Performance of extracorporeal membrane oxygenation in patients with fatal paraquat poisoning:grasp for straws?
2021-08-15 06:22:10MengxiaoFengYuanqiangLu
Meng-xiao Feng, Yuan-qiang Lu
1 Department of Emergency Medicine, the First Affi liated Hospital, School of Medicine, Zhejiang University, Hangzhou 310003, China
2 Department of Geriatric Medicine, the First Affi liated Hospital, School of Medicine, Zhejiang University, Hangzhou 310003, China
3 Zhejiang Provincial Key Laboratory for Diagnosis and Treatment of Aging and Physic-chemical Injury Diseases, the First Affi liated Hospital, School of Medicine, Zhejiang University, Hangzhou 310003, China
Dear editor,
Paraquat (PQ) can cause acute lung injury and irreversible pulmonary fibrosis, without specific antidotes.Respiratory failure is the main cause of death among patients with PQ poisoning.Currently, the treatment involves the use of adsorbents, intensive hemoperfusion,antioxidants, immunosuppressive therapy, respiratory support by mechanical ventilation, and other symptomatic and supportive treatments.[1-3]The mortality of patients with severe PQ poisoning remains high.More eff ective and safer therapies remain to be explored.Few studies reported performing extracorporeal membrane oxygenation (ECMO)and subsequent lung transplantation with either successful or poor clinical outcome in extremely critical patients with PQ poisoning.[4,5]This study aims to summarize the clinical experience and ref lect on the therapeutic prospect of ECMO in respiratory failure or cardiopulmonary failure caused by fatal PQ poisoning.
METHODS
We conducted a retrospective and observational study of five patients receiving ECMO on admission to the First Affiliated Hospital of Zhejiang University after PQ poisoning between 2011 and 2018.All patients were diagnosed with PQ poisoning according to their history of excessive ingestion of 20% PQ solution and strongly positive semi-quantitative urine dithionite tests.All patients had no severe related primary diseases of the heart, lung,liver, or kidney before poisoning.The treatment protocols were carried out in accordance with the principles of theDeclaration of Helsinki.
RESULTS
The baseline information and clinical characteristics of these patients are shown in Table 1.Four patients, except patient 1, had fever and only patient 5 manifested as dyspnea on admission.Symptomatic and supportive treatments were applied immediately for all five patients, such as gastric lavage, antioxidants of glutathione and acetylcysteine,immunosuppressive therapy of methylprednisolone and cyclophosphamide, stomach and liver protection, and infection control.All patients performed continuous renal replacement therapy (CRRT) and/or hemoperfusion (HP).As shown in Table 1, patient 1 ingested 150 mL PQ solution,which was far beyond the lethal dose.Vasoactive drugs of dopamine and noradrenaline were administered to improve circulatory failure immediately after poisoning.The venousarterial (V-A) ECMO was performed proactively at 21 hours after poisoning, even though she had not displayed apparent dyspnea and pulmonary abnormality, according to the computed tomography (CT) scan.Furthermore, the other four patients developed dyspnea and a sharp decline in oxygen saturation (SaO2) during hospitalization.Severe changes were observed in the bilateral pulmonary CT scan images.The life-threatening cardiac and/or respiratory failure developed and ECMO was subsequently performed.Patient 2 had sudden cardiac arrest and acute respiratory distress syndrome; therefore, V-A ECMO was performed to provide both circulatory and respiratory support.Patients 3,4, and 5 manifested symptoms as respiratory failure without circulatory failure and venous-venous (V-V) ECMO was applied.The specif ic characteristics of ECMO are shown in Table 1.
Hemorrhage is the main complication of ECMO.All patients, other than patient 4, presented hemorrhage at the site of puncture, oropharynx, lungs, or multiple organs.Notably, patient 2 displayed massive pulmonary hemorrhage during operation of ECMO and died of hemorrhagic shock after seven hours.V-V ECMO assisted patients 4 and 5 to maintain oxygenation for about ten days.Figure 1 shows the typical CT imaging manifestations after f ive days of ECMO in patient 4.However, because of high medical expenses and lack of donor lungs, both patients had to discontinue further treatments, and they died of respiratory failure and multiple organ failure (MOF), respectively.Unfortunately, all five patients did not survive.
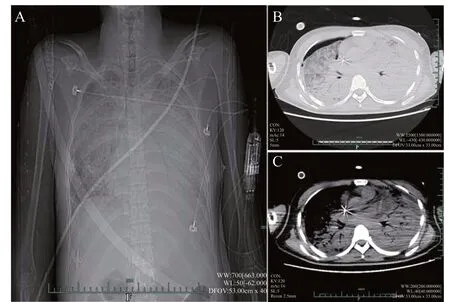
Figure 1.T ypical computed tomography imaging manifestations of patient 4 on day 5 of extracorporeal membrane oxygenation.A: X-ray indicated b ilateral pulmonary infiltration; B and C: CT images revealed bilateral pulmonary diff use exudation with partial consolidation and bilateral pleural eff usion; pneumothorax was observed in the right pulmonary.
DISCUSSION
Redox cycling is the main mechanism involved in PQ toxicity.PQ reacts with the abundant pulmonary oxygen to generate oxidative stress and deplete the body of antioxidants.[1]Therefore, oxygen therapy is usually not applied at the early stage to prevent aggravating injury by redox cycling.Previous studies have shown that ECMO has attracted more attention in severe poisoning,such as through irritant gases, PQ, and aluminum phosphide.[6-8]E CMO can preserve tissue perfusion by augmenting oxygenated venous blood via V-V ECMO,enhancing perfusion to critical organs, and improving oxygenation via V-A ECMO.L ung transplantation may be the most effective end-stage therapy, owing to irreversible pulmonary f ibrosis induced by PQ, in which ECMO can be the transitional supportive therapy.[4,9]However, because of the severity of the disease and the lack of lung sources, mortality remains high.In addition,the most common c omplication of ECMO is hemorrhage at the cannulation site in V-V ECMO or at the surgical entry site in V-A ECMO, which may increase morbidity.[8]
Our department, as a poisoning treatment center,has successfully performed ECMO for approximately 30 critical patients each year in the past eight years.Moreover, our hospital is equipped to perform lung transplantation.According to previous clinical practice and studies, rare patient has survived after ingesting 40-60 mL of 20% PQ solution.[3]Patient 1 developed circulatory failure after ingesting 150 mL 20% PQ solution.The V-A ECMO was proactively performed to maintain circulatory stability and to reduce pulmonary oxygen transport, and thereby to decrease the generation of oxygen free radicals before the appearance of significant abnormalities in her pulmonary system.However, she still died of MOF.We speculate that other mechanisms of PQ intoxication might play an important role in addition to those of oxidative stress.T he V-A ECMO showed a high risk of hemorrhage.[8]Both patient 1 and patient 2 in our study had hemorrhage.Patient 2 b led heavily during the operation of V-A ECMO and died of hemorrhagic shock.In the present study, V-V ECMO maintained ventilation and oxygenation in two patients for approximately ten days.These two patients may demonstrate the applicability of ECMO for patients with fatal PQ poisoning, although they abandoned treatments,owing to high costs and lack of donor lungs, and f inally died.Moreover, a previous study[4]has reported one successful case that ECMO could be a bridge to lung transplantation for a patient with severe PQ poisoning.T herefore, we speculate that ECMO may be just a bridge treatment for lung transplantation, other than treating severe PQ poisoning, according to these five patients’clinical outcome.
CONCLUSIONS
Further clinical verification is needed regarding the effectiveness of ECMO in patients with fatal PQ p oisoning to confirm whether EMCO i s an effective life-saving therapy or just grasp for straws.The optimal characteristics in PQ patients, as well as the timing and patterns of ECMO, should be further explored.Prohibitive costs and insuffi ciency of donor lungs are also prominent inevitable problems.In addition, clinicians should consider key points during the operation of ECMO to decrease the occurrence of complications and provide enough time for cardiopulmonary s upport.
Funding:This work is supported by the Foundation of Key Discipline Construction of Zhejiang Province for Traditional Chinese Medicine (2017-XK-A36) and the Medical and Health Science Foundation of Zhejiang Province (2019327552).
Ethical approval:This study was approved by the Ethical Committee of the First Affiliated Hospital, School of Medicine,Zhejiang University (2018369).
Conf licts of interest:No any benef its have been received from a commercial party related directly or indirectly to the study.
Contributors:MXF proposed and wrote the first draft.Both authors contributed to the design and interpretation of the study and to further drafts.
 World journal of emergency medicine2021年3期
World journal of emergency medicine2021年3期
- World journal of emergency medicine的其它文章
- Chemical pneumonitis caused by intravenous injection of insecticide spray
- Myocardial infarction detected by a smartwatch after transcatheter aortic valve replacement during the COVID-19 pandemic
- Mediastinum metastasis in a post-surgical pancreatic cancer patient successfully conf irmed with endoscopic ultrasonography
- Biphasic anaphylaxis manifested as type I Kounis syndrome induced by ingestion of raw f ish gallbladder: A case report
- Tension hydropneumothorax in a Boerhaave syndrome patient: A case report
- Intravenous haloperidol for the treatment of intractable vomiting, cyclical vomiting, and gastroparesis