Safety and efficacy of sofosbuvir/velpatasvir/voxilaprevir in postliver transplant patients with previous direct-acting antiviral failure:Six case reports
2021-01-13 05:56:52CoryHigleyChristineHsuColemanSmithSandeepNadellaAlexanderLalos
World Journal of Hepatology 2020年12期
Cory Higley, Christine C Hsu, Coleman Smith, Sandeep Nadella, Alexander T.Lalos
Cory Higley, Department of Medicine, MedStar Georgetown University Hospital, Washington, DC 20007, United States
Christine C Hsu, Coleman Smith, Alexander T.Lalos, Transplant Institute, MedStar Georgetown University Hospital, Washington, DC 20007, United States
Sandeep Nadella, Department of Gastroenterology, Medstar Georgetown University Hospital, Washington, DC 20007, United States
Abstract
Key Words: Sofosbuvir/velpatasvir/voxilaprevir; Hepatitis C; Liver transplant; Direct-acting antiviral; Drug-drug interactions; Case report
INTRODUCTION
Direct-acting antiviral (DAA) therapy regimens are highly effective at eliminating hepatitis C virus (HCV) infection but patients with decompensated cirrhosis or hepatocellular carcinoma (HCC) have been shown to have lower sustained virologic response rates (SVR)[1-3].Some of these patients with DAA treatment failure may eventually be referred for liver transplant and will require retreatment, which in many cases will be undertaken after transplantation.There is extensive published experience with DAA treatment of HCV after liver transplant, with most patients in these studies being treated with glecaprevir/pibrentasvir (G/P) and ledipasvir/sofosbuvir (L/S)[4,5].
Post-transplant treatment of hepatitis C in patients who have experienced previous DAA failure has been less well studied.The American Association for the Study of Liver Diseases–Infectious Disease Society of America (AASLD-IDSA) recently updated practice guidelines to recommend sofosbuvir/velpatasvir/voxilaprevir (SOF/ VEL/VOX) as the preferred regimen to treat HCV in DAA-experienced patients following liver transplant[1].However, this recommendation is listed as level 1, C which is based on expert consensus as there is a paucity of published experience[1].Additionally, the safety of SOF/VEL/VOX in this population, including guidance on navigating drug-drug interactions (DDI) between SOF/VEL/VOX and commonly used immunosuppressants has not been well supported in published studies.As such, we report a series of six patients with previous DAA failure who were subsequently treated successfully with SOF/VEL/VOX after liver transplant.We report our experience to emphasize the efficacy of this regimen in this population while also highlighting the safety profile.
CASE PRESENTATION
Chief complaints
Case 1:A 51-year-old African American male who presented to hepatology clinic to discuss treatment options for HCV.
Case 2:A 68-year-old Caucasian male who presented to hepatology clinic to discuss treatment options for HCV.
Case 3:A 66-year-old African American male who presented to hepatology clinic to discuss treatment options for HCV.
Case 4:A 70-year-old African American male who presented to hepatology clinic to discuss treatment options for HCV.
Case 5:A 48-year-old African American male who presented to hepatology clinic to discuss treatment options for HCV.
Case 6:A 68-year-old African American female who presented to hepatology clinic to discuss treatment options for HCV.
History of present illness
Patients in cases 1-6 had no acute complaints on initial visit.All patients were postliver transplant and had previously failed treatment of HCV.
History of past illness
Case 1:The patient had a past medical history of HCV cirrhosis complicated by HCC who underwent orthotopic liver transplantation.He had HCV coinfection with genotypes 1a and 4 that was treated with 24 wk of L/S prior to transplant however SVR was not achieved.Additionally, he received transarterial chemoembolization and transarterial radioembolization prior to transplant to downstage his HCC to meet Milan criteria.He also had a history of latent tuberculosis.
Case 2:The patient had a past medical history of HCV cirrhosis complicated by HCC who underwent orthotopic liver transplantation.He had HCV coinfection with genotypes 1 and 4 that was treated with 24 wk of L/S as well as interferon/ribavirin and sofosbuvir/ribavirin regimens prior to transplant, however SVR was never achieved.Additionally, he received transarterial chemoembolization and transarterial radioembolization prior to transplant to downstage his HCC to meet Milan criteria, however, following transplant, examination of explant revealed patient was not within Milan criteria.He also had a history of obesity, cataracts, anemia, and vitiligo.
Case 3:The patient had a past medical history of decompensated HCV cirrhosis complicated by HCC who underwent orthotopic liver transplantation.Prior decompensations included ascites and prior esophageal variceal bleed.He had HCV genotype 1b that was treated with 12 wk of L/S prior to transplant, however SVR was never achieved.He also had a history of coronary artery disease, hypertension, chronic sinusitis and vitamin D deficiency.
Case 4:The patient had a past medical history of HCV cirrhosis complicated by HCC who underwent orthotopic liver transplantation.The patient had HCV genotype 1b that was treated with 12 wk of L/S prior to transplant, however SVR was never achieved.He also had a history of hypertension, diabetes mellitus and latent tuberculosis.
Case 5:The patient had a past medical history of decompensated HCV cirrhosis complicated by HCC who underwent orthotopic liver transplantation.Prior decompensations included ascites and portopulmonary hypertension.He had HCV coinfection with genotypes 1 and 4 that was treated with 24 wk of L/S as well as 12 wk of simeprevir/sofosbuvir prior to transplant, however SVR was never achieved.He also had a history of diabetes mellitus, latent tuberculosis, and prior clostridium difficile infection.
Case 6:The patient had a past medical history of HCV cirrhosis complicated by HCC who underwent orthotopic liver transplantation.She had HCV genotypes 1a that was treated with 12 wk of L/S prior to transplant, however SVR was never achieved.She was then treated with elbasvir/grazoprevir following transplant but she again failed to achieve SVR.She also had a history of diabetes mellitus, hypertension, and hyperlipidemia.
Baseline patient demographics are included in Table 1 and patients’ prior therapies are summarized in Table 2.
Personal and family history
Case 1:The patient was a nonsmoker and did not drink alcohol.He had no relevant family history.
Case 2:The patient did not drink, smoke, or ever use intravenous drugs.Patient does not know his family history.
Case 3:Patient was a nonsmoker and denies alcohol use.His family history was negative for liver disease and otherwise noncontributory.
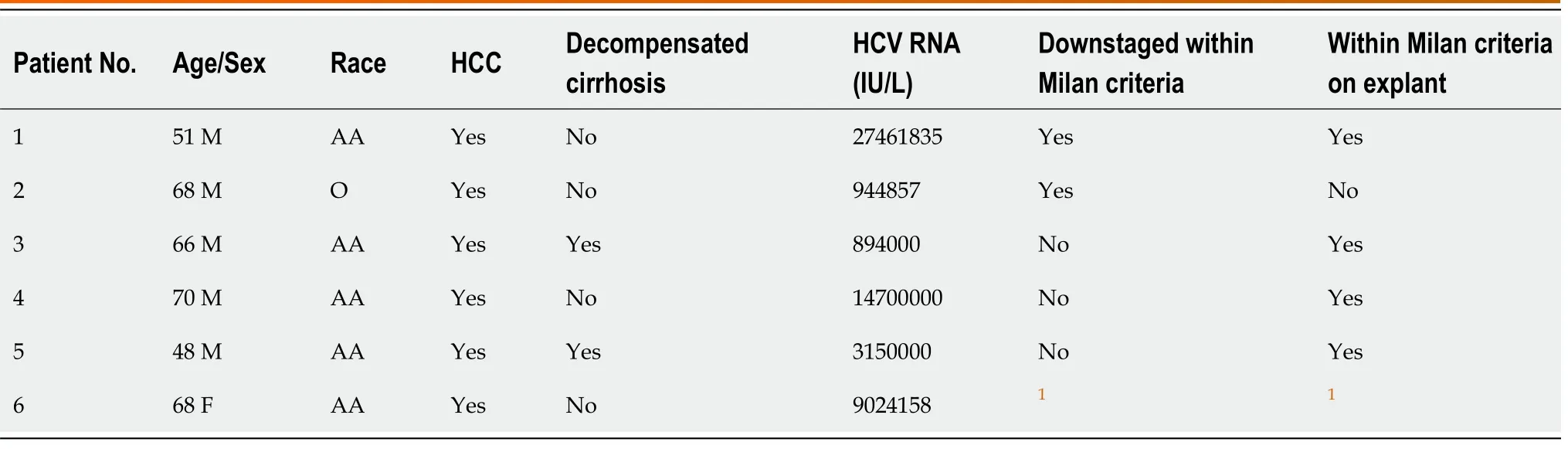
Table 1 Baseline demographics prior to sofosbuvir/velpatasvir/voxilaprevir therapy
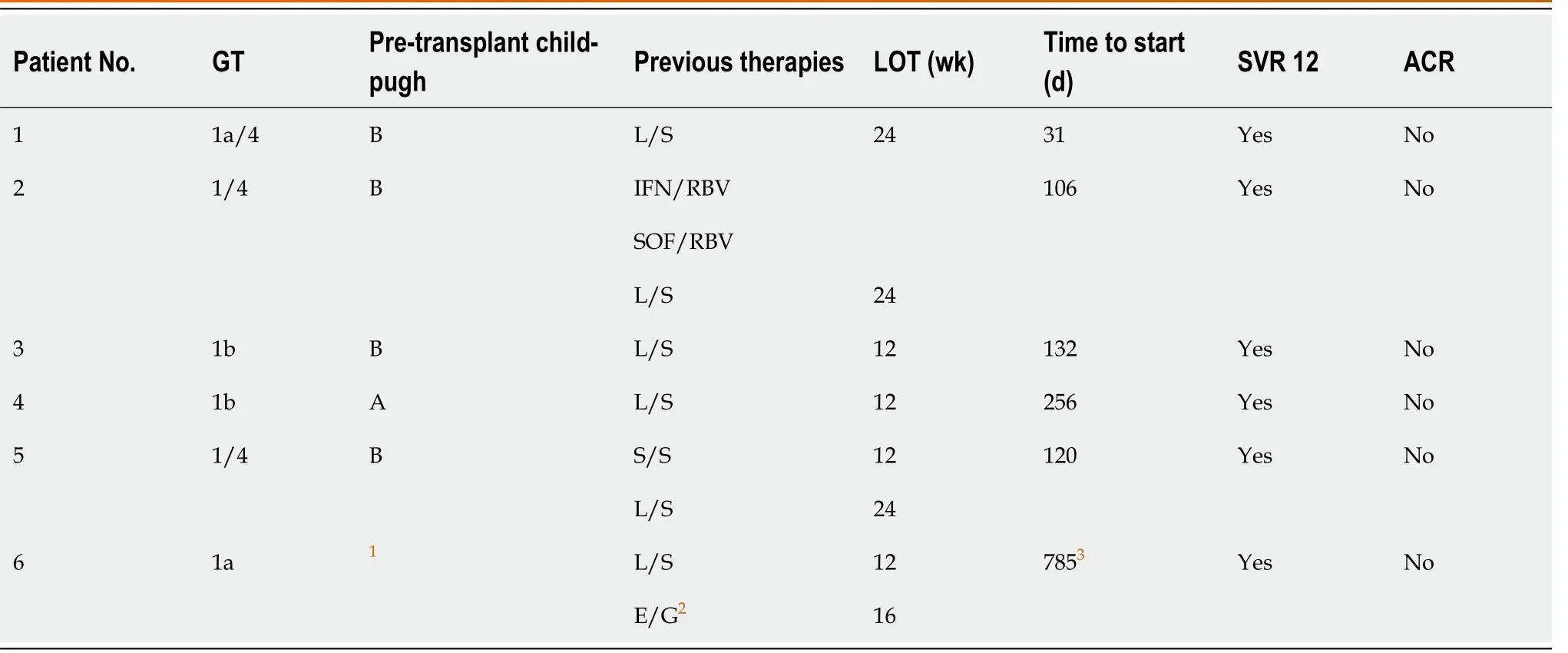
Table 2 Patients who completed sofosbuvir/velpatasvir/voxilaprevir after liver transplant
Case 4:He states he is a former intravenous drug user, smoker, and alcohol drinker.His family history is significant for diabetes mellitus and hypertension.
Case 5:The patient denies tobacco use and he will socially drink.He states both of his siblings have HCV as well.
Case 6:The patient denies recreational drug use, tobacco use, and alcohol use.Both of her parents had skin cancer.
Physical examination
On initial clinic visit, patients in cases 1-5 had physical exams notable for well-healed abdominal surgical scars.Their abdomens were soft, nontender, and without ascites.There was no jaundice or lower extremity edema.The remainder of exams was otherwise unremarkable.The patient in case 6 had similar exam but for a well-healing abdominal surgical scar with staples and Jackson-Pratt drain in still place after surgery.
Laboratory examinations
Relevant laboratory value just prior to initiation of SOF/VEL/VOX for cases 1-6 are as below.Of note, all liver grafts were from HCV antibody negative donors and nucleic acid testing for HCV was also negative.
Case 1:HCV RNA 27461835 IU/L, creatinine 1.38 mg/dL, total bilirubin 0.60 mg/dL, aspartate aminotransferase (AST) 30 units/L, alanine aminotransferase (ALT) 181 units/L, alkaline phosphatase 121 units/L.
Case 2:HCV RNA 944857 IU/L, creatinine 0.77 mg/dL, total bilirubin 0.20 mg/dL, AST 70 units/L, ALT 45 units/L, alkaline phosphatase 92 units/L.
Case 3:HCV RNA 894000 IU/L, creatinine 0.95 mg/dL, total bilirubin 0.20 mg/dL, AST 30 units/L, ALT 21 units/L, alkaline phosphatase 101 units/L.
Case 4:HCV RNA 14700000 IU/L, creatinine 0.98 mg/dL, total bilirubin 0.40 mg/dL, AST 19 units/L, ALT 14 units/L, alkaline phosphatase 84 units/L.
Case 5:HCV RNA 3150000 IU/L, creatinine 1.54 mg/dL, total bilirubin 0.18 mg/dL, AST 55 units/L, ALT 61 units/L, alkaline phosphatase 135 units/L.
Case 6:HCV RNA 9024158 IU/L, creatinine 0.74 mg/dL, total bilirubin 0.30 mg/dL, AST 18 units/L, ALT 26 units/L, alkaline phosphatase 60 units/L.
Imaging examinations
There was no imaging immediately prior to initiation of SOF/VEL/VOX for cases 1-6.
FINAL DIAGNOSIS
The patients in case 1-6 all had HCV that required treatment in the post-transplant setting.
TREATMENT
All six patients were treated with a 12-wk course of SOF/VEL/VOX, initiated at varying times in their post-transplant course with a median start date of 126 (IQR 87.3, 388.3) d after transplant.
OUTCOME AND FOLLOW-UP
After beginning treatment, 100% of the patients achieved undetectable HCV RNA levels within 4 wk.SVR12 was documented in all cases and no patient experienced a virologic relapse with mean follow up time of 505.3 ± 152.8 d.Since treatment was relatively early after transplant, no patients had suspected cirrhosis of their liver graft or clinical findings to suggest fibrosing cholestatic hepatitis, although no formal fibrosis (i.e., liver biopsy or FibroScan) testing was performed.Additionally, no patients had severe renal dysfunction, which we defined as a GFR < 30 mL/min/1.73 m3.
No patient had a serious adverse event defined as death, life-threatening episode, hospitalization, or persistent or significant disability.All patient tolerated SOF/VEL/VOX well with no specific adverse effects reported.Most important, there were no episodes of acute cellular rejection or graft loss and no documented recurrence of HCC in any patient throughout the follow-up period.One patient received a hepatitis B core positive donor has been maintained medication to prevent hepatitis B reactivation.
All patients were on a regimen of tacrolimus and mycophenolate for the first six months following transplant at which point mycophenolate was discontinued and patients were continued on tacrolimus monotherapy as per our institute’s immunosuppression protocol.Five of our patients required their tacrolimus dosing to be reduced.All changes were relatively minor and most were in the immediate posttransplant setting where dose changes are often necessary.No patient had toxic levels of tacrolimus, defined as greater than 20 ng/mL, the upper limit of normal for our laboratory.Table 3 outlines specific changes in tacrolimus dosing throughout their 12-wk course of SOF/VEL/VOX.
DISCUSSION
We present what we believe to be the first case series highlighting the safety and efficacy of SOF/VEL/VOX in post-liver transplant patients with prior DAA failure.Although DAAs typically have very high cure rates, in general, approximately fivepercent of patients with HCV treated with DAAs will not achieve SVR; these patients often have evidence of decompensated cirrhosis or HCC, as the case with our cohort[1-3].Since some of these patients may eventually require a liver transplant, we expect there will be cases of transplant recipients with previous DAA failure requiring repeat treatment after the transplant.
SOF/VEL/VOX is a well-established option to treat recurrent HCV in DAAexperienced patients, however the two phase 3 trials from which this was founded did not include liver transplant recipients[6].Despite this, SOF/VEL/VOX is currently listed as the preferred regimen for DAA-experienced patients after transplant however, we believe the data in the post-transplant population to be very limited[1].To our knowledge, we are aware of only one case report highlighting its effectiveness and safety in this setting[7].Additionally, although our study involves a small cohort, we believe this to be a comparatively large sampling as DAA failures are an uncommon event.As such, we believe this case series contributes to our understanding of efficacy, safety profile, and potential DDI for SOF/VEL/VOX in this unique and under-studied population.
We also note that SOF/VEL/VOX has not been formally studied in post-transplant patients, and is therefore not FDA-approved for use in post-transplant population.We expected this regimen to be effective and well tolerated since both G/P and L/S have been previously shown to be safe and effective after transplant[8,9].In essence, SOF/VEL/VOX is a combination of both of these regimens in terms of its anti-HCV components.Our findings do show that all patients achieved SVR12 without serious adverse events.In addition, no patient reported any adverse effects that necessitated interruption or early termination of treatment.
We were very concerned about the possibility of DDI, specifically with regards to DAAs and immunosuppressant medications.Tacrolimus remains the backbone for most liver transplant anti-rejection regimens and that is the case at our institution.While we know tacrolimus levels will typically increase with initiation of DAA regimens containing NS3/4A protease inhibitors such as G/P and E/G, there seems to be minimal data on how tacrolimus levels are influenced by SOF/VEL/VOX[1,10].The AASLD-IDSA website currently does not suggest dose reduction citing lack of data[1].As such, we paid particularly close attention to monitoring tacrolimus levels not only during initiation of SOF/VEL/VOX but also at regular biweekly intervals until completion of treatment.Table 3 shows changes to tacrolimus dosing for each patient during their 12-wk course of SOF/VEL/VOX.Five of our patients required a dosereduction in their tacrolimus; this is consistent with other DAA regimens containing NS3/4A protease inhibitors[10].Most of the tacrolimus adjustments were minor, further emphasizing the safety profile of SOF/VEL/VOX.Of note, we do not typically use cyclosporine at our institution and as such we are unable to comment on DDI between it and SOF/VEL/VOX, although prior data suggest no dose adjustments are necessary[10].
One potential limitation of this case series is the small patient cohort.Additionally, included patients are from similar demographics (gender, race, age, and city) possibility limiting generalizability of these findings.And finally, it is well known that patients who fail DAA regimens will frequently have multiple resistance association variants identified on resistance testing.We did not formally assess for these in our patients as their presence has not been shown to affect the ability to achieve SVR with SOF/VEL/VOX[11].
CONCLUSION
In conclusion, our experience supports the efficacy of SOF/VEL/VOX as an effective therapy for post-transplant treatment of HCV in patients who had previously failed DAA therapy prior to liver transplant as all treated patients achieved SVR at 12 wk.In addition, SOF/VEL/VOX appears to be safe as there were no episodes of acutecellular rejection or serious adverse events.Minor changes in tacrolimus dosing may be needed.
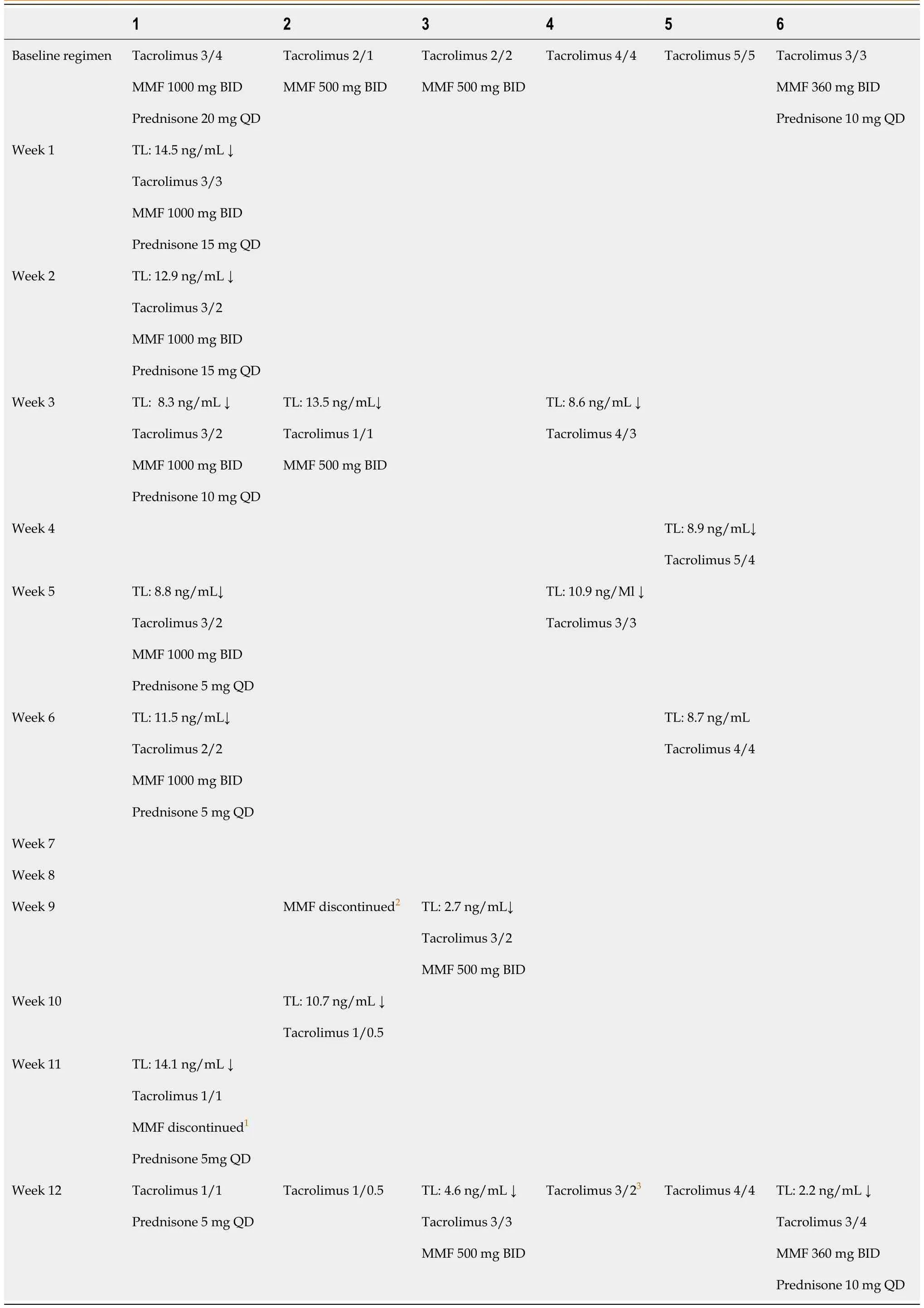
Table 3 Immunosuppressive medication changes while receiving sofosbuvir/velpatasvir/voxilaprevir
 World Journal of Hepatology2020年12期
World Journal of Hepatology2020年12期
- World Journal of Hepatology的其它文章
- Autophagy related protein 9A increase in hepatitis B virusassociated hepatocellular carcinoma and the role in apoptosis
- Hepatitis E virus re-infection accelerates hepatocellular carcinoma development and relapse in a patient with liver cirrhosis: A case report and review of literature
- Successful hepatic resection for recurrent hepatocellular carcinoma after lenvatinib treatment: A case report
- Subclinical proximal tubulopathy in hepatitis B: The roles of nucleot(s)ide analogue treatment and the hepatitis B virus
- HIPPOCRATES? project: A proof of concept of a collaborative program for hepatitis C virus microelimination in a prison setting
- Effect of non-alcoholic beer, diet and exercise on endothelial function, nutrition and quality of life in patients with cirrhosis