Rates of readmission and reoperation after operative management of midshaft clavicle fractures in adolescents
2021-12-28 01:31:50LauraCarrilloHaoHuaWuAmanChopraMattCallahanToshaliKatyalIshaanSwarup
World Journal of Orthopedics
2021年12期
Laura A Carrillo, Hao-Hua Wu, Aman Chopra, Matt Callahan, Toshali Katyal, Ishaan Swarup
Laura A Carrillo, School of Medicine, Medical College of Wisconsin, Milwaukee, WI 53226, United States
Hao-Hua Wu, Matt Callahan, Toshali Katyal, Ishaan Swarup, Department of Orthopaedic Surgery, UCSF, San Francisco, CA 94143, United States
Aman Chopra, School of Medicine, Georgetown University School of Medicine, Washington D.C., WA 20007, United States
Abstract BACKGROUND The national rates of readmission and reoperation after open reduction internal fixation (ORIF) of midshaft clavicle fractures in adolescents is unknown.AIM To determine rates of and risk factors for readmission and reoperation after ORIF of midshaft clavicle fractures in adolescents.METHODS This retrospective study utilized data from the Healthcare Cost and Utilization Project State Inpatient Database for California and Florida and included 11728 patients 10–18 years of age that underwent ORIF of midshaft clavicle fracture between 2005 and 2012. Readmissions within ninety days, reoperations within two years, and differences in patient demographic factors were determined through descriptive, univariate, and multivariate analyses.RESULTS In total, 3.29% (n = 11) of patients were readmitted within 90 d to a hospital at an average of 18.91 ± 18 d after discharge, while 15.87% (n = 53) of patients underwent a reoperation within two years at an average of 209.53 ± 151 d since the index surgery. The most common reason for readmission was a postoperative infection (n < 10). Reasons for reoperation included implant removal (n = 49) at an average time of 202.39 ± 138 d after surgery, and revision ORIF (n < 10) with an average time of 297 ± 289 d after index surgery. The odds of reoperation were higher for females (P < 0.01) and outpatients (P < 0.01), while the odds of reoperation were lower for patients who underwent surgery in California (P = 0.02).CONCLUSION There is a low rate of readmission and a high rate of reoperation after ORIF for midshaft clavicle fractures in adolescents. There are significant differences for reoperation based on patient sex, location, and hospital type.
Key Words: Adolescent; Clavicle fracture; Reoperation; Readmission
INTRODUCTION
In the past decade, there has been a shift in the paradigm for the treatment of clavicle fractures[1]. In both adolescents and adults, the trend has been towards increasing rates of operative management[1-4]. In the pediatric population, demand for return to sport and year-round sporting activity have also made surgical management a more popular treatment option[3]. However, it is unclear if the literature supports the superiority of open reduction internal fixation (ORIF) to nonoperative management in the management of closed midshaft clavicle fractures in adolescents. Recent studies have shown improved outcomes with ORIF in skeletally mature patients[5-7]; however, studies in adolescent patients have shown no difference in functional outcomes[8,9]. Recent literature also suggests surgical complication rates ranging from 21%-86% with close to 50% of patients requiring a second surgery for implant removal[10-12]. To our knowledge, there are no studies that have examined the rates of readmission and reoperation after ORIF of midshaft clavicle fractures in adolescents.
The purpose of this paper is to determine the rates of 90-d readmission and twoyear reoperation after surgical management of midshaft clavicle fractures in adolescents. We hypothesized that the rates of readmission and reoperation would be low after surgical management of clavicle fractures in adolescents.
MATERIALS AND METHODS
The Healthcare Cost and Utilization Project (HCUP) State Inpatient Database (SID) was evaluated for the years 2005-2012. This database, sponsored by the Agency for Healthcare Research and Quality, provides publicly available all-payer statewide data related to inpatient discharge records from community hospitals in participating states[13]. At the time of data collection, 48 States and the District of Columbia provide inpatient data to HCUP[14]. Data for this study were obtained from the Florida (2005-2012) and California (2005-2009) HCUP SID. These states were chosen due to the availability of data over consecutive years, which allowed for a comprehensive review of ninety-day readmissions and two-year reoperations. This study was exempt from Institutional Review Board oversight.
International Classification of Diseases, 9Revision Clinical Modification (ICD-9 CM) diagnosis codes, and the current procedural terminology (CPT) codes were used to identify adolescent patients between the ages of 10 and 18 inclusive, who presented with a midshaft clavicle fracture and underwent an ORIF from January 1, 2005 to December 31, 2012 (ICD-9-CM 79.39, CPT: 23515). Data collection included patient age, sex, race, insurance type, hospital type, and income percentile. We determined the rates of readmission within ninety-days and reoperation within two-years. We compared demographic and socioeconomic factors to determine predictors of readmission and reoperation.
Statistical methods
Descriptive statistics were performed including-test andanalysis to determine statistical significance of adolescent reoperation rates. Multivariate logistic regression was used to compare differences between patients that did or did not require a readmission, and patients that did or did not require a reoperation. Specific predictor variables that were controlled for and analyzed included patient sex, age, race, payer type, hospital type, and state. All statistical analysis was performed using SAS Studio statistical software. Statistical significance was set at< 0.05.
RESULTS
Overall, 11728 adolescent clavicle fractures were analyzed between 2005-2012 in Florida and 2005-2009 in California. Within this cohort, there were 334 clavicle fractures that were managed operatively (2.8%). The surgical cohort consisted of 80.5% (= 265) male and 19.5% (= 64) female patients, and the mean age at time of injury was 16.0 ± 1.7 years (Range: 10-18 years). In total, 3.3% (= 11) of patients were readmitted within 90 d to a hospital at an average of 18.9 ± 18 d after discharge, while 15.9% (= 53) of patients underwent a reoperation within two years at an average of 209.5 ± 151 d since the index surgery.
Of the 334 patients who underwent clavicle ORIF, only 11 patients were readmitted within 90 d after discharge, and the most common reason was a postoperative infection (< 10). Per database reporting restrictions, there is insufficient data for additional analysis.
The most common reason for reoperation was removal of implant (92.5%,= 49) at an average of 202.4 ± 138 d after index surgery. The second most common reason for reoperation was revision ORIF (7.6%,= 4) at an average of 297 ± 289 d after index surgery. There were a greater number of male patients who underwent ORIF (68%32%,= 0.01) compared to females, and there were more reoperations in the state of Florida compared to California (98%2%) (< 0.01) over the study period (Table 1). There were no significant differences in age, race, payer type, median income quartile, and hospital type observed in patients who did or did not have a reoperation within two years (> 0.05). In the multivariate analysis, female patients had greater odds of undergoing reoperation compared to male patients [odds ratio (OR) = 3.49 (1.66-7.33),< 0.01], and patients in California had lower odds of having a reoperation than patients in Florida [OR = 0.08 (0.01-0.66),= 0.02] (Table 2). Additionally, it was demonstrated that patients who had their index surgery at an outpatient center had greater odds of having a reoperation when compared to patients who had their index surgery at a community hospital [OR = 10.76 (2.04-56.83),< 0.01].
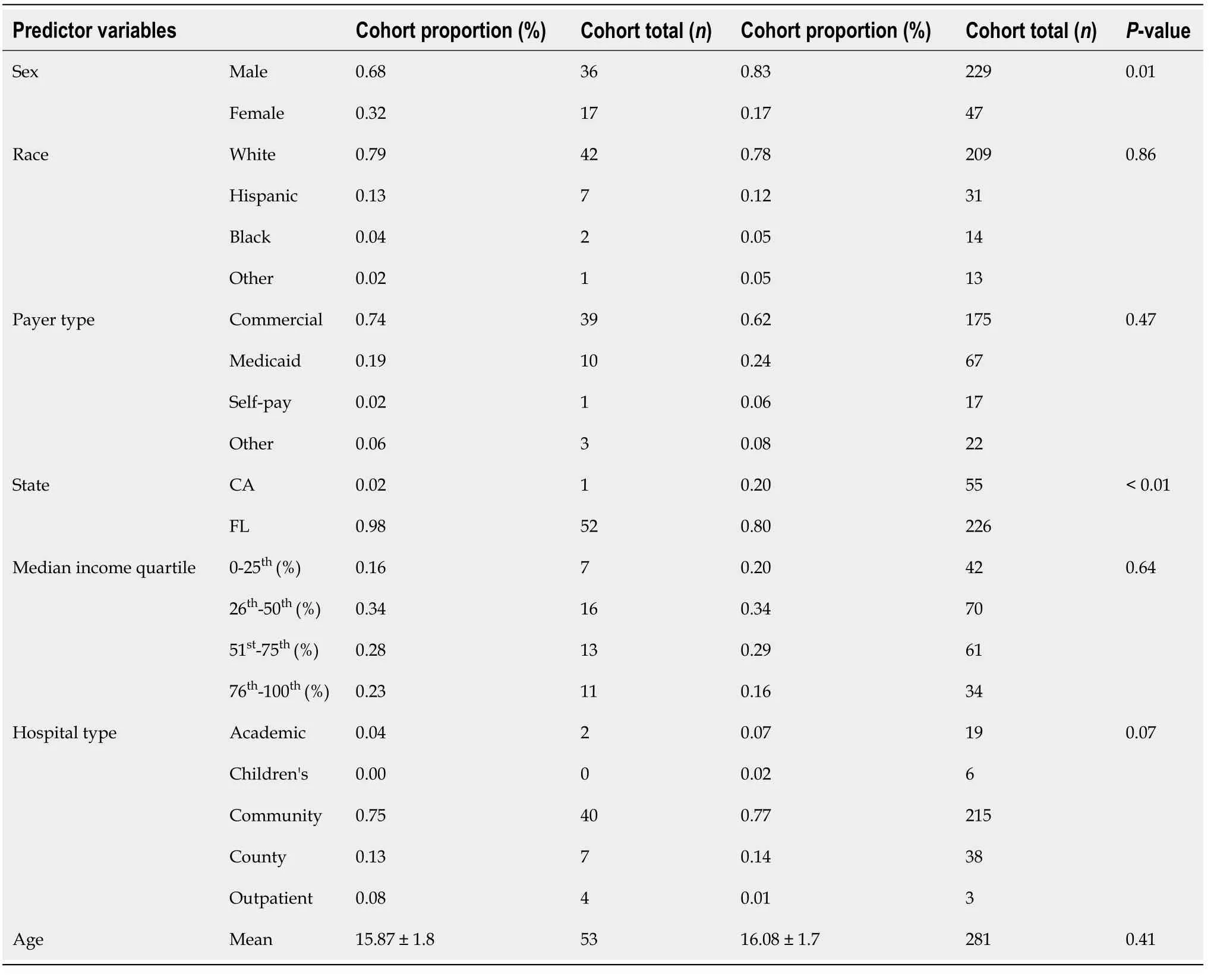
Table 1 Adolescent fracture demographics: Reoperation vs no reoperation
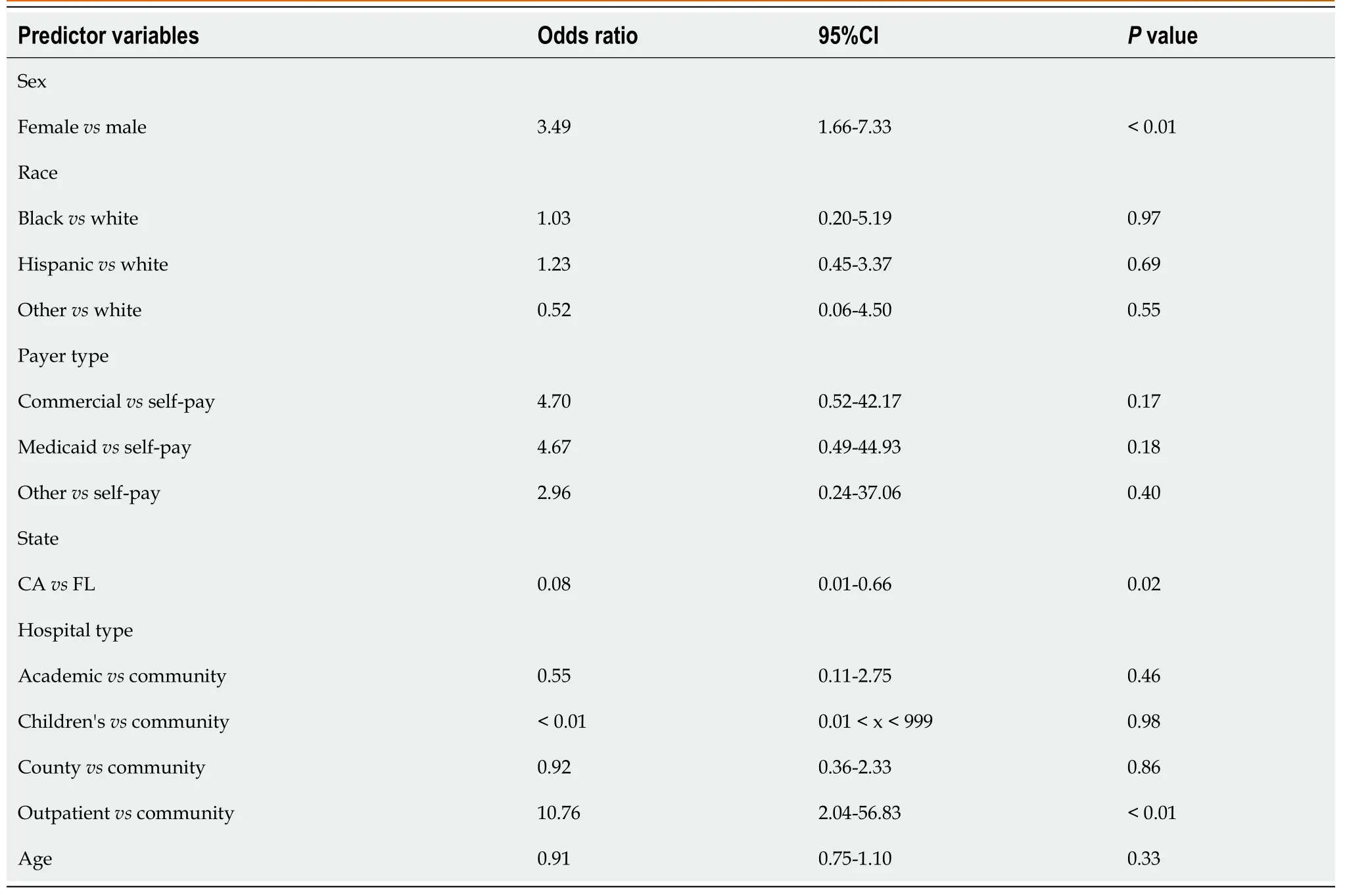
Table 2 Adolescent fracture demographics: Multivariate analysis
DISCUSSION
Recent literature has suggested improved functional outcomes after ORIF for displaced midshaft clavicle fractures in adults[5]. However, these studies have not focused on pediatric or adolescent patients, and the superiority of surgical management in these patients is unclear. There has also been a recent increase in the rates of surgical management of midshaft clavicle fractures in adolescents, and it is important that we understand the rates and reasons for readmission and reoperation after surgery[2,4]. A few studies have described such rates, but these studies have been limited by small samples sizes. To our knowledge, this is the first study to investigate these factors using a large database[12,15-17].
In this study, we found a low rate of readmission but a significantly high rate of reoperation after surgical management of midshaft clavicle fractures in adolescents. Although rates of readmission were low, the most common reason for readmission was postoperative infection. In a previous study by Li[12], 2/85 pediatric patients experienced a wound dehiscence or infection after ORIF. The rate of readmission islikely low after surgical management of midshaft clavicle fractures in adolescents, but additional multicenter studies are needed to validate these results.
Most reoperations were performed due to removal of implant (= 49; 92.45%). This finding is comparable to other reports in the literature. For example, Vander[15] reported 17.6% of adolescent patients underwent implant removal after the operative treatment of a closed midshaft clavicle fracture. This instrumentation removal rate is much lower compared to other studies that have reported rates ranging from 41%-59%[12,15-17]. Reasons for these differences could be related to population differences and differences in regional surgical practice and trends. Overall the high rate of reoperation (15.9%) found among adolescents surgically treated for midshaft clavicle fractures is similar to the reoperation rate reported by Kruppa[18] among children and adolescents surgically treated for femoral shaft fractures (14.3%).
We found significant differences in patients that did or did not undergo a reoperation. We found that female adolescents had a 249% greater odds of undergoing reoperation, which contrasts with findings published by Li[12]. In the adult literature, female sex has been identified as a risk factor for implant removal after ORIF[19,20]. Reasons for this difference have been postulated to relate to a thinner physique and implant irritation with clothing[19-21]. Thus, this may explain why adolescent females were more likely to undergo reoperations in this study. We also found that patients who had their initial surgery performed at an outpatient center had a higher likelihood to undergo reoperation. Additionally, patients in Florida had a higher likelihood to undergo reoperation. Such differences may reflect differences in regional practice and require further investigation.
The results from this study have several implications to clinical practice. First, it provides surgeons with a general idea of the rates of readmission and reoperation after surgical management. Secondly, it allows surgeons to adequately counsel patients regarding risk factors for reoperation. Surgeons may want to consider such characteristics when counseling patients and parents prior to ORIF to ensure no additionalconcerns arise if a reoperation is later needed. For example, it is more likely that female patients will undergo removal of implant after surgical management. Finally, these results provide the framework for additional research to investigate geographic differences and differences in rates based on hospital setting.
Several limitations were present. Given the nature of database studies, we were limited to the data available and did not have access to clinical or radiographic outcomes or patient-reported outcome measures, which may be valuable in future studies. Additionally, we are unable to clearly investigate reasons for readmission and reoperation due to limitations of the database. We were also unable to determine how many patients had implant-related complaintselective implant removal, which may have been recommended by the pediatric surgeon[12]. This study was also limited to two states (California and Florida) due to the lack of data available over consecutive years in the remaining states. Additional studies are needed to understand the applicability of the results nationally and improve the generalizability of these results. As this study is unable to comment on long-term outcomes, future prospective studies are needed to review short, mid, and long-term outcomes, patient reported outcomes, and complications. Despite these limitations, this study is the first to our knowledge to explore readmission and reoperation rates among surgically treated clavicle fractures in adolescents using a large database cohort.
CONCLUSION
In conclusion, the rates of readmission are low after surgical management of midshaft clavicle fractures in adolescents. However, the rates of reoperation are relatively high, and removal of implant remains the primary reason for reoperation. Rates of reoperation significantly differ based on sex and the geographic location of the index surgery. Future multicenter prospective studies are needed to further investigate these findings and ultimately decrease the need for readmission and reoperation after surgical management of midshaft clavicle fractures in adolescents.
ARTICLE HIGHLIGHTS
Research background
In the past decade, there has been a shift in the paradigm for the treatment of clavicle fractures. In both adolescents and adults, the trend has been towards increasing rates of operative management.
Research motivation
It is unclear if the literature supports the superiority of open reduction internal fixation(ORIF) to nonoperative management in the management of closed midshaft clavicle fractures in adolescents.
Research objectives
The primary objective of this paper is to determine the rates of 90-d readmission and two-year reoperation after surgical management of midshaft clavicle fractures in adolescents.
Research methods
This retrospective study utilized data from the Healthcare Cost and Utilization Project State Inpatient Database for California and Florida and included patients 10–18 years of age that underwent ORIF of midshaft clavicle fracture between 2005 and 2012.
Research results
In total, 3.29% (n = 11) of patients were readmitted within 90 days to a hospital at an average of 18.91 ± 18 d after discharge, while 15.87% (n = 53) of patients underwent a reoperation within two years at an average of 209.53 ± 151 d since the index surgery.The most common reason for readmission was a postoperative infection (n < 10).Reasons for reoperation included implant removal (n = 49) at an average time of 202.39± 138 d after surgery, and revision ORIF (n < 10) with an average time of 297 ± 289 days after index surgery. The odds of reoperation were higher for females (P < 0.01)and outpatients (P < 0.01), while the odds of reoperation were lower for patients who underwent surgery in California (P = 0.02).
Research conclusions
There is a low rate of readmission and a high rate of reoperation after ORIF for midshaft clavicle fractures in adolescents. There are significant differences for reoperation based on patient sex, location, and hospital type.
Research perspectives
Future studies are needed to understand the applicability of the results nationally and improve the generalizability of these results. Additional prospective studies are needed to review short, mid, long-term outcomes, patient reported outcomes, and complications for the patient population.
登錄APP查看全文
 World Journal of Orthopedics
2021年12期
World Journal of Orthopedics
2021年12期
- World Journal of Orthopedics的其它文章
- Intraosseous device for arthrodesis in foot and ankle surgery:Review of the literature and biomechanical properties
- Arthroscopic vs open ankle arthrodesis: A prospective case series with seven years follow-up
- Decision aids can decrease decisional conflict in patients with hip or knee osteoarthritis: Randomized controlled trial
- Surgical treatment outcome of painful traumatic neuroma of the infrapatellar branch of the saphenous nerve during total knee arthroplasty
- Role of biomechanical assessment in rotator cuff tear repair:Arthroscopic vs mini-open approach
- Assessing the accuracy of arthroscopic and open measurements of the size of rotator cuff tears: A simulation-based study