Toric implantable collamer lens for the management of pseudophakic anisometropia and astigmatism
2021-11-30 04:48:04CongYiWangLingWangXiaHuaGangLiYanLiLiAnWu
Cong-Yi Wang, Ling Wang, Xia Hua, Gang Li, Yan Li, Li-An Wu
1Shaanxi Eye Hospital, Xi’an People’s Hospital (Xi’an Fourth Hospital), Affiliated Guangren Hospital, School of Medicine,Xi’an Jiaotong University, Xi’an 710004, Shaanxi Province,China
2Clinical College of Ophthalmology, Tianjin Medical University, Tianjin 300020, China
3Tianjin Aier Eye Hospital, Tianjin 300191, China
Dear Editor,
We present the reported case of toric implantable collamer lens (ICL) implantation for correcting pseudophakic anisometropia after unilateral traumatic cataract surgery 10 years ago. After cataract surgery, the normal pattern of eye development is broken. It is difficult to predict the long-term refractive status after IOL implantation for cataract in children[1]. However, correcting binocular high myopic astigmatism anisometropia in patients with pseudophakic eyes are challenging. Possible strategies to treat high myopic anisometropia include prescribing spectacles and contact lenses, corneal refractive surgeries, and lens-based surgeries,such as refractive lens supplementation and exchange.Patients with myopic anisometropia greater than 3 diopters(D) may be intolerant to aniseikonia and diplopia caused by the full correction of the spectacles. One of the most serious complications associated with improper use of contact lenses is infectious keratitis[2]. Laser refractive surgery may correct residual ametropia in pseudophakic eyes; however, it is only suitable for patients with moderate myopia and limited corneal thickness[3]. The toric visian implantable collamer lens (TICL)may be a suitable surgical option for the correction of high myopic astigmatism with anisometropia in eyes[4]; this method reduces the risk of complications compared with an intraocular lens (IOL) exchange.
The present case described the outcome of toric ICL implantation for pseudophakic anisometropia after unilateral traumatic cataract surgery. We obtained the written informed consent from the patient, and this case study is in accordance with the tenets of the Declaration of Helsinki.
A 23-year-old male was examined with binocular high myopic astigmatism with anisometropia following unilateral phacoemulsification and IOL implantation due to a traumatic cataract in his right eye 10 years ago. The patient underwent blunt contusion of the eyeball by badminton and the cornea was clear. The patient required surgical treatment to rectify refractive error of both eyes. A series of preoperative examination was performed in Xi’an Fourth Hospital. The anterior segment image of the right pseudophakic eye showed that an IOL was in the capsular bag with posterior capsular opacification (Figure 1A). All other examinations of both eyes were normal.
The manifest refraction was -10.00 DS/-2.50 DC×20° in the right eye with corrected distance logarithm of the minimum angle of resolution (logMAR) visual acuity (CDVA) of 0.1 and -6.00 DS/-2.00 DC×160° in the left eye with CDVA of 0.15. Keratorefractive laser surgery was not suitable for the patient because of the relatively thin corneas (482 and 465 μm). ICL power calculations were performed by the manufacturer (STAAR Surgical) by using a modified vertex formula. The size length of the ICL was determined on the basis of the patient’s anterior chamber depth (ACD) measured with scanning-slit topography (Orbscan IIz; Bausch & Lomb,Rochester, New York, USA) and white-to-white (WTW).Preoperative WTW was 11.4 mm in the right eye and 11.4 mm in the left eye, measured under a microscope with calipers.The ACD was 3.79 mm in the right eye and 3.43 mm in the left eye. The axial length was 27.88 mm in the right eye and 25.92 mm in the left eye (IOL-Master). The number of corneal endothelial cells was 1542/mm2 in the right eye and 2298/mm2in the left eye before surgery. The ICL power of the right eye was a spherical lens of a power of -14.0 D and crossed cylinder of a power of +3.0 D with axes at 110°, a length of 12.6 mm,and a residual spherical equivalent (SE) of -0.1 D. The power of the left eye was a spherical lens of a power of -9.0 D and a crossed cylinder of a power of +1.5 D with axes at 72°, a size of 12.6 mm, and a residual SE of 0.7 D.
The TICL implantation combined posterior capsulectomy surgery in the right pseudophakic eye was performed at 1wk before the left phakic eye was treated. No intraoperative complication was observed during the operation. The patient was examined at 1d, 1wk, and 12mo after surgery. One day after TICL V4c implantation surgery, the uncorrected distance visual acuity (UDVA) in the right eye improved from 1.4 preoperatively to 0.1 postoperatively. Slit lamp examination showed a middle ACD, the ICL in the sulcus with the IOL in the capsular bag, and posterior capsulorrhaphy in the right eye.The anterior segment optical coherence tomography (OCT)of the right eye showed the ICL V4c implanted between the ciliary sulcus well with open angle, and the vault was 840 μm(Figure 1B). The UDVA improved from 0.6 to 0 in the left eye.Slit lamp examination showed a quiet anterior chamber and the ICL in the sulcus with the crystal lens in position. The anterior segment OCT revealed the ICL V4c implanted between the ciliary sulcus well with open angle, and the vault was 550 μm(Figure 1C)
At the one year follow-up after surgery, no adverse events,such as lens rotation or cataract formation, were found, and visual acuity improved (Figure 2). The number of corneal endothelial cells was 1450/mm2 in the right eye and 2250/mm2in the left eye. The refractive errors were 0.25 DC×100° with a UDVA of -0.1 in the right eye and 0.25 DC×80° with a UDVA of -0.1 in the left eye. The anisometropia and astigmatism of both eyes were reduced to asymptomatic levels, and no significant difference was found between the pseudophakic eye and the other phakic eye.
The most interesting finding in this case is toric ICL implantation may be a better choice for correcting pseudophakic anisometropia than IOL exchange and piggyback IOL implantation after unilateral traumatic cataract surgery in adult patient.
IOL exchange for correcting pseudophakic ametropia has a high risk of damage to the capsular bag and zonules with subsequent vitreous loss and retinal detachment when improper surgical manipulations are performed following a long-term primary operation[5]. Furthermore, IOL exchange also fails to correct binocular anisometropia simultaneously because the other phakic myopic eye with crystal-line lens is not a candidate for lens replacement in the reported case.

Figure 1 The preoperative anterior segment picture of the right eye (A) and the anterior segment OCT of both eyes at 1d postoperatively The ICL V4c implanted well in the sulcus with open angles with the vaults of 840 μm (B) and 550 μm (C).
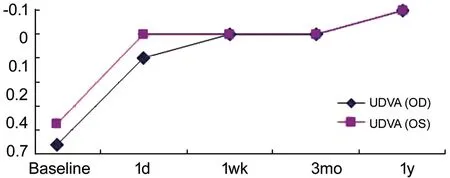
Figure 2 UDVA of both eyes after TICL V4c implantation at the one year follow-up after surgery UDVA: Uncorrected distance visual acuity; TICL: Toric visian implantable collamer lens.
Traditional anterior chamber IOLs have a high risk of endothelial cell loss, require a large incision for insertion,and have problems with pupil ovaling[6]. The technique for implanting two IOLs in the capsular bag is described as“piggyback IOL”; nevertheless, it involves high potential risks of intraocular pressure increase, IOL shift, and pupil capture[7].The implantation of an ICL in the posterior chamber seems to be safer than classic piggyback IOL, given that the large space between the ICL and the previous IOL may help prevent secondary opacification[8]. The innovative central hole design of ICL V4c may help maintain the IOP without a peripheral iridotomy in ICL V4c implantation[9]. Importantly, the current model TICL V4c also allows astigmatism to be simultaneously corrected[10].
Our case suggests that TICL may be a safe, effective, and predictable alternative for the management of unilateral pseudophakic anisometropia.
ACKNOWLEDGEMENTS
Foundations:Supported by Key Research and Development Program of Shaanxi Province (No.2020SF-271; No.2017SF-273).
Conflicts of Interest: Wang CY,None;Wang L,None;Hua X,None;Li G,None;Li Y,None;Wu LA,None.
 International Journal of Ophthalmology2021年11期
International Journal of Ophthalmology2021年11期
- International Journal of Ophthalmology的其它文章
- Angle-closure glaucoma with attenuated mucopolysaccharidosis type l in a Chinese family
- Novel biallelic compound heterozygous mutations in FDXR cause optic atrophy in a young female patient: a case report
- A novel temporary keratoprosthesis technique for vitreoretinal surgery
- Human umbilical cord-derived mesenchymal stem cells treatment for refractory uveitis: a case series
- lntroduction of longstanding complicated sulcus intraocular lens into the intact capsular bag
- Applications of dynamic visual acuity test in clinical ophthalmology