Effects of acupuncture plus language training on language function and cerebral blood flow in patients with motor aphasia after ischemic stroke
2021-10-27 08:27:32WeiJianhua衛(wèi)建華JiangTongbo蔣同伯XuMin許敏LiJingmin李京民
Wei Jian-hua (衛(wèi)建華), Jiang Tong-bo (蔣同伯), Xu Min (許敏), Li Jing-min (李京民)
Huai’an Hospital of Traditional Chinese Medicine, Jiangsu Province, Huai’an 223000, China
Abstract
Keywords: Acupuncture Therapy; Governor Vessel; Speech Therapy; Ischemic Stroke; Cerebrovascular Disorders;Poststroke Syndrome; Aphasia, Broca; Cerebrovascular Circulation
Motor aphasia, or expressive aphasia, is a common manifestation of ischemic stroke. It often happens when the rear of the inferior frontal gyrus (Broca’s area) on the dominant side is affected, mainly showing disturbed oral expression[1-2]. People with motor aphasia caused by ischemic stroke usually present with less speech,difficulty with oral expression, pronunciation and intonation, and trouble finding the correct word, greatly affecting patients’ everyday life[3]. Currently, language training is adopted in Western medicine as the major method to improve patient’s oral expression and communication abilities, as well as the quality of life[4].But the treatment result is full of uncertainty since it is greatly associated with patient’s compliance, treatment intensity and duration of treatment, let alone the long treatment process[5]. In recent years, research has found that acupuncture-moxibustion can comparatively shorten the disease duration and improve the quality of life in treating motor aphasia after ischemic stroke,presenting with significant advantage[6]. The Governor Vessel is closely related to the brain. Acupuncture at the Governor Vessel plays a crucial role in the treatment of various central nervous diseases such as cerebral stroke,Parkinson’s disease and senile dementia[7]. This study adopted acupuncture at the Governor Vessel acupoints plus language training to treat motor aphasia after ischemic stroke, during which patients’ language function and cerebral blood flow were observed. The report is given as follows.
1 Clinical Materials
1.1 Diagnostic criteria
The China Guideline for Cerebrovascular Diseases Prevention and Treatment[8]was referred to make the diagnostic criteria for ischemic stroke, and CT or MRI examination was used to confirm the diagnosis.
The Chinese aphasia examination scale[9]was referred to establish the diagnostic criteria for motor aphasia:clinically featured by oral expression disturbance,substantially normal oral comprehension, along with hindered reading and writing abilities; CT or MRI examination revealed damages in the posterior inferior frontal gyrus and its adjacent areas.
1.2 Inclusion criteria
Conformed to the diagnostic criteria for ischemic stroke, in a remission stage and with a stable condition;conformed to the diagnostic criteria for motor aphasia;ages between 35-70 years old; left hemispheric stroke;signed the informed consent form.
1.3 Exclusion criteria
With hearing, vision or cognitive impairment; lefthanded; accompanied by severe renal insufficiency,cardiac insufficiency, or respiratory failure; received other treatments in the previous 2 weeks, which may affect the observation in this trial; pregnant women or women during lactation period.
1.4 Dropout and rejection criteria
People with poor compliance and failed to follow the treatment plan; those quitted halfway; cases with serious adverse reactions; worsened or aggravated cases or deaths; those with incomplete medical data that may affect efficacy evaluation.
1.5 Statistical methods
SPSS 20.0 statistical software was adopted for data analysis. Chi-square test was used for numeric data. The measurement data conforming to normal distribution and homogeneous variance were expressed as mean ±standard deviation (±s), and checked with pairedttest in intra-group comparisons andt-test in betweengroup comparisons; those not conforming to normal distribution or homogeneous variance were expressed as median (minimum, maximum) [M (Min, Max)] and checked with non-parametric test. Ranked data were analyzed using non-parametric test.P<0.05 indicated statistical significance.
1.6 General data
Eighty-six eligible hospitalized patients were recruited from our hospital between January 2018 and December 2019. They were divided into a control group and an observation group using the random number table method, with 43 cases in each group. The control group had 3 dropout cases versus 2 in the observation group.The finally included subjects were statistically equal comparing gender, age, disease duration and education level between the two groups (allP>0.05), suggesting the comparability (Table 1).

Table 1. Comparison of the general data
2 Treatment Methods
The two groups were provided with symptomatic treatments including anti-platelet aggregation,improving microcirculation, and nutritional support for cranial nerves, as well as blood pressure and glucose control.
2.1 Control group
Schuell stimulation therapy was employed for language training. After learning about patient’s life experiences and hobbies, the therapist would give olfactory, auditory, tactile and visual stimuli with the contents well-accepted by the patient. The stimulation content, mode and intensity were increased gradually.When patient was unable to give the right response, the therapist should provide certain assistance[10]. The training lasted for 30 min each day and was conducted for 8 weeks. Under a stable condition, the patient could be transferred to the rehabilitation department for treatment to better stick with the treatment plan during hospitalization.
2.2 Observation group
In addition to the treatment given to the control group,acupuncture at the Governor Vessel acupoints was offered to the observation group.
Acupoints: Shuigou (GV 26), Shenting (GV 24), Baihui(GV 20), Yamen (GV 15), Fengfu (GV 16) and Dazhui(GV 14).
Operation: Hwato brand disposable sterile acupuncture needles (Suzhou Medical Appliance Factory,China) of 0.25 mm in diameter and 25 mm in length were selected. Patient was asked to lie on his side to expose the acupoints; after routine sterilization, Shuigou (GV 26)was punctured obliquely upward by 10-15 mm; Shenting(GV 24) and Baihui (GV 20) were inserted subcutaneously forward by 5-10 mm; Yamen (GV 15),Fengfu (GV 16) and Dazhui (GV 14) were punctured perpendicularly by 10-20 mm. When needling qi was obtained, bird-pecking manipulation was performed at Shuigou (GV 26) and even reinforcing-reducing manipulation at the other points. The needles were retained for 30 min. The acupuncture treatment was performed once every other day for a total of 8 weeks.
3 Therapeutic Efficacy Observation
3.1 Observation items
3.1.1 Aphasia battery of Chinese (ABC)The two groups were tested using the ABC before and after treatment to assess the language function including six parts, i.e. spontaneous speech, comprehension,repetition, naming, reading and writing. A higher score indicates a better language function[11].
3.1.2 Chinese functional communication profile (CFCP)The patients were scored using the CFCP before and after treatment. The CFCP reveals the everyday verbal communication ability using 25 items with a full score of 250 points. The higher the score, the better the communication ability[12].
3.1.3 Cerebral blood flow parameters
Transcranial color Doppler was adopted to examine cerebral blood flow before and after treatment. The mean velocity (Vm) and resistance index (RI) of the middle cerebral artery of the left side were recorded.
3.2 Efficacy criteria
The increase rate of ABC general score (the sum of the six component scores) was taken to evaluate the efficacy[13]. ABC general score increase rate = (Posttreatment ABC general score - Pre-treatment ABC general score) ÷ Pre-treatment ABC general score × 100%.
Substantially recovered: ABC general score increase rate ≥90.0%.
Markedly effective: ABC general score increase rate≥60.0% but <90.0%.
Effective: ABC general score increase rate ≥30.0% but<60.0%.
Invalid: ABC general score increase rate <30.0%.
3.3 Results
3.3.1 Dropouts
During treatment, there were 3 dropout cases in the control group: 1 case was due to poor compliance and receiving other treatments and 2 cases withdrew on their own due to family or work matters. The observation group had 2 dropout cases: 1 case was because of receiving other treatments and the other quitted due to family matters. Finally, 40 cases in the control group and 41 cases in the observation group were included for data analysis.
3.3.2 Comparison of efficacy
The total effective rate was 92.7% in the observation group, higher than 62.5% in the control group (P<0.05),(Table 2).
3.3.3 Comparison of the ABC scores
Prior to treatment, there were no significant differences in the ABC component and general scores between the two groups (allP>0.05). After treatment,the scores of spontaneous speech, comprehension,repetition, naming and writing, as well as the ABC general score increased in the control group (allP<0.05),while the score of reading didn’t show significant change(P>0.05); the ABC component and general scores increased after treatment in the observation group (allP<0.05), and were all higher than in the control group (allP<0.05), (Table 3).

Table 2. Comparison of therapeutic efficacy (case)
Table 3. Comparison of the ABC scores ( ±s, point)

Table 3. Comparison of the ABC scores ( ±s, point)
Note: BT=Before treatment; AT=After treatment; SS=Spontaneous speech; compared with the same group before treatment, 1) P<0.05;compared with the control group after treatment, 2) P<0.05
Group n Time SS Comprehension Repetition Naming Reading Writing General score Observation 41 BT 17.56±1.69 164.44±9.17 25.12±2.81 23.97±4.47 37.02±3.98 8.80±2.24 276.93±12.20 AT 30.27±1.571)2) 196.63±10.431)2) 74.54±14.081)2) 49.56±5.151)2) 61.71±8.231)2) 32.54±4.441)2) 445.24±17.391)2)Control 40 BT 17.38±1.84 167.05±9.34 25.58±2.93 24.73±3.37 36.48±4.62 8.83±2.35 280.03±10.92 AT 27.48±1.761) 185.90±9.701) 60.18±12.501) 45.13±3.311) 38.00±4.14 10.93±2.851) 367.60±19.191)
3.3.4 Comparison of the CFCP score
There was no significant difference in the CFCP score between the two groups prior to treatment (P>0.05).After treatment, the CFCP score increased in both groups(bothP<0.05), and was higher in the observation group than in the control group (P<0.05), (Table 4).
3.3.5 Comparisons of Vm and RI of the left-side MCA
Before treatment, there were no significant betweengroup differences in Vm and RI of the left-side MCA (bothP>0.05). Vm of the left-side MCA increased after treatment in the control group (P<0.05), but there was no significant change in RI (P>0.05); Vm of the left-side MCA increased and RI decreased after treatment in the observation group, presenting with statistical significance (bothP<0.05), and were markedly different from those in the control group (P<0.05), (Table 5).
Table 4. Comparison of the CFCP score ( ±s, point)

Table 4. Comparison of the CFCP score ( ±s, point)
Note: Compared with the same group before treatment, 1) P<0.05;compared with the control group after treatment, 2) P<0.05
Group n Pre-treatment Post-treatment Observation 41 124.41±14.78 208.46±18.811)2)Control 40 125.60±13.96 174.90±22.341)
Table 5. Comparisons of Vm and RI of the left-side MCA( ±s)
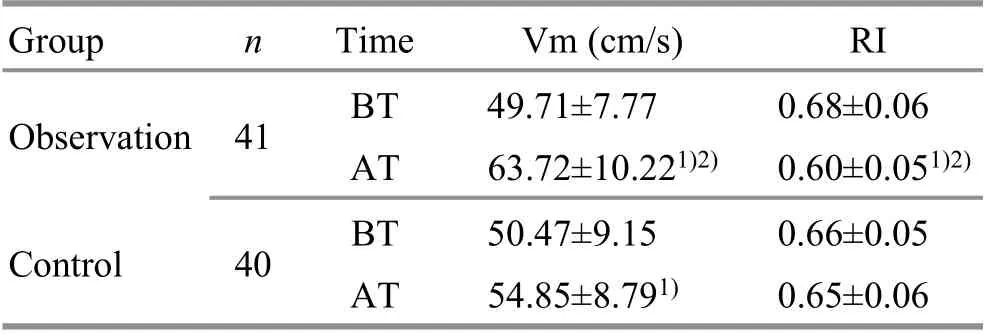
Table 5. Comparisons of Vm and RI of the left-side MCA( ±s)
Note: BT=Before treatment; AT=After treatment; compared with the same group before treatment, 1) P<0.05; compared with the control group after treatment, 2) P<0.05
Group n Time Vm (cm/s) RI Observation 41 BT 49.71±7.77 0.68±0.06 AT 63.72±10.221)2) 0.60±0.051)2)Control 40 BT 50.47±9.15 0.66±0.05 AT 54.85±8.791) 0.65±0.06
4 Discussion
Motor aphasia is a type of non-fluent aphasia, also the most common aphasia type, mostly due to MCA infarction or hemorrhage in the dominant hemisphere[14].For the vast majority of people, the dominant hemisphere is the left side, and thus the left-side MCA occlusion is more often seen in motor aphasia, in which the most significant feature is that the auditory comprehension is comparatively normal while the oral expression is greatly impaired[15]. It is generally accepted that the mechanism of language function repair after ischemic stroke includes the brain network reconstruction around the lesion and the compensation of the language function in the parallel zone in the nondominant hemisphere[16]. Therefore, promotion of neural function compensation and reconstruction is considered as the main target in treating post-stroke motor aphasia.
Prompt language rehabilitation training is required as soon as the stroke is stable, to accelerate the compensation, help with the recovery of neural function,and also prevent from the atrophy of tongue, pharynx and throat muscles. As the most popular language training method, Schuell stimulation therapy applies to various types of language dysfunction. Based on auditory stimulation, it combines multi-channel stimuli, visual,tactile, etc., to boost the reconstruction and recovery of the damaged verbal sign system to the maximum extent through repeated and more and more intensive training[17].
In traditional Chinese medicine, motor aphasia after ischemic stroke can be classified into the scopes of ‘Yin Fei’ or ‘Feng Fei’. It majorly affects the brain, but is also associated with other organs such as the heart, liver and kidney, with deficiency in the root and excess in the superficial manifestations. Deficiency is usually found in the heart, liver, spleen and kidney, while the excess superficial manifestations include blood stasis, liver wind and phlegm turbidity which block the brain orifices. All the factors together cause brain damage, and subsequent cerebral dysfunction, and impaired language zone, finally leading to aphasia. Hence, awakening the brain, regulating the mind and opening the orifices should be the basic treatment principle[18].
The Governor Vessel goes to the brain, connecting the kidney and heart, closely related to this disease. Besides,the Governor Vessel is the sea of yang meridians,governing yang qi of the whole body, and thus it is the main route for yin essence and yang qi to enter the brain.Since the Governor Vessel plays a significant role in bridging the brain and Zang-fu organs and meridians for qi-blood transportation, so there is a saying that the Governor Vessel can be selected first to treat brain diseases[19]. Selecting the Governor Vessel to treat nervous system disorders is to unblock the Governor Vessel, regulate the mind, and awaken the brain and open the orifices. In this trial, Governor Vessel acupoints including Shuigou (GV 26), Shenting (GV 24), Baihui(GV 20), Yamen (GV 15), Fengfu (GV 16) and Dazhui(GV 14) were chosen for treatment. Shuigou (GV 26) can connect the meridian qi between the Governor Vessel and Conception Vessel to harmonize yin and yang,unblock orifices, and calm the heart and mind; Shenting(GV 24) is the crossing point of the Bladder Meridian of Foot Taiyang, Stomach Meridian of Foot Yangming and Governor Vessel, acting for calming and refreshing;Baihui (GV 20) also can open the orifices, refresh the mind, and upraise the clear qi to improve central neural function and blood circulation; Yamen (GV 15) is the crossing of the Governor Vessel and Yang Link Vessel,often selected to treat hoarse voice, aphasia and mental disorders; as another crossing point of the Governor Vessel and Yang Link Vessel, Fengfu (GV 16) functions to refresh the brain, open orifices, quench the wind and calm the mind; Dazhui (GV 14) works to supplement the deficiency and calm the mind and is a key point in the treatment of mental disorders. The above acupoints work together to produce a joint effect in unblocking the Governor Vessel, refreshing the brain, reinforcing the marrow and regulating the mind, opening orifices and recovering the speech function.
ABC test was adopted in this study to evaluate the patients’ language function. This is a test made based on the real conditions in China by referring the Western aphasia battery and Boston diagnostic aphasia examination. It consists of 6 sections, i.e. spontaneous speech, comprehension, repetition, naming, reading and writing. This test can be used to differentiate the aphasia type and assess the residual language function, and has become the most popular clinical tool to evaluate the language function in China[20]. This study showed that the total effective rate was higher in the observation group than in the control group (P<0.05); the scores of spontaneous speech, comprehension, repetition,naming, reading and writing and the ABC general score all increased after treatment in the observation group(allP<0.05), and were higher than in the control group(allP<0.05). This suggests that acupuncture at the Governor Vessel acupoints plus language training is effective in treating motor aphasia after ischemic stroke and can significantly improve the language function.
The CFCP reflects the residual verbal ability and everyday communication level. The content of the test is very much associated with daily life and it has no special requirement with the testing environment and takes a comparatively shorter time, and thus is well-accepted by patients[21]. The study results demonstrated that the CFCP score increased after treatment in both groups(bothP<0.05) and was higher in the observation group than in the control group (P<0.05), indicating that acupuncture at the Governor Vessel acupoints plus language training can effectively improve the everyday verbal communication ability in the patients.
Most of the patients with motor aphasia after ischemic stroke are right-handed with the left side of the brain as the dominant hemisphere and the left-side MCA occlusion as the cause. Therefore, we examined Vm and RI of the left-side MCA in the current study. The results showed that Vm of the left-side MCA increased (P<0.05)but RI didn’t show significant change (P>0.05) in the control group, while Vm increased and RI decreased in the observation group (bothP<0.05) and were significantly different from those in the control group(bothP<0.05). This suggests that acupuncture at the Governor Vessel acupoints plus language training can strengthen the cerebral blood perfusion in patients with motor aphasia after ischemic stroke.
In summary, acupuncture at the Governor Vessel acupoints plus language training is effective in treating motor aphasia after ischemic stroke. It can notably improve the language function, daily verbal communication ability and cerebral blood perfusion in the patients. However, this study was restricted by small sample size, single source of subjects and lack of followup. Hence, large-sample high-quality clinical studies based on multiple centers are expected in the future to provide stronger clinical evidence to support this conclusion.
Conflict of Interest
The authors declare that there is no potential conflict of interest in this article.
Acknowledgments
There was no project-fund supporting for this study.
Statement of Informed Consent
Informed consent was obtained from all individual participants.
Received: 14 September 2020/Accepted: 25 December 2020
 Journal of Acupuncture and Tuina Science2021年5期
Journal of Acupuncture and Tuina Science2021年5期
- Journal of Acupuncture and Tuina Science的其它文章
- Study on the regulatory effect of herbal cakepartitioned moxibustion on colonic CD206, AMPK and TSC2 in rats with Crohn disease
- Acupuncture combined with medication for postherpetic neuralgia affecting the head and face:a randomized controlled trial
- Tendon-regulating and bone-setting manipulation plus endurance resistance exercises for female with chronic neck pain
- Efficacy and effect on related brain-gut peptides of acupoint sticking therapy for functional dyspepsia
- Clinical observation on moxibustion therapy plus tuina in treating children with recurrent respiratory tract infections due to qi deficiency of spleen and lung
- Clinical efficacy observation of ‘Tong Du Yun Pi’manipulation for infantile diarrhea in autumn