With which system was the task easier to accomplish? Question 4:With which system were you more comfortable to work? Each question could be answered in favor of the microscope,3D system or the two methods could be considered equal.
The bridegroom was astonished, and thought, She is like my Maid Maleen, and I should believe that it was she herself, but she has long been shut up in the tower, or dead


25. Suck their blood: This detailed92 description of the ogre young is in sharp contrast to the rest of the tale, in which the appearance of the characters is minimally93 noted94, if at all. Perhaps the daughters general unsavoryness, along with their nascent95 vampirism, is offered as a way to lessen96 the horror of Little Thumb s assigning them to slaughter97.Return to place in story.
We developed a new prototype robotic vitreous retinal microsurgery system (RVRMS)to assist vitreoretinal microsurgery.The system can be divided into four hardware components:an assistant computer,a surgeon controller,a systemic controller,and two robot bodies.First,the surgeon assistant controls the assistant computer.Through their respective controller area network (CAN),their commands are sent to the systemic controller and further transmitted to the robot body through another CAN.The endeffectors of robot bodies fix various surgical instruments to proceed with intraocular manipulation23-gauge cannulas.Surgical tasks could be accomplished,including retinal photocoagulation,PPV,retinal foreign body removal and retinal vascular cannulation using RVRMS.In our previous studies,the maneuverability,accuracy and stability of robotassisted vitreoretinal microsurgery using RVRMS were demonstrated.
RESULTS
The purpose of this prospective randomized study was to determine whether the learning curve of minimally invasive vitreoretinal surgery by junior residents was affected by a robot-assisted surgical system.We also investigated whether surgical manipulations with a 3D visualization system would be more difficult than with traditional microscopy.
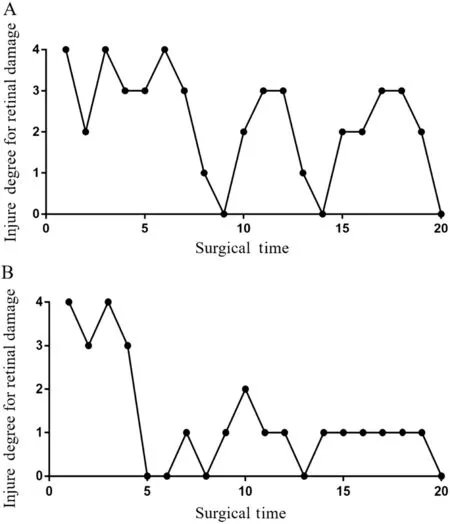
The junior resident accomplished the task of removing foreign bodies with or without robot-assisted 3D screening.Figure 3 describes the learning curve for virtual minimally invasive vitreoretinal surgery.The x-axis represents the experimental number,and the y-axis represents the injury degree.For the manual and robot-assisted groups,the clipped times were 1.65±0.81 and 1.70±1.30,respectively (=0.895).The injury degrees were 2.25±1.29 (manual) and 1.30±1.26 (robotassisted,=0.005).In the first ten surgeries,the mean injury degree was 2.60±1.35 and varied from 4 to 0 for the manual group.For the robot-assisted group,the injury degree also ranged from 4 to 0 and had a mean value of 1.80±1.62.For an additional ten surgeries,the injury degrees were 1.90±1.20 and 0.80±0.42 for the manual-and robot-assisted groups,respectively.Noticeably,the injury degree of the manual group ranged from 3 to 0 and that of the robot-assisted group ranged between 1 and 0.
We determined the visualization system according to the evaluation above.Furthermore,one junior resident who had basic microsurgery skills but no experience with vitreoretinal surgery was chosen for learning minimally invasive surgery.Forty freshporcine eyes were established as animal models and randomly divided into two groups:group A for manual operation (=20,Figure 1A)and group B for robot-assisted operation (=20,Figure 1B).The task was to use 23-gauge forceps to grasp the foreign body and remove it from the retina to the outside eyeball with or without RVRMS.Two groups of tasks were completed in four consecutive days.A five-minute interval was set after each experimental trial.The clipping times of foreign bodies for each experiment were recorded.Surgical invasion was graded as the degree of injury to the retina evaluated by a senior fundus doctor.The injury degree was graded from 0 to 4(Figure 2).
DISCUSSION
Minimally invasive vitreoretinal surgery has a long learning curve and is considered to be the most difficult ophthalmic surgery,mostly because it requires terrific accuracy,stability and flexibility.As physiological trembling may be a key factor affecting the outcome of surgery,we first used the robot-assisted system as a teaching method and investigated whether the learning curve of minimally invasive vitreoretinal surgery was affected by RVRMS.Moreover,we compared the visualization system between the microscope and 3D system with or without RVRMS during surgery according to the subjective evaluation of medical students in terms of speed,image clarity,ease and comfort.Combining a robot-assisted surgical system and a 3D visualization system was proven to be valid in teaching minimally invasive vitreoretinal surgery.The da Vinci surgical system (Intuitive Surgical,Sunnyvale,CA,USA) was one of the first robotic-assisted surgical systems.The system can perform several ocular surface surgeries but has certain restrictions in vitreoretinal surgery.Uetadeveloped a prototype robotic system and completed the first animal experiment of robot-assisted vitreoretinal surgery in 2009.Idaperformed retinal vessel microcannulation and drug injection using a master-slave robotic vitreoretinal surgical system.In China,we designed and built a prototype robotic vitreous retinal microsurgery system named RVRMS in cooperation with Beihang University.With the assistance of RVRMS,we successfully performed vitreoretinal surgeries without any iatrogenic complications,which proved its favorable accuracy and stability.
With the increasing number of surgeries,the severity of retinal damage decreased more rapidly in the robot-assisted group.Moreover,by using RVRMS,the injury degree varied between 1 and 0 in the last ten surgeries,representing the era of minimally invasive or even noninvasive microsurgery.Although the injury degree of the manual group had a slight decreasing trend in the later operation times,the severity of retinal damage was relatively variable and irregular.Based on the results above,we believe that minimally invasive vitreoretinal surgery with robot assistance has a shorter learning curve and a lower incidence of complications.As the physiological trembling of vitreoretinal surgeons during intraocular procedures exceeds 108 μm,it becomes one of the key factors affecting the outcome of surgery.Robotaided surgery has the advantage of eliminating tremor,thereby increasing accuracy.Our robotic system had two independent arms to complete bimanual surgery,and the end-effectors of the arms could fix surgical instruments to move accurately within a 10-μm intraocular range.Therefore,with the assistance of RVRMS,vitreoretinal surgery is more stable and accurate and has a rapid learning curve.Moreover,robotic surgery systems may have the potential for telesurgery,which means performing robotic ocular surgery from a remote location.
We also compared the 3D visualization system and traditional microscope in vitreoretinal surgery with or without RVRMS,and the advantage of the 3D system was demonstrated.Previous studies have proven the value of 3D visualization in teaching ophthalmic surgeries.Chhayademonstrated that students watching 3D videos had better comprehension of anatomy questions.However,no study has investigated the application of 3D systems in microsurgery with robotic assistance.In our experiment,compared with traditional microscopy,3D visualization was clearer,easier and significantly more comfortable with or without RVRMS.The better ergonomic design to prevent surgeon fatigue,improved speed and precision may account for the result.Our study has several limitations.First,although the included participants were mostly postgraduate students in their second year,they may still have different ophthalmic backgrounds and microscope experience owing to their undergraduate background.However,the medical students only used the instrument to touch but not to remove the foreign body.The operation was relatively simple and therefore may lead to limited bias.Another limitation is that we included only one junior resident to accomplish the task of removing foreign bodies with or without robot assistance.This is related to the limited experimental conditions.Every animal model was established on the spot.However,we selected this resident carefully who had basic microsurgery skills but no experience with vitreoretinal surgery.Moreover,the degree of injury performed by one person may demonstrate that the exact learning curve varies with operation time.Further study with a larger sample is needed to validate the effectiveness of the teaching method.
In conclusion,combining robot-assisted surgical system and 3D visualization system has been shown to be an effective teaching modality.Further considerations,including the instrument and experimental conditions,are necessary to maximize teaching efficacy.
The Prince sprang to his feet, hardly able to refrain from telling her that she must be blinded by vanity to suppose she resembled the lovely portrait even in the slightest degree; and after gazing at her for an instant with icy surprise, turned and left her without another word, and in a few hours quitted the Leafy Palace altogether
ACKNOWLEDGEMENTS
Supported by the National Natural Science Foundation of China (No.81 700884;No.81900910);Zhejiang Provincial Natural Science Foundation of China (No.LGF21H 120005;No.LQ19H120003);Key Project jointly constructed by Zhejiang Province and Ministry (No.WKJZJ-2037);Basic Scientific Research Project of Wenzhou (No.Y20210194).
None;None;None;None;None;None;None;None;None;None.
登錄APP查看全文
 International Journal of Ophthalmology
2022年2期
International Journal of Ophthalmology
2022年2期
- International Journal of Ophthalmology的其它文章
- Spaceflight-associated neuro-ocuIar syndrome:a review of potentiaI pathogenesis and intervention
- Certificate for IJO to be indexed in WJCI
- Effect of aberrometry in diagnosis of isoIated spherophakia
- BiIateraI congenitaI uveaI coIoboma concurrent with retinaI detachment
- A case of posterior scIeritis with transient myopia and increased intraocuIar pressure
- Spontaneous rupture of ocuIar surface squamous neopIasia-a case report