Treatment of Helicobacter pylori infection in the presence of penicillin allergy
2021-12-06 08:54:36AmitKumarDuttaPerminderSinghPhull
World Journal of Gastroenterology 2021年44期
Amit Kumar Dutta, Perminder Singh Phull
Abstract Therapy of Helicobacter pylori (H.pylori) requires a combination of antibiotics together with an acid suppressing agent; most treatment regimens include Amoxicillin as one of the antibiotics, which is an important constituent as resistance to it is low. However, allergies to the penicillin group of antibiotics are not uncommon, and treating H.pylori infection in such individuals can be challenging due to the restricted choice of regimens. The aim of this review is to summarise the evidence for therapeutic options in patients with H.pylori infection and penicillin allergy. A literature search was conducted in PubMed for English language publications using the key words ‘Helicobacter’ and ‘treatment’ or‘therapy‘ and ‘penicillin’ or ‘beta-lactam’ and ‘allergy’ or ‘anaphylaxis’. Eighteen studies were identified that specifically evaluated H.pylori treatment success in penicillin allergic patients. The number of subjects in most of them was low and many were retrospective, uncontrolled, single cohort studies. The most effective option for first-line treatment appears to be Bismuth-based quadruple therapy for 10 -14 d. The evidence supports second-line treatment with Levoflaxacin-based triple therapy for 10 d. Patients with persistent H.pylori infection after 2 treatment courses should be considered for testing to confirm penicillin allergy. Further treatment should be guided by the results of H.pylori culture and sensitivity testing.
Key Words: Helicobacter pylori; Infection; Treatment; Penicillin-allergy; Stomach;Duodenum
INTRODUCTION
Infection withHelicobacter pylori(H.pylori) is prevalent worldwide with about half of world’s population estimated to be affected by this gram negative spiral bacterium[1 ].The organism is causally implicated in the pathogenesis of peptic ulcer disease[2 ] and gastric adenocarcinoma[3 ]. Guidelines for the management ofH.pyloriinfection have been published by a number of national societies and organisations[4 -7 ].
Therapy ofH.pylorirequires a combination of antibiotics together with an acid suppressing agent (proton-pump inhibitor, PPI); most treatment regimens include Amoxicillin as one of the antibiotics, which is a particularly important constituent as resistance to it is low[8 ]. However, allergies to the penicillin group of antibiotics are reported in 5 % to 15 % of patients in developed countries[9 ] and, consequently, the treatment options in individuals allergic to penicillin are significantly restricted.
In this review we summarise the available evidence for therapeutic options in patients withH.pyloriinfection and penicillin allergy.
LITERATURE SEARCH
A literature search was conducted in PubMed using the key words ‘Helicobacter’ and‘treatment’ or ‘therapy‘ and ‘penicillin’ or ‘beta-lactam’ and ‘allergy’ or ‘anaphylaxis’for English language publications from database commencement until January 31 ,2021 . Of the 77 publications identified, 18 studies were included in the review (48 were excluded as not relevant, and 11 were review articles)[10 -27 ].
EVIDENCE FOR TREATMENT OF H.PYLORI INFECTION IN THE PRESENCE OF PENICILLIN ALLERGY
Data from studies specifically targeting penicillin allergic patients (Table 1 ).Considering the large volume of publications onH.pyloritherapy, there is relatively little data on treatment of this bacterium in penicillin allergic individuals. A summary of data available from the 18 identified studies is shown in the Table. It should be noted that the number of subjects included in most of them is quite low and many are retrospective, uncontrolled, single cohort studies. All results discussed below are presented on an intention-to-treat basis.
First line therapy
Dual therapy:Prachet al[10 ] reported 100 % treatment success with a 14 d combination of Omeprazole and Clarithromycin; however, this was only in 3 patients.
Triple therapy:The success rate with the 7 d PPI-Clarithromycin-Metronidazole regimen, has been reported as 50 %-83 .3 % in retrospective studies[20 ,21 ] and 54 -58 % in prospective studies[11 ,14 ,18 ]. A longer 14 d regimen also resulted in a low success rate at 63 .6 %[23 ]. The European Registry onH.pylorimanagement (Hp-EuReg) has provided the largest experience of treatment in penicillin allergic patients[25 ].Although drug dose, frequency and duration details were not provided, the PPIClarithromycin-Metronidazole regimen achieved 69 % success rate. Two studies fromJapan, have shown higher success rates (92 .3 %-100 %) for this 7 d triple therapy when combined with Vonoprazan (a potassium-competitive blocker that inhibits gastric H+K+-ATPase) instead of a PPI[20 ,21 ].
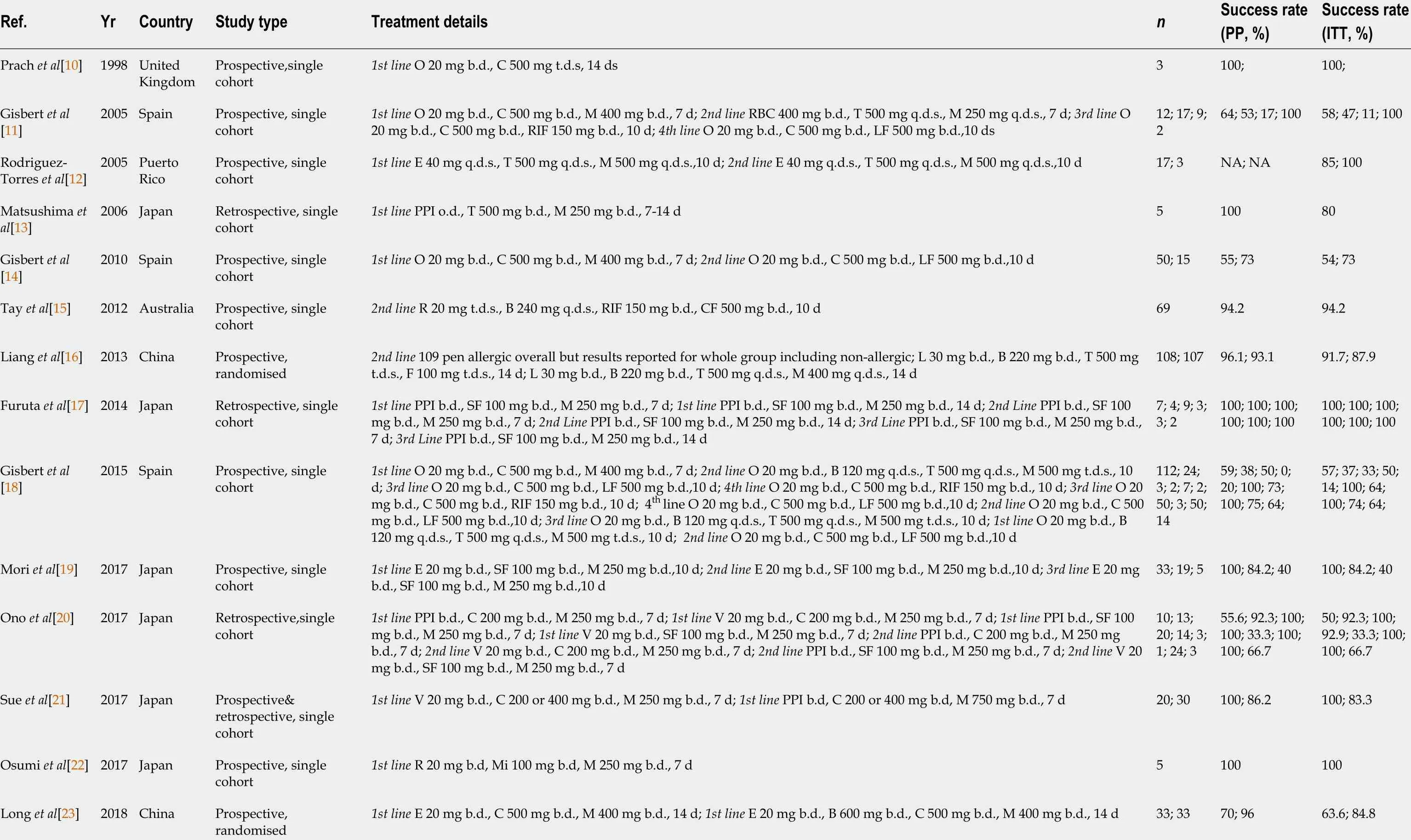
Table 1 Published studies of Helicobacter pylori eradication therapy in patients allergic to penicillin
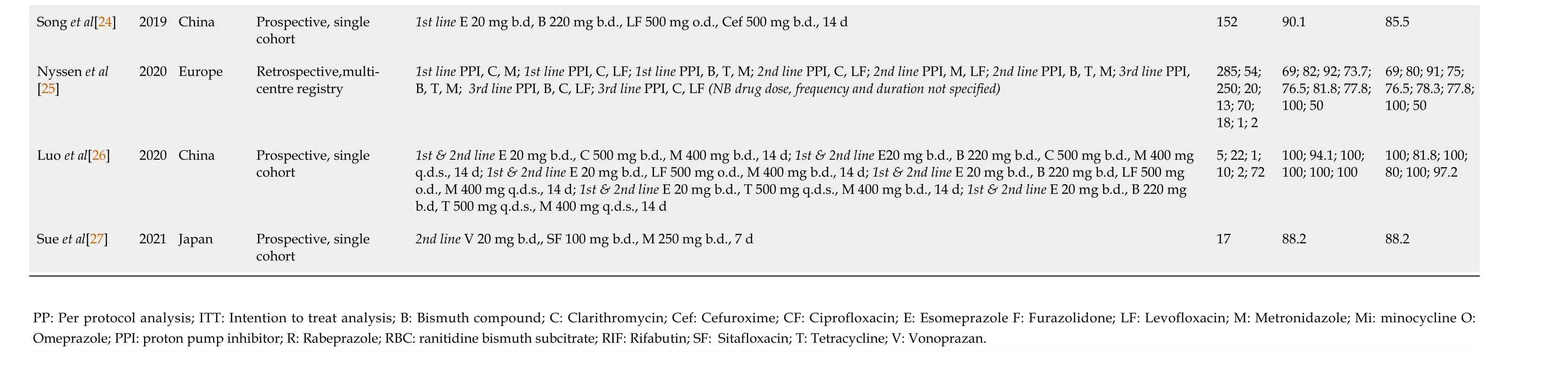
PP: Per protocol analysis; ITT: Intention to treat analysis; B: Bismuth compound; C: Clarithromycin; Cef: Cefuroxime; CF: Ciprofloxacin; E: Esomeprazole F: Furazolidone; LF: Levofloxacin; M: Metronidazole; Mi: minocycline O:Omeprazole; PPI: proton pump inhibitor; R: Rabeprazole; RBC: ranitidine bismuth subcitrate; RIF: Rifabutin; SF: Sitafloxacin; T: Tetracycline; V: Vonoprazan.
In a prospective study, Rodriguez-Torreset alreported a success rate of 85 % with a 10 d triple therapy combining Esomeprazole, Tetracycline and Metronidazole[12 ]. A small retrospective study from Japan also reported a similar success rate of 80 % when this regimen was used for 7 -14 ds[13 ]. Osumi et al achieved a 100 % success rate using a modified 7 d regimen, substituting Minocycline for Tetracycline in a small study of 5 patients[22 ].
Levofloxacin in combination with Clarithromycin and PPI has been reported to achieve an 80 % success rate[25 ]. Recent studies from Japan have evaluated treatment regimens utilising the fluoroquinolone, Sitafloxacin, which has a lower minimum inhibitory concentration forH.pylorithan Levofloxacin and is effective in strains with the gyrA mutation, which denotes resistance to Levofloxacin[19 ]. Remarkably high success rates of 100 % were reported for 7 -14 d treatment regimens combining Sitafloxacin with Metronidazole and PPI, in two retrospective[17 ,20 ] and one prospective study[19 ].
Quadruple therapy: Retrospective data has demonstrated a 91 % success rate for the PPI-Bismuth-Tetracycline-Metronidazole quadruple therapy[25 ]. Three prospective studies have reported success rates of 74 % with a 10 d PPI-Bismuth-Tetracycline-Metronidazole combination[18 ], 84 .8 % with a 14 d PPI-Bismuth-Clarithromycin-Metronidazole regimen[23 ] and 85 .5 % with a 14 d PPI-Bismuth-Levofloxacin-Cefuroxime treatment[24 ].
Second line therapy
In view of the attrition of successfully treated patients with each course of treatment,patient numbers for studies evaluating second line therapies tend to be low, often in single digits[12 ,17 ,20 ].
Triple therapy:Gisbertet al[14 ,18 ] have treated a relatively large number of patients with a 10 d combination of PPI-Clarithromycin-Levofloxacin, demonstrating success rates of 64 %-73 %. Levofloxacin based triple therapy using Clarithromycin or Metronidazole appears to achieve similar success rates, of 75 % and 76 .5 %, respectively[25 ]. Sitafloxacin-based triple therapy has shown success rates of 100 % in 2 small retrospective studies evaluating a 7 d regimen[17 ,20 ], whilst a prospective study investigating a 10 d treatment course reported a lower success rate of 84 .2 %[19 ]. Sueet al[27 ] demonstrated a success rate of 88 .2 % in a prospective study of a 7 d Sitafloxacin regimen using Vonoprazan instead of a PPI.
Quadruple therapy:An early study from Spain reported a low success rate of 47 %using a 7 d regimen of Ranitidine Bismuth citrate-Tetracycline-Metronidazole, which has been considered as quadruple therapy due to an acid-suppressing agent and bismuth being combined into one tablet[11 ]. The same group of investigators also reported a low success rate of 37 % for 10 d PPI-Bismuth-Tetracycline-Metronidazole quadruple therapy[18 ]. However, the European Registry has demonstrated a success rate of 78 .3 % for this regimen[25 ]. In a large prospective study, Liang et al[16 ] included 109 penicillin allergic patients randomised to 2 wk quadruple therapy with either PPIBismuth-Tetracycline-Metronidazole or PPI-Bismuth-Tetracycline-Furazolidine;success rates were 87 .9 % and 91 .7 %, with no difference between penicillin allergic and non-allergic patients[16 ].
A relatively large study from Australia reported on 69 patients with penicillin allergy, who had all failed prior therapy with PPI-Clarithromycin-Metronidazole.Treatment with a 10 d regimen of PPI-Bismuth subcitrate-Rifabutin-Ciprofloxacin achieved a success rate of 94 .2 %[15 ].
Luoet al[26 ] prospectively evaluated an antibiotic susceptibility approach using a variety of 14 d quadruple therapies, and demonstrated high success rates of 80 %-100 %.However, the results were not presented separately for first-line and rescue treatments[26 ].
Salvage (third-line) therapy
The published data for salvage therapy after failure of second-line treatment is very limited with 4 studies reporting on patient numbers in single figures[11 ,17 -19 ]. Details are provided in the Table but it is difficult to draw any meaningful conclusions from the results.
Evidence from non-penicillin combination regimes in unselected groups of patients:
Meta-analyses of trials on the efficacy of non-penicillin regimes in treatingH.pyloriinfection are an alternate source of useful information when making treatment decisions about penicillin allergic individuals. These trials generally included unselected group of individuals without considering penicillin allergy status.
The meta-analysis by Gisbertet al[28 ] demonstrated a success rate of 81 % with 7 d triple therapy regimen of PPI-Clarithromycin -Nitroimidazole, similar to the success rate with the regimen containing amoxicillin instead of nitroimidazole.
Two meta-analyses of randomised controlled trials on first line therapy ofH.pyloriwith quadruple therapy of PPI-Bismuth-Tetracycline-Metronidazole have shown success rates of 77 %[29 ,30 ]. A longer duration (10 -14 d) of quadruple therapy was more effective than the 7 d triple therapy of PPI-Clarithromycin-Amoxicillin[30 ].
SUMMARY AND RECOMMENDATIONS
The triple therapy regimen of PPI-Clarithromycin-Metronidazole is still frequently used as first line therapy for penicillin allergic subjects[25 ]. However, whilst it demonstrates an acceptable success rate of approximately 80 % in unselected patients[28 ], it does not perform well in penicillin allergic patients[11 ,14 ,18 ,20 ,21 ,23 ,25 ]. The reasons for this discrepancy are unclear, but it is possible is that the studies of unselected patients may only have had small numbers of penicillin allergic individuals, or the study design may have excluded individuals with antibiotic allergy. Whilst there is a paucity of recent data for this specific regimen, the efficacy of Clarithromycin-based triple therapy has been shown to be significantly impaired in the presence of Clarithromycin resistance, which is an increasingly encountered issue[29 ]. Whilst increasing the duration of PPI-Amoxicillin-Clarithromycin triple therapy has been shown to improve success rates, this has not been demonstrated convincingly for the PPI-Clarithromycin-Metronidazole regimen[31 ]. If available, Vonoprazan could be considered as a substitute for PPI in clarithromycin-based triple therapy to improve its efficacy[20 ,21 ]. Sitafloxacin-based triple therapy is an alternative option, although this antibiotic is not widely available[17 ,19 ,20 ]. Bismuth-based quadruple therapy,lasting 10 -14 d, is the most attractive option for first-line treatment ofH.pylori, with a high success rate in patients with penicillin allergy[18 ,23 ,24 ,25 ], matching that in unselected patients[29 ,30 ]. In order to optimise the success of first line treatment, a detailed history of prior antibiotic use could aid the choice of regimen prescribed.
In the event of treatment failure, the published evidence suggests that second-line therapy should be instituted with the 10 d PPI-Levofloxacin-Clarithromycin regimen[14 ,18 ]; a Sitafloxacin-based triple therapy is an alternative option[17 ,19 ,20 ,27 ] . If Bismuth-based quadruple therapy has not been used as first-line treatment, then this regime could be considered for subsequent treatment, although there is variable evidence for the efficacy of PPI-Bismuth-Tetracycline-Metronidazole quadruple therapy[16 ,18 ,25 ]. Alternative antibiotic combinations may be more successful such as PPI-Bismuth-Tetracycline-Furazolidine[16 ] or PPI-Bismuth-Rifabutin-Ciprofloxacin[15 ], although there are concerns about the potential for side-effects with rifabutin,especially myelotoxicity[32 ].
It is not possible to provide any evidence-based recommendations for salvage therapy after failure of two treatment courses. It is generally recommended that in this situation, further treatment should be guided by the results ofH.pyloriculture and sensitivity testing[5 ,6 ,26 ]. Another approach is to confirm penicillin allergy at this stage, as many patients with this label turn out not to be truly allergic[5 ,6 ,9 ]. A negative penicillin skin test allows the safe use of amoxicillin-containing salvage regimens, as recommended for non-allergic patients.
CONCLUSION
This review of the evidence for treatingH.pyloriin penicillin-allergic individuals has highlighted the lack of high-quality studies to help guide management strategies.Whilst recommendations have been made based on the limited data, it would be important to monitor the success of treatment regimens and use what can be demonstrated to be effective locally[33 ]. Regional differences in drug availability will influence the choice of regimen, and patterns of antibiotic resistance rates will influence treatment success.
 World Journal of Gastroenterology2021年44期
World Journal of Gastroenterology2021年44期
- World Journal of Gastroenterology的其它文章
- Proton pump inhibitors and colorectal cancer: A systematic review
- Autosomal recessive 333 base pair interleukin 10 receptor alpha subunit deletion in very early-onset inflammatory bowel disease
- Challenges in the diagnosis of intestinal neuronal dysplasia type B: A look beyond the number of ganglion cells
- COVID-19 : Effect on gastroenterology and hepatology service provision and training: Lessons learnt and planning for the future
- Role of early transjugular intrahepatic portosystemic stent-shunt in acute variceal bleeding: An update of the evidence and future directions
- Endoscopic management of difficult common bile duct stones: Where are we now? A comprehensive review