Extensively drug-resistant Salmonella typhi causing rib osteomyelitis: A case report
2021-06-05 03:34:34SaraIqbalHumzaThobaniSaulatFatimi
Sara Iqbal, Humza Thobani, Saulat Fatimi
1Section of Cardiothoracic Surgery, Department of Surgery, Aga Khan University Hospital, Pakistan
2Medical College, Aga Khan University, Pakistan
ABSTRACT
KEYWORDS: Salmonella typhi; Extensive drug resistance; Rib;Osteomyelitis; Immunocompetence
1. Introduction
Salmonella (S.) enterica serotype typhi is a pathogen endemic to South and South East Asia as well as parts of Africa. The microbe causes what is often known as enteric or typhoid fever and is a common communicable disease in these regions. It may spread hematogenously to cause osteomyelitis and is a frequent etiology of osteomyelitis in immunocompromised children, such as those with sickle cell anemia. Strains of S. typhi which are resistant to ciprofloxacin and ceftriaxone-the current first-line choice of antibiotics-are increasingly being reported[1]. These extensively drug resistant (XDR) strains of S. typhi are cause for concern due to the difficulty associated with treating them, their propensity to progress to complicated infections and the widespread prevalence of typhoid fever in endemic areas[2].
This case report is exempt from requiring ethical approval as per the regulations of the Aga Khan University Ethical Review Committee. The subject of this case report has consented to this report being openly published. To the best of our knowledge, this is one of the first reported cases of osteomyelitis of the ribs in an immunocompetent adult caused by XDR S. typhi resistant to ciprofloxacin and ceftriaxone.
2. Case report
This case followed a 55-year-old female with complaints of a low-grade fever and dry, non-productive cough for the past 8 months along-with a swelling on the lower left side of her chest.She had no other pre-existing ailments or comorbidities. The patient, who lived in a rural area in Quetta, Pakistan, had sought treatment from local physicians. She reported having received several courses of antibiotics however she was unable to recall their names. None of the antibiotics succeeded in alleviating her symptoms. She also had a previous blood culture, which revealed no growth of any blood-borne microorganisms. She then presented to our hospital for further management.
On local examination, the patient had a non-mobile, 3 cm ×3 cm, soft tissue swelling with an overlying sinus discharging purulent fluid on the anterolateral portion of her lower left chest, extending from the 7th to the 9th rib. Systemic exam was unremarkable. Bacterial culture of the purulent discharge from the mass revealed S. typhi. Antimicrobial sensitivity analysis showed resistance to ceftriaxone, ciprofloxacin, ampicillin, trimethoprimsulfamethoxazole and chloramphenicol while it was sensitive to carbapenems and azithromycin. A computed tomography scan(CT scan) of chest showed marked erosion on the anterolateral portion of the 8th rib, with surrounding soft tissue thickening and inflammatory changes (Figure 1). Given these findings, a provisional diagnosis of rib osteomyelitis due to XDR S. typhi was made. The patient was electively admitted to the hospital for surgical debridement and resection of the lesion.
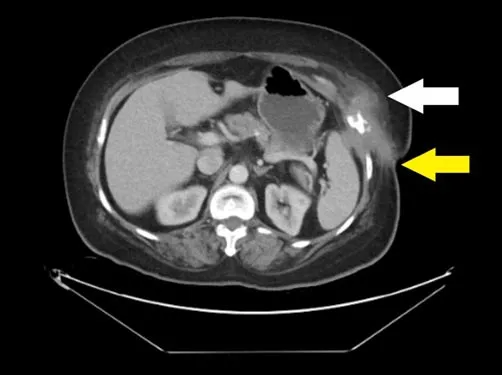
Figure 1. A CT scan axial view of the chest of a 55-year-old female who had a non-mobile, 3 cm × 3 cm, soft tissue swelling with an overlying sinus discharging purulent fluid on the anterolateral portion of her lower left chest, extending from the 7th to the 9th rib. Note the soft tissue mass on the antero-lateral portion of the left chest wall (white arrow) with a discharging sinus reaching the skin (yellow arrow).
After appropriate pre-operative preparation and optimization, the patient underwent resection of the inflamed rib-based mass under general anesthesia. Intraoperatively, an elliptical incision was made around the discharging sinus and the subcutaneous tissue around the swelling was excised. A thick, inflamed mass involving the anterolateral segments of the left 7th-9th ribs was identified and excised along with the diaphragmatic segment adherent to the internal surface of 8th rib and the overlying serratus anterior and intercostal musculature. The diaphragm was repaired, and the chest wall defect closed by suturing the surrounding myocutaneous flaps of the pectoralis major, serratus anterior and external oblique muscles. The resected samples were sent for histopathology and culture.
Postoperatively, the patient was managed on 1 000 mg ⅣMeropenem every 8 hours and 1 000 mg oral azithromycin once a day after consultation with our hospital’s infectious disease service. The culture confirmed XDR S. typhi as the cause of the osteomyelitis while acid fast bacilli cultures showed no growth.
The patient was discharged after an uneventful 4-day hospital stay, with instructions to continue the oral azithromycin for 2 days and Ⅳ meropenem for 4 days. She made a full recovery with no significant complaints and no recurrence of her initial mass on 3-month follow-up.
3. Discussion
Osteomyelitis of the ribs is an extremely rare complication of S. typhi. Such infections predominate in immunocompromised children and usually occur in the metaphysis of long bones[3],with very few reported cases in the ribs of an immune-competent adult[4,5]. What makes this case particularly interesting is that the osteomyelitis was caused by a strain of XDR S. typhi-a worrying new pathogen first reported in the city of Hyderabad in Pakistan in 2016[6]. Due to the ineffectiveness of first line antibiotics(ciprofloxacin and 3rd generation cephalosporins) in treating XDR S. typhi, it has been clinically associated with a higher patient morbidity and more severe complications[7]. This is similar to our own case, wherein the patient’s infection had persisted and eventually metastasized to the rib in spite of her receiving prior treatment.
The challenge of treating XDR S. typhi is particularly evident in lower-middle income countries such as Pakistan where healthcare is largely delivered in small rural centers with limited diagnostic capabilities. Our tertiary care institution had the capability to process the blood cultures, antimicrobial sensitivity analyses and other various diagnostic tests required to treat patients. However,such resources are often not available throughout the country,leading to mismanaged cases of XDR S. typhi, prolonged infections and further proliferation and spreading of the disease, as seen with our patient. To make matters worse, strains with decreased susceptibility to azithromycin have been reported recentlyindicating that more resistant strains of S. typhi will likely arise in the near future[8].
We demonstrated that aggressive surgical debridement combined with carefully targeted antimicrobial therapy can successfully treat XDR S. typhi osteomyelitis of the ribs and prevent recurrence of the infection. Furthermore, the early identification and appropriate treatment of XDR strains is crucial, especially given the high reported prevalence of XDR S. typhi[9], in order to avoid complications such as the one we reported. In addition, while treatment for S. typhi is likely to become increasingly difficult,significant steps have been made towards its prevention with the development of typhoid conjugate vaccines. These have been found to be immunogenic in children and provide a long-term immune response without the need for frequent revaccinations[8].As XDR S. typhi spreads through densely populated urban areas in Pakistan and India, the case for widespread vaccination only grows stronger. However, as infections and their associated resistances continue to proliferate, physicians across the country are set to face an increasingly difficult task fighting off what was once an easily manageable illness.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Authors’ contributions
SI conceptualized this case report and provided all relevant case details. SI and HT participated in writing the manuscript and collecting patient data. SF provided mentorship and oversight,expert professional feedback and reviewed/edited the final manuscript.
登錄APP查看全文
 Asian Pacific Journal of Tropical Medicine
2021年5期
Asian Pacific Journal of Tropical Medicine
2021年5期
- Asian Pacific Journal of Tropical Medicine的其它文章
- Perceived susceptibility, severity, and reinfection of COVID-19 may influence vaccine acceptance-Authors' reply
- Perceived susceptibility, severity, and reinfection of COVID-19 may influence vaccine acceptance
- Successful containment of a COVID-19 outbreak in Bach Mai Hospital by prompt and decisive responses
- S gene drop-out predicts super spreader H69del/V70del mutated SARS-CoV-2 virus
- Circulation of Brucellaceae, Anaplasma and Ehrlichia spp. in borderline of Iran,Azerbaijan, and Armenia
- Morphological study and molecular epidemiology of Anisakis larvae in mackerel fish