Cystic nephroma:A bosniak III benign tumor in the kidney
2021-05-27 15:54:58KeRen,XinGou
Asian Journal of Urology 2021年2期
Dear editor,
Cystic nephroma(CN)is a rare kind of tumor in the kidney,which has benign pathological features and biological behaviors but malignancy-like image manifestations.Pediatric CN is always associated with germlineDICER1
mutation and belongs to DICER1 syndrome,while adult CN which is now considered a different entity apparently has nothing to do withDICER1
mutation[1].The accurate preoperative diagnosis is of great importance in choosing proper treatment.This paper provides a case of adult CN as below.The patient was a 27-year-old female complaining left upper abdominal dull pain for nearly 2 years without gross hematuria.No special past medical history and family history were found.A palpable mass measured about 11 cm was detected in the left upper abdomen in physical examination.The blood test and urine test were both normal.Ultrasonic inspection showed a 15 cm mass with mixed echo in the left kidney,and enhanced computed tomography(CT)confirmed it was a complex solid-cystic mass,with a maximum diameter of 15.6 cm(Fig.1).Measurable enhancement was found in the cyst wall and septa in the aterial phase,which was more intensified in the venous phase.According to Bosniak Classification Criteria,the cystic mass could be categorized as Bosniak type III.No abnormalities were found in the lung,the thyroid,the brain and the ovary based on physical examination and image.Finally,the patient was clinically diagnosed as renal cell carcinoma(cT2b),and its RENAL score was 3+3+3+X+3=12X(in bosniak classification,X means cannot be classified as anterior or posterior).The main differential diagnoses included nephroblastoma,benign cystic renal mass such as CN,renal mucinous cystadenoma,etc
.Accurate diagnosis depends on postoperative pathological examination.As Bosniak type III is more likely to be malignant and surgery is recommended in most of these cases,together with its clinical stage and RENAL score,radical nephrectomy was planned.The operation went uneventfully and the round tumor measured 15 cm×13.5 cm×12 cm,with complete pseudocapsule outside.The section of the tumor comprised compact yellow stroma and cystic cavity of various sizes,with colorless transparent liquid inside the cavity.The inner surface of the cavity was smooth with no papillary structures or soft tissue adhering(Fig.2).The histopathologic examination demonstrated that the inner surface of the cavity was covered with a single layer of cuboid epithelium or squamous epithelium,with some distinctive hobnail epithelium therein,and the cyst wall was composed of proliferative fibrous tissue(Fig.3).The immunohistochemical result showed cytokeratin+(CK+),epithelial membrane antigen+(EMA+),cluster designation 10+(CD10+),renal cell carcinoma-(RCC-),estrogen receptor+(ER+),progestrone receptor+(PR+),vimentin-(VIM-),cytokeratin-high molecular weight+(CKH+),cluster designation 117-(CD117-),cytokeratin 7-(CK7-),KI67+<2%,carbonic anhydrase-IX-(CA-IX-).No malignant component was found in the mass,and the final pathologic diagnosis was CN.In order to make sure the subtype of the tumor and to avoid misdiagnosis,germline gene sequencing of the patient was performed andDICER1
mutation was not detected.This case was considered a typical adult CN with noDICER1
mutation.No recurrence was found 12 months after the surgery.CN was firstly reported in 1892 and was named renal cystadenoma at that time[2].The distinctive hobnail epithelium together with positive estrogen receptor(ER)and progestrone receptor(PR)staining in postoperative pathological examination could be regarded as its characteristic features[3].CN mainly occurs in two groups of people:Infants under the age of 24 months and middleaged women,which were traditionally regarded as two subtypes of CN.However,according to the latest edition of renal neoplasm pathological classification(World Health Organization[WHO]https://www.who.int/,2016),adult CN is regarded as part of the mixed epithelial and stromal tumor(MEST)family,while pediatric CN is now considered as a distinctive entity which is closely related toDICER1
gene mutation,or DICER1 syndrome(young patients with pleuropulmonary blastoma and other associated neoplasms,such as pediatric CN,thyroid tumor,ovary tumor,etc
)[4].Recent clinical research also found pediatric CN is morphologically,immunohistochemically,and genetically distinct from adult CN[5].The case we reported above is a typical adult CN withoutDICER1
mutation based on the postoperative confirmative examinations,and surgery is no doubt the best choice.However,preoperative accurate diagnosis of CN is difficult because of its non-specific clinical and image manifestation.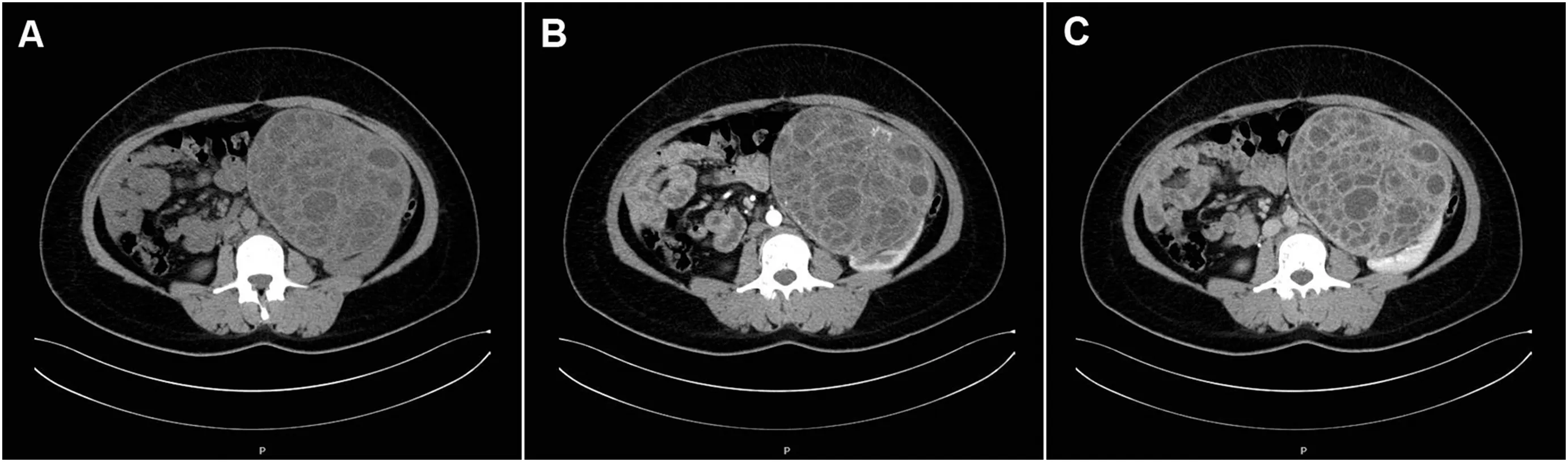
Figure 1 The CT scan imges.(A)Plain scan:The density of the solid wall ranged from 13 to 35 HU,a little higher than that of the kidney cortex which ranged from 4 to 31 HU,while the density of the cyst content ranged from-4 to 16 HU;(B)Arterial phase:Slight contrast was found in the solid wall which ranged from 20 to 81 HU while the density of the kidney cortex ranged from 37 to 167 HU,but no contrast was found in the cyst content;(C)Venous phase:The density of the solid wall ranged from 33 to 135 HU,which was higher than that in the arterial phase,while the density of the kidney cortex ranged from 31 to 112 HU,which was lower than that in the arterial phase.CT,computed tomography.
CN is different from the so-called renal mucinous cystadenoma,although they are both Bosniak III benign cystic renal neoplasm and have similar name.With regard to renal mucinous cystadenoma,the cyst content is thick mucus full of mucus protein and the inner surface of the cyst wall is always lined with a single layer of columnar epithelium with positive MUC staining but negative ER/PR staining[6].However,the cyst content of CN is mainly colorless clear thin liquid resembling serous fluid and the inner surface of the cyst wall is always lined with flat or cuboid epithelium with negative MUC staining but positive ER/PR staining[7].Pathological examination and immunohistochemistry are the key points in the differential diagnosis of these two kinds of cystic renal masses.
It is a worldwide challenge to distinguish malignant tumors from benign lesions preoperatively in those Bosniak III cystic renal masses,of which about 65% are considered to be malignant[8].Measurable enhancement(>15 HU)in the cyst wall or septa is regarded as an important malignant manifestation in contrast-enhanced CT scan,according to the Bosniak classification criteria[9].For our case,measurable enhancement in the cyst wall and septa was indeed detected in the aterial phase compared with that in the plain scan phase,but the enhancement was more intensified in the venous phase,which could be summarized as“fast-in but slow-out”.However,the typical manifestation of malignant tumors in CT scan,generally speaking,is always“fast-in and fast-out”,which means the most intensified enhancement appears in the arterial phase but not in the venous phase[10].Therefore,this tip could be regarded as a complementary to Bosniak classification in identifying malignant tumors.However,this tip is only based on the case we reported and lack of other literature evidences,so it needs more confirmation in other cohorts.
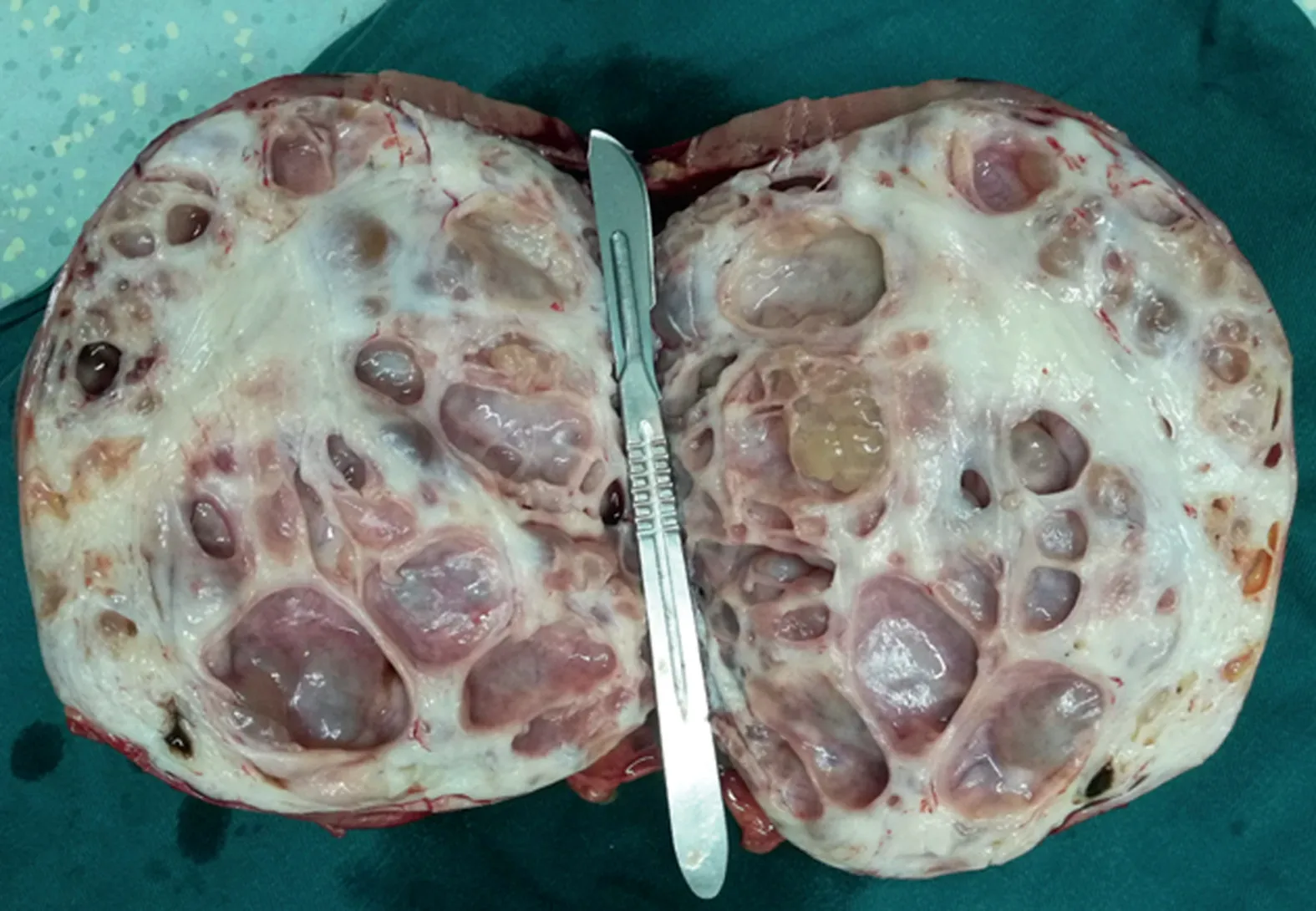
Figure 2 The section of the tumor specimen:Compact yellow stroma and cystic cavity of various sizes,with colorless transparent liquid inside the cavity.The inner surface of the cavity was smooth with no papillary structures or soft tissue adhering.

Figure 3 The pathological and immune stain result of the specimen.(A)HE 40×:The inner surface of the cavity was covered with a single layer of cuboid epithelium,with some distinctive hobnail epithelium therein;(B)HE 100×;(C)Positive ER stain,200×;(D)Positive PR stain,200×.HE,hematoxylin-eosin;ER,estrogen receptor;PR,progestrone receptor.
Referring to the case we present above,nephrectomy was inevitable even if we had known the cystic mass was benign,because of the huge size and high RENAL score of the tumor,as well as the irretrievable renal function of the left kidney.However,when treating smaller size Bosniak III renal mass for which kidney preserving surgery is technically possible,the accurate preoperative diagnosis will be of great importance and persistently challenging for us all.
Author contributions
Study design
:Xin Gou.Data acquisition
:Ke Ren,Xin Gou.Data analysis
:Ke Ren.Drafting of manuscript
:Ke Ren.Critical revision of the manuscript
:Xin Gou.Conflicts of interest
The authors declare no conflict of interest.
Acknowledgements
The authors thank Prof.Yaying Yang(Department of Pathology,Chongqing Medical University)for her technical assistance for this study.
Ke Ren
Xin Gou
Department of Urology,The First Affiliated Hospital of Chongqing Medical University,Chongqing,China
*Corresponding author.
E-mail address:
renke_rk@163.com(K.Ren)10 April 2019
 Asian Journal of Urology2021年2期
Asian Journal of Urology2021年2期
- Asian Journal of Urology的其它文章
- Super-mini percutaneous nephrolithotomy
- Are we progressing in prostate cancer management?
- Testicular germ cell tumors
- Multimodal therapy in oligometastatic prostate cancer:A glimpse into the future?
- Bilateral ureteral reconstruction using appendicular interposition combined with Wallace anastomosis following stenosis after radical cystectomy and ileal neobladder construction
- Expanding luminal epitheliums as cells of origin for prostate cancer