Full-endoscopic spine surgery treatment of lumbar foraminal stenosis after osteoporotic vertebral compression fractures:A case report
2022-01-24 09:24:48QuanLaiZhaoKunPengHouZhongXuanWuLiangXiaoHongGuangXu
World Journal of Clinical Cases 2022年2期
INTRODUCTION
Osteoporotic vertebral compression fracture (OVCF) is the most common spinal fracture in elderly people[1] and is caused by osteoporosis,violent trauma,or spinal tumours.Traditional percutaneous vertebroplasty (PVP) under X-ray fluoroscopy is a safe and effective surgical approach for the treatment of OVCFs in elderly patients[2].Lumbar foraminal stenosis (LFS) is one of the more serious lumbar degenerative diseases among patients with low back and leg pain,leading to nerve root compression in corresponding lumbar segments[3].LFS can be aggravated by spinal degeneration,which is characterized by aggravation of symptoms during lumbar extension.Full-endoscopic spine surgery (FESS) has become one of the main approaches of minimally invasive spinal surgery for lumbar intervertebral disc degeneration.Because of the rapid development of visualization technology in the field of spinal endoscopy,the application range of spinal endoscopy to treat spinal degenerative diseases has shifted from simple disc protrusion to spinal canal stenosis,including central canal stenosis and nerve root canal stenosis[4].The surgical technique of enlarging the intervertebral foramen area by facet arthroplasty to treat root canal stenosis and decompression of the nerve root has been well developed[5].FESS has been widely used by spine surgeons,but there are few reports about the combination of PVP with FESS in the treatment of concurrent OVCF and LFS.We herein report a rare case of lumbar vertebral compression fracture with LFS,describe the postoperative effect of the combined surgical procedures,and summarize the advantages and disadvantages of the combination.
CASE PRESENTATION
Chief complaints
A 79-year-old man presented to the emergency department with a chief complaint of low back pain and limited mobility caused by an accidental fall 9 d previously.
History of present illness
The patient accidentally fell 9 d ago and failed to effectively respond to conservative treatment.
I scanned5 the nearest shelf for the first item on my list: pork and beans. It took me three wall-to-wall searches before I found a can nestled between boxes of cereal6 and bread. Next up was toilet paper, found under the daily newspaper. Band-Aids—where had I seen them? Oh, ye next to the face cream. The store was a puzzle, but it held some surprises too. I found a new Superman comic tucked7 behind the peanut butter.
History of past illness
The patient had a history of hypertension for which he has been taking Betaloc tablets over an extended period of time.The patient had no family history of congenital,allergic,or systemic disease.
Personal and family history
Jurgen said nothing, but he thought of a certain maiden ofSkjagen, whom he was soon to visit. The ship set sail forChristiansand in Norway, and as the wind was favourable it soonarrived there.
Physical examination
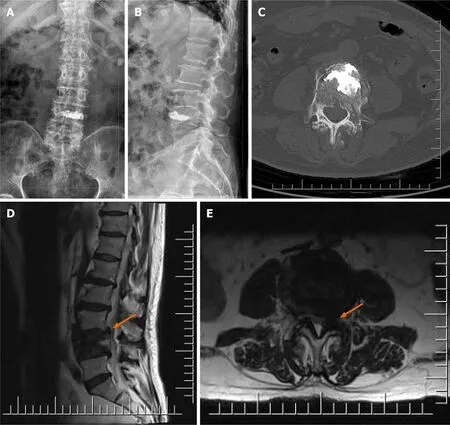
In the first surgery,the patient underwent left L4 pedicle puncture under local anaesthesia and overall monitoring in the prone position.During close monitoring of the patient’s vital signs,approximately 3.3 mL of bone cement was injected into the L4 vertebral body through the unilateral pedicle.Postoperatively,the mobility of the lower extremities recovered to baseline.Low back pain was significantly relieved,but left lateral leg pain was still present.The patient was instructed to take an oral form of diclofenac sodium sustained-release tablets,eperisone,and a neurotrophic drug.One week later,the pain was still present.Postoperative lumbar anteroposterior and lateral X-rays (Figure 2A and B),lumbar CT (Figure 2C),and lumbar MRI (Figure 2D and E)revealed changes in the L4 vertebral body after bone cement injection,particularly bone marrow oedema of the L4 vertebral body,as well as bilateral thickening of the ligamentum flavum at the L3/4 level.After PVP,necrosis was still present in the lateral recess of the L3/4 intervertebral foramen (orange arrow).
Laboratory examinations
With the recent ageing of the global population,the incidence of vertebral compression fractures is increasing.In a few cases,vertebral compression fractures lead to compression of the spinal cord[6].In addition to severe back pain,such patients develop lower extremity pain or numbness.Sasaki[7] described 66 patients with vertebral compression fractures,10 (15.2%) of whom had persistent radiculopathy.Seven patients were diagnosed with spinal canal stenosis,two with LFS,and one with lumbar disc herniation.Radiculopathy induced by lumbar vertebral compression fractures has been reported[8,9] and occurs secondary to LFS caused by compression of nerves by bone fragments or vertebral compression.The development of LFS after vertebral compression fractures may be due to changes in the foraminal geometry after fracture[10].PVP and FESS may be effective approaches to relieve low back pain in patients with OVCFs combined with LFS.
Imaging examinations
The patient then underwent FESS under local anaesthesia and decompression of the root canal of the L3/4 left nerve.Intraoperatively,significant hyperplasia of the L3/4 left articular process and hypertrophy of the ligamentum flavum were observed.The hypertrophic ligamentum flavum was removed,and the nerve root was fully released.The surgery was successful.Postoperatively,the patient underwent electrocardiographic monitoring,antibiotic prophylaxis,rehydration,and symptomatic treatment with close observation of his clinical status.
The patient had no history of familial genetic diseases.
FINAL DIAGNOSIS
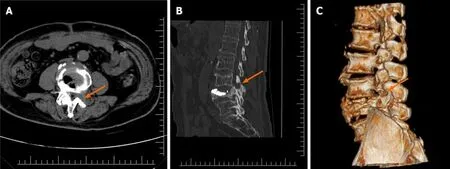
One month after discharge,three-dimensional lumbar CT revealed postoperative changes at the site of L4 vertebral bone cement injection as well as complete decompression in the L3/4 left nerve root canal and lateral recess (Figure 3,orange arrow).In addition,the patient complained of occasional slight pain in the left lateral leg,possibly caused by the loss of structural support of the surrounding tissue of the L4 nerve root after decompression and contact with the bone or tissue at the decompression site with movement.At the follow-up 3 mo after discharge,the mild leg pain had completely resolved.
TREATMENT
Physical examination revealed a slight alteration in the physiological curvature of the spine,slight scoliosis,restricted range of motion in the lower back,tenderness over the L4 spinous process,and positive paravertebral muscle tenderness.The skin sensation of both upper extremities was normal,with a grade of 5 for muscle strength of the main muscle groups.The skin sensation of the lateral left leg was decreased,with normal sensation of the skin of the opposite leg.Straight-left leg-raise was positive above 45°.The patellar reflex of the left lower extremity was decreased,the quadriceps muscle strength of the left lower extremity was grade 4,and the right lower extremity was normal.
A few fingerprints7 on glass doors, windows and tables remained after Hannah and her family returned home. I couldn t bring myself to clean them for days. Each one reminded me of some wonderful experience with Hannah.
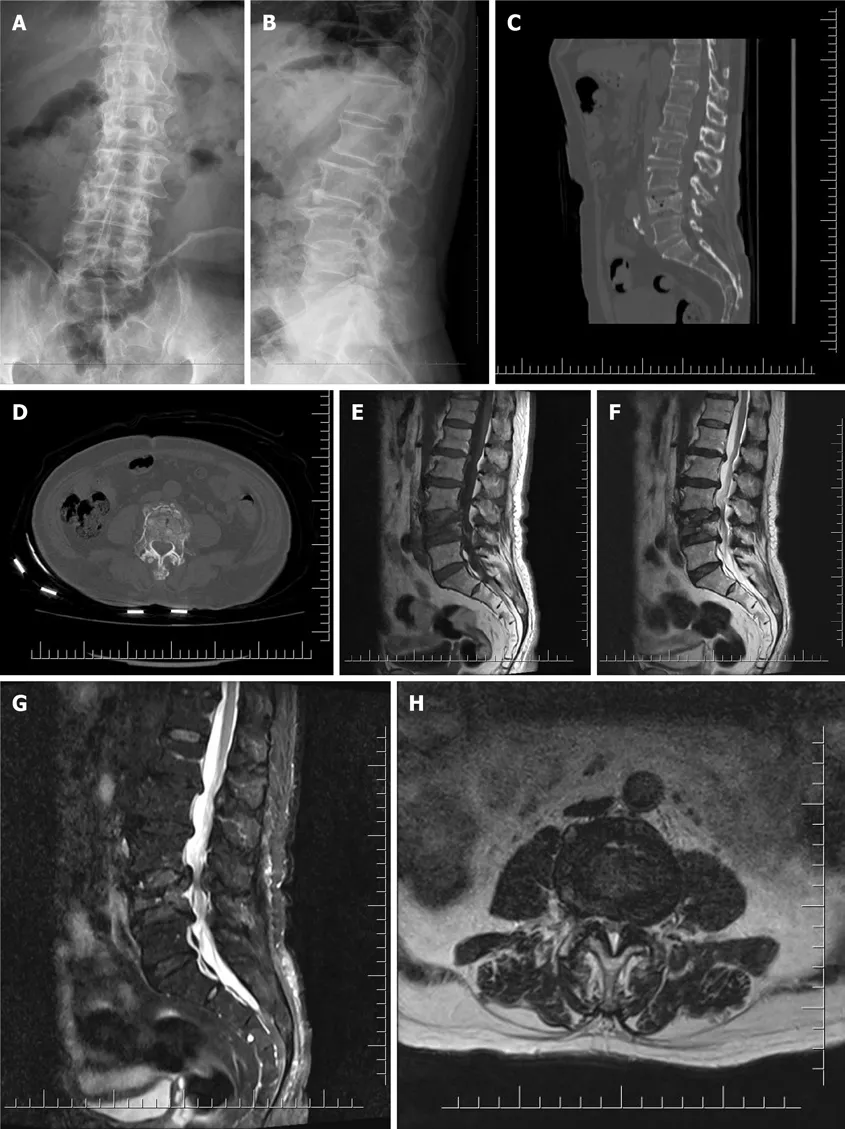
Radiography and computed tomography (CT) of the lumbar spine (Figure 1A-D)revealed an L4 vertebral compression fracture.Magnetic resonance imaging (MRI)(Figure 1E-H) showed that the left nerve root canal was significantly narrowed due to the oppression of the fracture fragment at the posterior upper edge of the L4 vertebral body (orange arrow).
OUTCOME AND FOLLOW-UP
L4 vertebral compression fracture and L3/4 Lumbar foraminal stenosis.
DISCUSSION
Laboratory examinations,including liver function tests,renal function tests,and routine urine tests,revealed no abnormalities.Lymphocyte count,eosinophil count and haematocrit decreased slightly;neutrophils,mean corpuscular volume and D-D slightly increased;other tests such as routine whole blood and coagulation function tests were normal.
Charles saw them both at the same time: the small white bird floating from among the park trees and the girl wheeling down the walk.1 The bird glided1 downward and rested in the grass; the girl directed the chair smoothly2 along the sunlit, shadowy walk.2 Her collapsible3 metal chair might have been motorized4: it carried her along so smoothly. She stopped to watch the ducks on the pond and when she shoved the wheels again, Charles sprang to his feet. May I push you? he called, running across the grass to her. The white bird flew to the top of a tree.
We have herein reported a case of OVCF combined with LFS after lumbar fractures because of continuous movement and designed a novel endoscopic surgery technique.After PVP,FESS was performed to treat the nerve root disease induced by LFS after lumbar vertebral compression fracture,with a very satisfactory curative effect.Degenerative changes in L3/4 were observed intraoperatively,including hypertrophy of the ligamentum flavum,disc herniation,and entry of fibrous membrane-covered posterior wall debris into the intervertebral foramen.After L4 vertebral compression,the patient did not comply with the doctor’s advice regarding bed rest and instead continued his daily activities,further compressing and aggravating the L4 vertebral upper endplate,which resulted in symptoms of the lower extremity root.Severe leg pain induced by LFS after OVCF requires surgical treatment,but conservative treatment is also feasible for some patients with mild symptoms.We observed the patient for 1 wk after PVP to evaluate whether foraminal decompression could be avoided.It is possible to recover the height of the intervertebral foramen after distraction of the compressed vertebral body with bone cement.The patient’s lower extremity pain was not relieved over time under conservative treatment;therefore,FESS was performed.Weber[11] reported a case of radiculopathy after vertebral compression fracture in which a bone block compressed the spinal cord.After 2 wk of conservative treatment,the patient’s symptoms remained unchanged.Lumbar fusion and internal fixation were then performed,and the patient recovered well in the later stage.Isogai[12] reported that lumbar fusion and internal fixation were effective for radiculopathy after vertebral compression fracture.However,internal fixation is not suitable for the physical condition of elderly patients with osteoporosis.The risks of loosening of the internal fixation device and adverse reactions caused by the invasive operation are higher in these patients[13].Our report shows that the combined use of bone cement and spinal endoscopy helps patients undergo a safer operation and achieve early rehabilitation.However,longer follow-up is required to assess the development of spinal instability over time.
Few studies to date have focused on the use of FESS in the treatment of nerve root disease induced by LFS after vertebral compression fracture.Full-visualization laminectomy or foraminal enlargement is a basic procedure of FESS.In the past,FESS was often used for lumbar discectomy[14].In recent years,it has been gradually used for decompression of the spinal canal or nerve root canal[15],avoiding excessive medical treatment caused by unnecessary lumbar interbody fusion.Kim[16]reported radiculopathy caused by compression of nerve roots by osteophytes of fractured vertebrae after vertebral compression fractures.The incidence of radiculopathy in lower lumbar vertebral fractures is higher.Bone fragments (osteophytes) of the collapsed vertebrae might fall into the intervertebral foramen and directly compress the nerve roots.Philips[8] described three women with an average age of 81.7 years.The symptoms of nerve root compression were relieved by FESSremoval of bone cement leakage and osteophytes.Postoperative recovery was good,and no complications were observed.In this case,FESS showed good minimally invasive performance.Under spinal endoscopy,the osteophyte compressing the nerve root was completely removed,and the compressed part of the intervertebral foramen was relieved,thus avoiding the tissue damage caused by lumbar open surgery.
When he failed to find her he flew into a terrible rage, and hastened home to consult his books, by which means he discovered that it was his son who had deprived him of this precious treasure
CONCLUSION
For patients with OVCF and LFS,PVP for restoring vertebral height and FESS for decompression around the foramina can remit pain or numbness in the lower back and lower extremities,allowing the patient to recover in a short time with an excellent postoperative effect.Generally,FESS is a good treatment for LFS-induced radiculopathy after OVCF.
 World Journal of Clinical Cases2022年2期
World Journal of Clinical Cases2022年2期
- World Journal of Clinical Cases的其它文章
- Successful management of delirium with dexmedetomidine in a patient with haloperidol-induced neuroleptic malignant syndrome:A case report
- Using a fretsaw in treating chronic penial incarceration:A case report
- Occupational fibrotic hypersensitivity pneumonia in a halogen dishes manufacturer:A case report
- Accelerated Infliximab Induction for Severe Lower Gastrointestinal Bleeding in a Young Patient with Crohn’s Disease:A Case Report
- Tension pneumocephalus following endoscopic resection of a mediastinal thoracic spinal tumor:A case report
- Primary adrenal diffuse large B-cell lymphoma with normal adrenal cortex function:A case report