Review of systematic reviews of acupuncture for diabetic peripheral neuropathy
2021-04-23 09:07:46FanWeijing樊煒靜LiangShibing梁士兵HanQiang韓強HuangRenyan黃仁燕XuFeng徐烽LiuGuobin柳國斌
Fan Wei-jing (樊煒靜), Liang Shi-bing (梁士兵), Han Qiang (韓強), Huang Ren-yan (黃仁燕), Xu Feng (徐烽),Liu Guo-bin (柳國斌)
1 Shuguang Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai 201203, China
2 Center for Evidence-based Chinese Medicine, Beijing University of Chinese Medicine, Beijing 100029, China
Abstract
Objective: To review the systematic reviews of acupuncture for diabetic peripheral neuropathy (DPN) and to provide evidence for clinical decisions.
Methods: Published systematic reviews targeting acupuncture treatment of DPN were searched using computer through both Chinese and English databases till July 1, 2019. Two researchers screened the papers based on inclusion and exclusion criteria and conducted report quality evaluation, methodological quality assessment and evidence quality grading using the preferred reporting items for systematic reviews and meta-analyses (PRISMA), assessment of multiple systematic review 2 (AMSTAR 2) and grading of recommendations assessment, development and evaluation (GRADE).
Results: Ten systematic reviews were included, involving 11 outcome measures. According to PRISMA, 6 items were sufficiently reported while 1 item was not; AMSTAR 2 appraised that all the included systematic reviews were of low quality in the methodological evaluation; according to GRADE, of the 30 clinical evidences, only 5 were graded moderate while the remained were graded low or extremely low. Descriptive analysis showed that acupuncture can significantly improve DPN symptoms, accelerate the conduction velocities of sensory and motor nerves, and up-regulate the content of plasma nitric oxide (NO), while the adverse reaction rate was low.
Conclusion: Acupuncture can produce satisfactory clinical efficacy in treating DPN, but the existing problems, such as lowquality evidence, unitary outcome measures, poor methodological quality of systematic reviews and nonstandard reporting, need to be treated cautiously; meanwhile, more high-quality clinical trials are required to elevate the level of evidence.
Keywords: Acupuncture Therapy; Diabetes Mellitus, Type 2; Diabetic Neuropathies; Peripheral Nervous System Diseases;Systematic Review
Diabetic peripheral neuropathy (DPN) is one of the most common chronic complications in type 2 diabetes mellitus and also a major risk factor for diabetic foot.According to epidemiological investigation, DPN affects 60%-90% of diabetic patients, more or less. Main approaches to prevent and treat DPN include blood glucose control, improving circulation, neurorestoration,improving metabolic disorders, etc., together with nursing care and rehabilitation for lower limbs[1-2].Acupuncture can be adopted as a major treatment measure for DPN[3], since it has been proved effective in ameliorating nerve conduction velocity and promoting sensory neurorestoration[4].
More and more systematic reviews have emerged documenting acupuncture treatment of DPN, confirming that acupuncture therapy produced more significant efficacy in improving nerve conduction velocity and upregulating plasma nitric oxide (NO) content, and it was safer, compared with conventional therapy. However,the evidence level of the included studies in the existing systematic reviews was doubted. Only high-quality systematic reviews can really provide reliable evidence for clinical decisions. Therefore, this study was to sort out the relevant evidence of acupuncture treating DPN via reviewing the existing systematic reviews, in order to provide evidence for clinical decisions.
1 Materials and Methods
1.1 Inclusion criteria
1.1.1 Study type
Systematic reviews or meta-analyses of acupuncture in treatment of DPN (peer reviewed and published studies).
1.1.2 Study participants
Patients with DPN, conforming to the diagnosis criteria domestically or internationally recognized,without limitation to age, disease duration, nationality or race.
Diagnostic criteria for DPN: Numb, painful sensations and paraesthesia affected the limbs; decreased tendon reflexes and superficial sensations and limb muscle weakness; electromyogram (EMG) found decreased nerve conduction velocity; scored high by multiple peripheral neuropathy screening scales such as Toronto clinical scoring system (TCSS) and Michigan diabetic neuropathy score (MDNS)[5].
1.1.3 Interventions
The experiment group took acupuncture alone or acupuncture plus other therapies, while the control group used other therapies or placebos, or was a blank control.
1.1.4 Outcome measures
Primary outcome measures: Clinical effectiveness [the
Guiding Principles for Clinical Study of New Chinese Medicines[6]was referred, and evaluated as markedly effective, effective and invalid using the Chinese medicine symptom scores involving pain, numbness and paraesthesia] and nerve conduction velocity.
Secondary outcome measures: Adverse reactions.
1.2 Exclusion criteria
Duplicate publication; data extraction inaccessible.
1.3 Search strategy
Foreign language databases including Cochrane Library, PubMed, Science Citation Index (SCI), Springer and Embase, and Chinese databases including China
National Knowledge Infrastructure (CNKI), Chongqing VIP Database (CQVIP), Wanfang Academic Journal Fulltext Database (Wanfang) and China Biology Medicine Disc (CBM) were searched using computer from the inception till July 1, 2019. In addition, the references of the included studies were tracked to find the missing ones, and the main-stream search engines were used to retrieve grey literatures such as unpublished conference articles. Subject words and random words were combined for retrieval. The following terms,‘acupuncture’, ‘pricking’, ‘needling’, ‘needle’ ‘electroacupuncture’, ‘electroacupuncture’, ‘diabetes peripheral neuropathy’, ‘peripheral neuropathy’, ‘diabetic peripheral neuropathy’, ‘diabetic neuropathy’,‘neuropathies, diabetic’, ‘diabetic autonomic neuropathy’, ‘diabetic neuralgia’, ‘meta’, ‘systematic review’, etc., were adopted and adjusted to fit different databases. Figure 1 displays the retrieval strategy for PubMed.
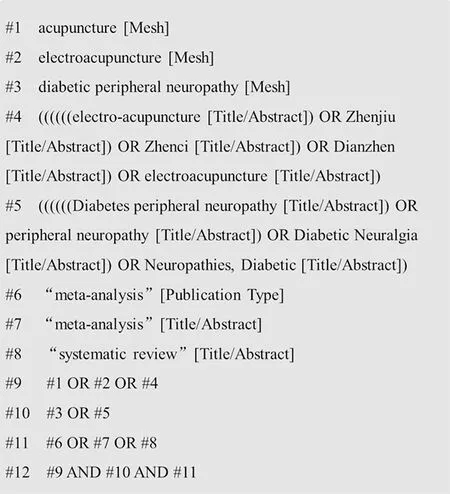
Figure 1. PubMed search strategy
1.4 Literature screening and data extraction
According to the preset research plan, two researchers independently conducted literature search, screening and data extraction. The extracted data included title,author list, publication time, literature source, inclusion criteria, exclusion criteria, outcome measures and quality evaluation methods. They would cross-check the screening results and the disagreement would be resolved by a third party.
1.5 Literature quality evaluation and statistical analysis
The methodological quality evaluation of systematic reviews was conducted using the assessment of multiple systematic review 2 (AMSTAR 2)[7]and preferred reporting items for systematic reviews and metaanalyses (PRISMA)[8], and the quality was appraised by the grading of recommendations assessment,development and evaluation (GRADE)[9].
2 Results
2.1 Literature selection process
Eighty relevant systematic reviews were identified through literature search and finally 10[10-19]were included after duplicates removal and exclusion of those targeting acupoint injection, moxibustion, and non-DPN.The screening process is shown by Figure 2.
2.2 Basic characteristics of the included studies
The included 10 systematic reviews included 1 in English and 9 in Chinese; 1 study was from SCI journal, 3 from journals indexed by Chinese Core Journal Criterion of Peking University, 4 from source journals of Chinese Scientific and Technical Papers and Citations, and 2 from state-level journals; the studies were published between 2011 and 2019. The basic characteristics of the included studies are shown in Table 1.
2.3 PRISMA
According to PRISMA, the study that reported most adequately and gained most ‘consistent’ satisfied 22 items[10], while the one gained least ‘consistent’ only satisfied 10 items[14]. The details are provided in Table 2.
Items 1, 4, 9, 14, 17 and 26 were reported most adequately and were 100% ‘consistent’; followed by items 2, 3, 6, 10, 11, 13, 20 and 21, which were 90.0%‘consistent’.
However, the reporting of item 5 was the most inadequate one, and was 90.0% ‘inconsistent’, followed by items 15 and 27, which were 40.0% ‘inadequate’.
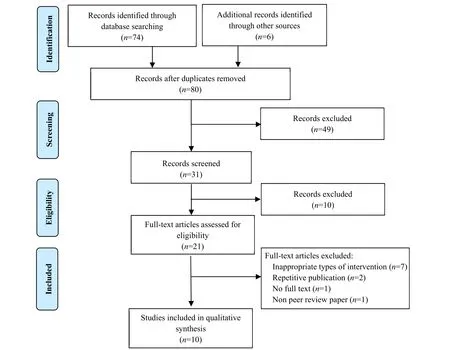
Figure 2. Literature screening process

Table 1. Characteristics of the included studies
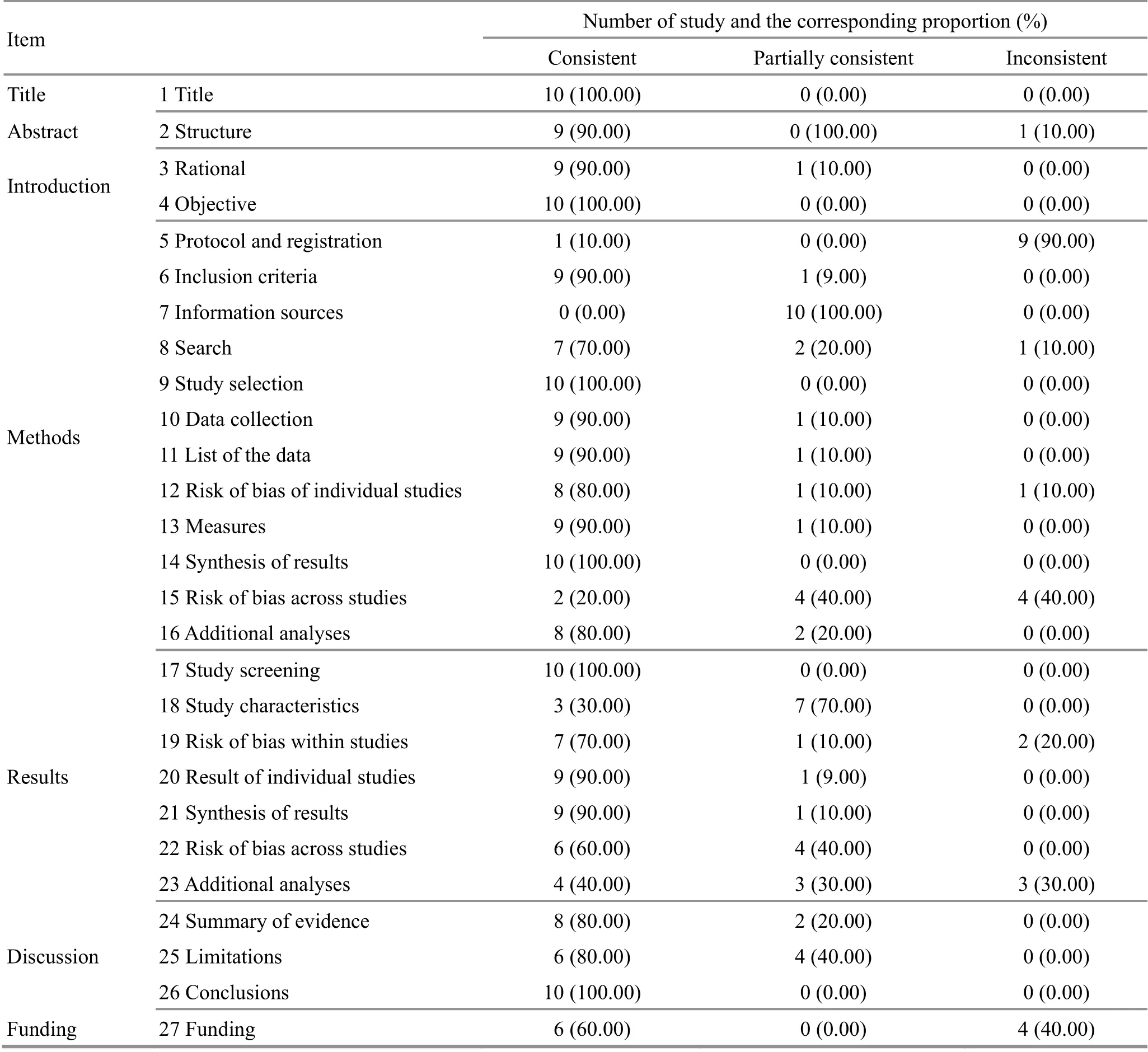
Table 2. PRISMA reporting quality assessment result
2.4 AMSTAR 2
According to MASTAR 2, each of the 10 included systematic reviews has more than one key item evaluated unqualified, and some of the reviews had one or more non-key items rated unqualified. Therefore, the quality of all the 10 reviews was estimated as critically low. In this study, the best rated study satisfied 11 items[10], while the worst one only matched 3 items[14].The included studies all reported item 1, ‘population,intervention, control group and outcome (PICO) factors in the inclusion criteria’; item 3, ‘study type’; item 5,‘study screening’. Only one English study reported item 2, ‘did the review methods establish prior to the conduct of the review and did the report justify any significant deviations from the protocol’; item 6, ‘data extraction’;item 14, ‘explanation for heterogeneity’; item 16,‘conflict of interest’. The details are provided in Table 3.
2.5 GRADE
The 10 included studies involved a total of 11 outcome measures, 30 clinical evidences. The details are provided in Table 4.
2.5.1 Total effective rate
Eight studies[10-11,13-17,19]analyzed total effective rate and concluded that acupuncture was more effective in improving DPN symptoms than the control. Of which,the evidences of 4 studies[11,13,15,17]were rated as moderate level [relative risk (RR)=4.97, 95% confidence interval (CI): 3.19-7.75,P<0.00001; RR=3.85, 95%CI:2.34-6.35,P<0.00001; RR=9.45, 95%CI: 5.95-15.02,P<0.00001; RR=1.38, 95%CI: 1.25-1.53,P<0.00001], and the other 4 as low level[10,14,16,19].
2.5.2 Sensory nerve conduction velocity
Six studies reported sensory nerve conduction velocity,including 2 on tibial sensory nerve conduction velcocity[12,19]showing that acupuncture plus medication produced more significant efficacy than using medication alone, but with low evidence level [weighted mean difference (WMD)=6.02, 95%CI: 3.87-8.16,P<0.00001; WMD=1.68, 95%CI: 1.05-2.32,P<0.00001]; 4 on median sensory conduction velocity[12-13,16-17]suggesting that acupuncture plus medication produced more significant efficacy than medication alone, but 1 with low evidence level (RR=6.20, 95%CI: 4.49-7.91,P<0.00001)[13]and the other 3 with very low evidence level[12,16-17]; 4 on peroneal sensory nerve conduction velocity[16-19]manifesting that acupuncture plus medication produced more significant efficacy than medication alone, but 1 with moderate evidence level[mean difference (MD)=3.42, 95%CI: 2.56-4.28,P<0.00001)[17], 2 with low evidence level (MD=4.10,95%CI: 0.22-7.99,P<0.05; WMD=3.34, 95%CI: 2.30-4.38,P<0.00001)[18-19]and the rest 1 with very low evidence level[16].
2.5.3 Motor nerve conduction velocity
Six studies analyzed motor nerve conduction velocity.One study reported on tibial motor nerve conduction velocity[12], showing that acupuncture plus medication produced more significant efficacy than medication alone, but was rated as very low evidence level(WMD=5.62, 95% CI: 4.49-6.75,P<0.00001); 5 studies analyzed median motor nerve conduction velocity[12-13,16-17,19], showing that acupuncture plus medication produced more significant efficacy than medication alone, 1 with low evidence level (WMD=2.81,95%CI: 1.71-3.91,P<0.00001)[16]and 4 with very low evidence level[12-13,17,19]; 4 studies analyzed peroneal motor nerve conduction velocity[16-19], manifesting that acupuncture plus medication produced more significant efficacy than medication alone, 2 with low evidence level(WMD=4.07, 95%CI: 3.27-4.86,P<0.00001; MD=3.55,95%CI: 0.79-6.31;P<0.05)[16,18]and 2 with very low evidence level[17,19].
2.5.4 Adverse reactions
One study reported adverse reactions[17], telling that no adverse reaction was found, but was rated as very low evidence level.
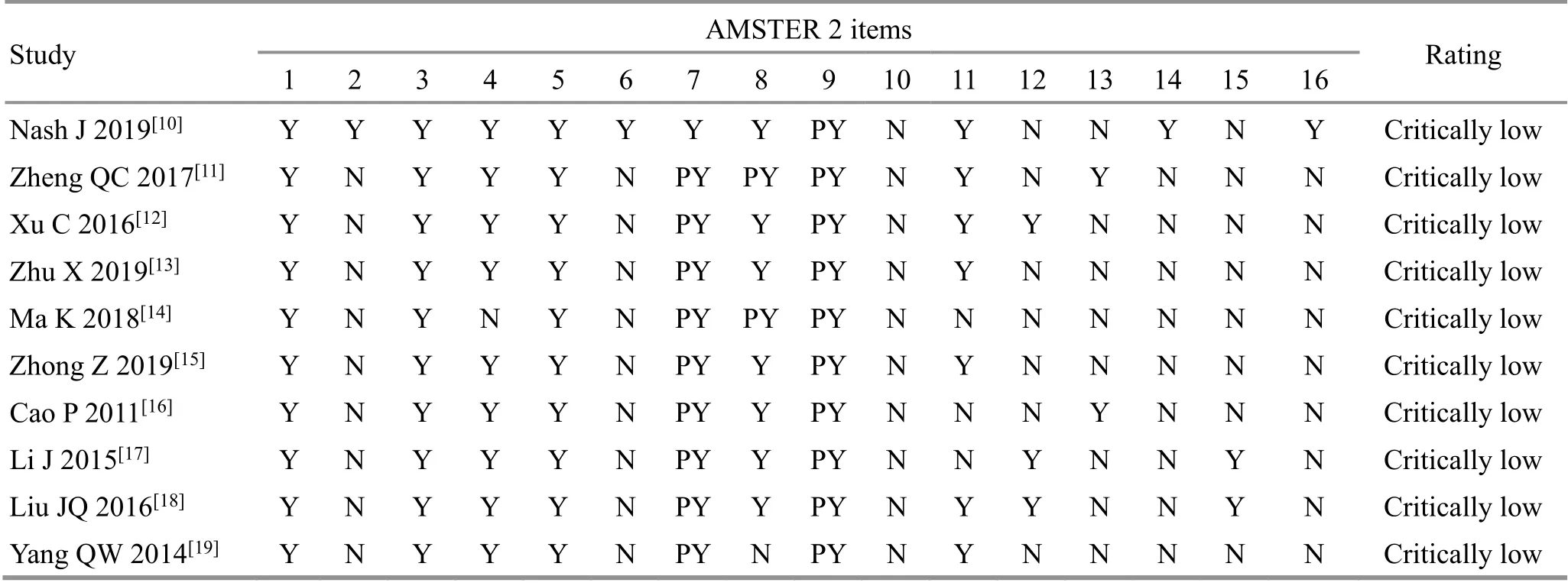
Table 3. AMSTAR 2 score of the included systematic reviews
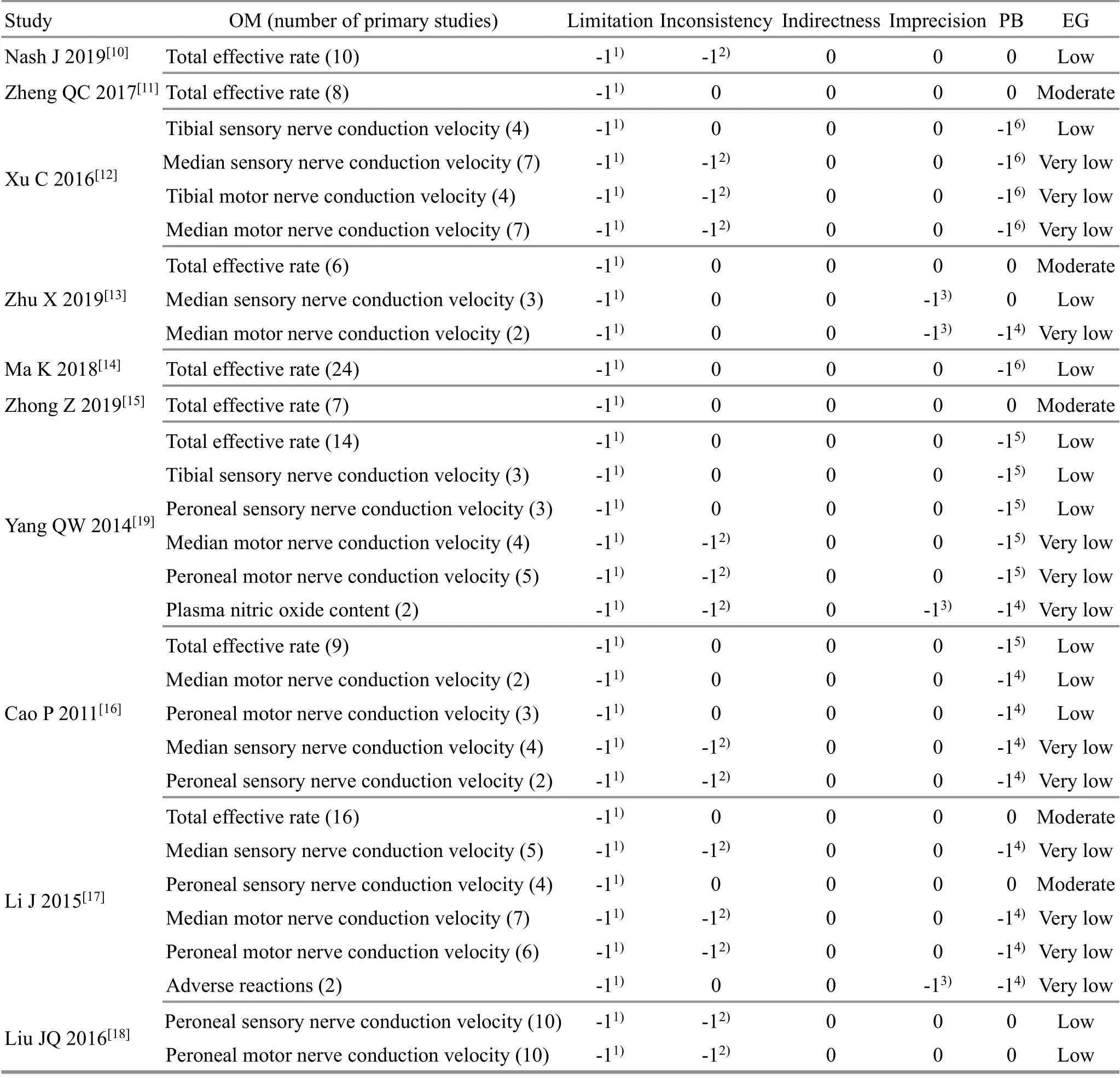
Table 4. GRADE result of the systematic reviews
2.5.5 Plasma NO content
One study analyzed plasma NO content[19]and suggested that acupuncture increased the content more significantly than medication, but was rated as very low evidence level (WMD=6.15, 95%CI: 1.84-10.46,P=0.005).
3 Discussion
As one of the most common diabetic complications,DPN is sneaky in its early stage and there are not many treatment choices for this condition. It is the major factor causing diabetic foot and even wounds on the lower limbs[19-20]. Many clinical studies have proven the effectiveness of acupuncture in releasing DPN symptoms,improving nerve function and elevating quality of life without causing notable adverse reactions[21-23].Therefore, it is of significance to conduction evidencebased studies on acupuncture treating DPN, for guiding treatment in clinical practice.
By reviewing the systematic reviews documenting acupuncture treating DPN, the present study conducted quality evaluation from multiple perspectives and finally concluded the following points.
3.1 Acupuncture was effective for DPN while the evidence was rated as low level
The included studies all confirmed the effectiveness of acupuncture in treating DPN and offered evidence proving that acupuncture was effective in ameliorating DPN symptoms, increasing the conduction velocities of sensory and motor nerves and up-regulating plasma NO content, so that patients can definitely benefited from this treatment and it should be introduced into clinical practice. However, according to GRADE, we found that the majority of clinical evidences were estimated as low or very low level, making the results less interesting references for clinicians. Meanwhile, individualized treatment features such as various acupuncture manipulations and acupoint grouping ways also result in significant heterogeneity across the included studies,which is currently a difficult issue to handle when performing studies of acupuncture-moxibustion. Hence,the design of clinical trials should consider the features of randomized controlled trial (RCT) and acupuncture treatment simultaneously[24-26].
3.2 The outcome measures adopted in acupuncture treatment of DPN were rather unitary
The present study statistically analyzed the outcome measures involved in the included reviews. Of the 11 outcome measures, plasma NO content was studied only by one review[19], and the rest were effective rate(improvement of symptoms) and nerve conduction velocity. Economical parameters and quality of life were not reviewed by any of the included studies, and few studies evaluated the safety of acupuncture. Compared with pharmacological treatment, the advantages of acupuncture therapy mainly are safety and low cost. So,it is of great significance to explore the evidence about safety and economic indicators for clinical evaluation of acupuncture-moxibustion.
3.3 The systematic reviews of acupuncture for DPN were incomplete and the methodological quality was rated relatively low
In this study, we adopted PRISMA list to evaluate the quality of the included systematic reviews and AMSTAR 2 to estimate the methodological quality. The results showed that all the reporting methods were rated as low quality. Although the report of some items was basically adequate, such as item 1, ‘the PICO factors of inclusion criteria’, item 3, ‘study type’, and item 5, ‘literature screening’, all the Chinese studies failed to register and provide the study design, neither declared the conflict of interest. Most of the studies did not offer the list of included studies, and some studies failed to conduct a complete literature search and offer the complete retrieval strategy of any database. Besides, the methodological bias has greatly influenced the quality evaluation, as all of the included systematic reviews only mentioned randomization but missed the description of the randomization method in detail, so did the report on blinding method. We would like to suggest that future systematic reviews should pay attention to the registration of study protocol, offer the list of included studies and declare the conflict of interest. In addition, a systematic review should be written in a standard way.Otherwise, it will cause trouble for future studies and undermine the credibility of the report, not benefiting the development of acupuncture-moxibustion.
Despite unveiling the above problems, this research had certain limitations. First, we only retrieved ordinary databases and main-stream search engines, but missed the protocol registration databases and the materials in paper, which may lead to selection bias. Second, both AMSTAR 2 and GRADE were somewhat based on subjective evaluation.
Regarding the above defects in the existing systematic reviews of acupuncture treatment of DPN, researchers are expected to consider about the characteristics of acupuncture therapy, improve the rigidity of RCT design and guarantee the scientificity of clinical trials; the safety and social-economic outcome measures are supposed to be introduced into the study design. Moreover,systematic reviews should enhance its methodological quality, screening primary studies in a more rigorous manner and reducing heterogeneity as far as possible; a systematic review should be registered before conduction to reduce selection bias; a systematic review is supposed to be written in a standard and objective form by strictly following the PRISMA list.
Conflict of Interest
The authors declare that there is no potential conflict of interest in this article.
Acknowledgments
This work was supported by General Project of National Natural Science Foundation of China (國家科學自然基金面上項目, No. 81774310); Youth Project of National Natural Science Foundation of China (國家自然科學基金青年項目, No. 81804095).
Received: 12 March 2020/Accepted: 10 June 2020
猜你喜歡
中國科技教育(2019年11期)2019-09-26 10:49:15
中國科技教育(2019年12期)2019-09-23 08:02:08
小小藝術家(2019年6期)2019-06-24 17:39:44
今古傳奇·故事版(2016年15期)2016-09-07 06:57:32
小雪花·成長指南(2015年3期)2015-05-04 00:04:37
投資與理財(2009年13期)2009-12-07 07:38:42
投資與理財(2009年21期)2009-11-17 09:59:46
投資與理財(2009年18期)2009-09-30 06:18:16
投資與理財(2009年16期)2009-09-03 07:03:12
投資與理財(2009年15期)2009-08-22 07:35:46
 Journal of Acupuncture and Tuina Science2021年2期
Journal of Acupuncture and Tuina Science2021年2期
- Journal of Acupuncture and Tuina Science的其它文章
- Effects of auricular point sticking on dry eye in myopia patients after SMILE surgery: a prospective randomized controlled clinical trial
- Effects of acupoint thread-embedding therapy on serum apelin and GLP-1 in type 2 diabetes mellitus patients with obesity due to dampness-heat encumbering spleen
- Nie-pinching the spine, puncturing Sifeng (EX-UE 10)plus Chinese herbs for pediatric anorexia due to dysfunction of spleen in transportation:a randomized controlled trial
- Effects of moxibustion on the P2X7R/STAT3/VEGF pathway in rats with colitis-associated colon cancer
- Evaluation of the prevention and treatment effects of acupuncture-moxibustion for Alzheimer disease based on various mouse models
- Warm needling moxibustion plus PKP for vertebral compression fracture due to kidney deficiency and blood stasis: a randomized controlled trial