Ileocecal intussusception caused by two different tumors - which is the culprit lesion? A case report
2020-09-14 10:51:46WuFengFanGangMaGuiChenLiJinLongYuanHongXuKeJianGuoZheLiu
World Journal of Clinical Cases 2020年10期
關(guān)鍵詞:工程
Wu-Feng Fan,Gang Ma,Gui-Chen Li,Jin Long,Yuan-Hong Xu,Ke-Jian Guo,Zhe Liu
Wu-Feng Fan,Gang Ma,Gui-Chen Li,Jin Long,Yuan-Hong Xu,Ke-Jian Guo,Zhe Liu, Department of Pancreatic-Biliary Surgery,First Hospital of China Medical University,Shenyang 110001,Liaoning Province,China
Abstract
Key words:Adult intussusception;Two different tumors;Right hemicolectomy and cholecystectomy;Atypical liposarcoma;High-level tubular adenoma;Case report
INTRODUCTION
Intussusception is common in children but rare in adults[1].It can be classified into four types:Enteric,ileocolic(without appendix invaginates),ileocolic(with ileocecal invagination),and colocolonic(including colorectal type).The etiology of adult intussusception is tumor- or surgery-related,idiopathic,and others.Benign or malignant tumors are the most frequent cause of intussusception in adults[1].Any intestinal condition that changes the normal pattern of peristalsis increases the risk of intussusception[1,2].Normal physiologic peristalsis along a bowel intussusception promotes extension of the invagination to involve longer segments of the intestine,mesentery,and mesenteric blood vessels[1,3].In general,surgery is the best treatment once intussusception is diagnosed.
CASE PRESENTATION
Chief complaints
Abdominal pain accompanied by nausea,vomiting,and hematochezia for 1 d.
History of present illness
The patient was admitted to the emergency department of our hospital due to abdominal pain for 1 d,accompanied by diarrhea,nausea,vomiting,and black stool.The patient had been hospitalized in a local hospital at the early stage of the disease and was diagnosed with“intussusception,colonic mass,and gallbladder stone” by abdominal computed tomography(CT)and colonoscopy.After 1 wk of hospitalization,he was transferred to our hospital for surgical treatment.The patient had normal sleep,poor appetite,poor urination due to prostate stones,poor defecation,and significant weight loss.
考慮到水源工程在運(yùn)行過程中自身需要消耗部分原材料、原水、輔助材料以及備品備件等,建議按陶岔渠首出口新增毛供水量適當(dāng)考慮計(jì)算水源工程的燃料材料及動(dòng)力費(fèi)。
History of past illness
Prostatitis,gallbladder stone,duodenal ulcer.
Physical examination upon admission
Sclera without yellow staining,no bleeding spots or petechiae in the skin mucosa,no liver palm or spider mole were observed.Superficial lymph nodes were not palpated,left epigastrium slightly distended,and no gastrointestinal type and peristaltic wave were noted.Abdomen was soft without tenderness,Murphy's sign was negative,and the liver and spleen were not palpated below the costal margin.The mass,which was approximately 15 cm in diameter,was palpable in the right epigastric region.There was no muscle tension or rebound pain,and no percussion pain in the liver and spleen area,shifting dullness was negative,bowel sound was 3-4 times/min,no air to water sound or high-pitched bowel sound was observed.
Laboratory examinations
White blood cell count was 11.84×109/L,neutrophils 9.86×109/L,red blood cells 5.00×1012/L,hemoglobin 156 g/L,platelets 482×109/L,direct bilirubin 4.5 μmol/L,and total bilirubin 13.2 μmol/L.
Imaging examinations
CT demonstrated an ileocecal bowel tube and mesangial membrane embedded in the ascending colon,showing a concentric circle sign.Eccentric thickening of the tube wall was seen in the colon-liver curvature,and enhancement was noted on the contrast-enhanced scan.The serous surface was slightly rough,herniated into the upper end of the intestinal loop,and there were round fat dense nodules,approximately 2.5 cm in diameter,suggesting a possible fat source of the tumor.Another solid mass,about 4.0 cm in diameter,was seen adjacent to this tumor and was suggestive of colon cancer.At the same time,thickening of the gallbladder wall,multiple dots of high-density shadows in the gallbladder,prostatic hyperplasia,chronic inflammation of the bladder and a small amount of pelvic effusion were noted(Figure 1A and 1B).
We considered the tumor to be the cause of intussusception before surgery;however,as two masses were found,it was uncertain which mass was the main cause of intussusception.We conducted an emergency surgical exploration.During the operation,the small intestine showed obvious dilatation,which is a manifestation of intestinal obstruction.Part of the ileum was inserted into the ascending colon up to the colon-liver curve,approximately 15 cm in length.A right hemicolectomy was performed,and the bowel was cut at the distal end of the tumor on the left side of the transverse colon(Figure 1C).The ileum was cut 15 cm from the ileocecal fold.The right hemicolon and the mesentery were completely removed and isolated.The gallbladder was removed due to gallstones.The ileum was inserted into the cecum up to the hepatic tract of the colon approximately 15 cm in diameter,and the intestinal wall showed necrotic changes.The insertion site showed a tumor in the ileocecum with a clear boundary and a diameter of 2.5 cm.
Postoperative pathology suggested that the ileocecal mass was a fatty dense mass and was suspected to be an atypical liposarcoma/highly differentiated liposarcoma that requiredMDM2gene testing for diagnosis(Figure 2).The transverse colon mass was a high-level tubular adenoma,and the gallbladder showed chronic cholecystitis.Immunohistochemistry results were:CK(-),CDK4(+),MDM2(-),Vimentin(+),s-100(+),CD34(-),SMA(-),beta-catenin(-),Ki-67(5%),CD117(-),and DOG-1(-).To confirm that the ileocecal mass was a lipoma or liposarcoma,the patient underwentMDM2gene testing,and noMDM2gene amplification was reported,which was consistent with the diagnosis of lipoma.The patient was diagnosed with ileocecal lipoma intussusception,transverse colon high-level tubular adenoma,and gallstones.
FINAL DIAGNOSIS
Ileocecal lipoma intussusception,tubular adenoma of the transverse colon,and gallstones.
TREATMENT
Right hemicolectomy and cholecystectomy.
OUTCOME AND FOLLOW-UP
The patient had a good postoperative recovery,without fever or other symptoms,and wound healing was satisfactory without exudation.Postoperative CT examination indicated that the anastomosis was normal.The patient was finally discharged from hospital 16 d after surgery with normal diet,urination,and defecation.
DISCUSSION
Intussusception is defined as a long intestinal tube connected to the stomach or within the lumen,causing diversion of intestinal contents due to intestinal obstruction[4].Intussusception can be divided into primary intussusception and secondary intussusception.More than 90% of primary intussusceptions are found in infants,while secondary intussusception in adult intussusception is clinically characterized by abdominal pain,vomiting,bloody stools,and abdominal mass.The causes of intussusception are diverse,and include ulcerative colitis[5],intestinal amoeba[6],intestinal allergic purpura[7],intestinal polyps[8],Meckel's diverticulum[9],colon cancer[10],colonic lipoma[11],and colonic liposarcoma[12].Intussusception is rare in adult intestinal obstruction[13].In most intussusceptions,there is a starting site of organic lesion from which intussusception develops[14].The types of intussusception are also diverse and include enteric,ileocolic,ileocecal,and colonic[15],and ileocecal intussusception is the most common type[16].
There are also rare causes of intussusception.Jinet al[17]reported cases of intussusception caused by para-duodenal hernia.Chaudharyet al[18]reported a case of colon-colon intussusception caused by primary liposarcoma of the colon.However,it would be interesting to dynamically observe cases of lipoma of the colon from asymptomatic to developing intussusception by colonoscopy[19].

Figure 1 Preoperative computed tomography of tumors and surgical procedure.A:Low density shadow at the distal end of the intussusception can be seen on computed tomography;B:Low-density shadow adjacent to a solid dense mass;C:Lipoma(white arrow)and tubular adenoma(yellow arrow)can be seen next to each other in postoperative specimens.
CONCLUSION
In this case,the patient was admitted to our hospital due to abdominal pain and bloody stool for 1 d.CT showed a low-density tumor and solid dense tumor,which were adjacent to the distal end of the nested bowel.Two masses were also seen on colonoscopy at a local hospital,which caused difficulty in preoperative diagnosis.When the specimens were examined after right hemicolectomy,the adipose-derived neoplasm was found in the nested head.The intussusception continued to the substantial neoplasm,which appeared just before the nested head and played an important role in mechanical blocking of the intussusception.This suggested that the adipose-derived neoplasm was the cause of the intussusception and the substantial neoplasm stopped the advance of the intussusception,and the two masses together caused intestinal obstruction,intussusception and intestinal necrosis.The patient was cured and discharged from hospital after pathological confirmation of the lipoma and high-level tubular adenoma.
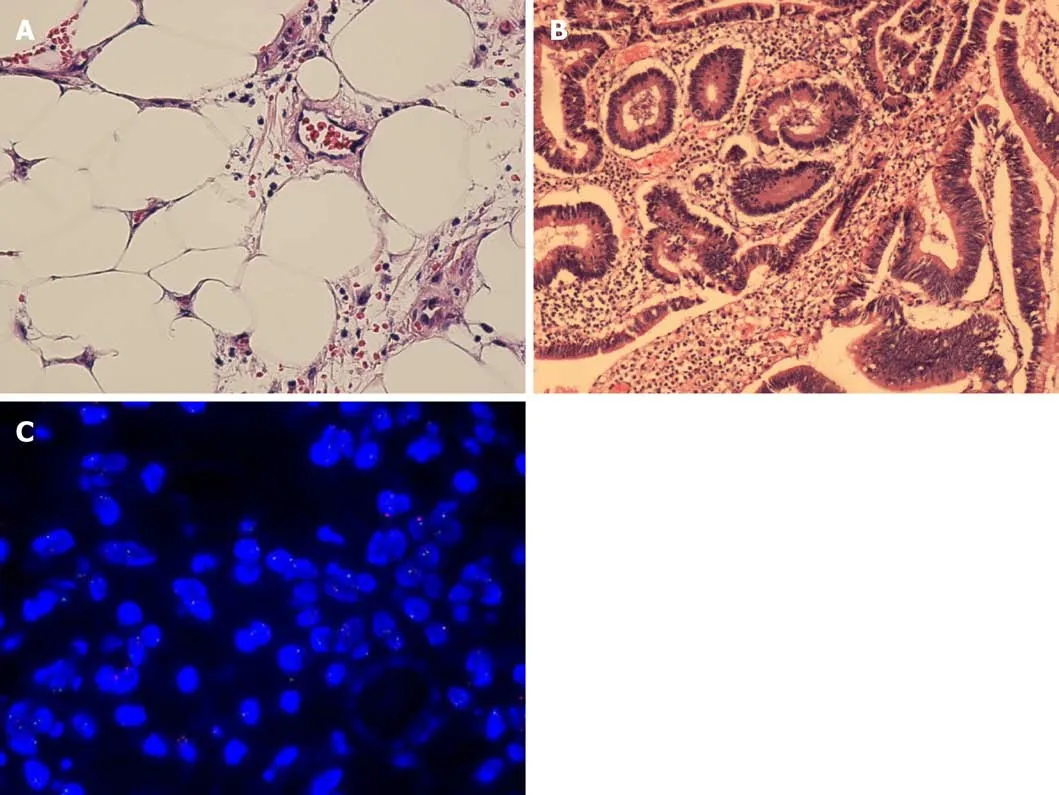
Figure 2 Histopathology of two tumors and fluorescence in situ hybridization result of lipoma.A:The tumor was separated by irregular fibers,and a large number of mature fat cells with hyperchromatin were observed.Adipoblasts were scarce,and mesenchymal nuclear heteroplasmic cells(lipoma)were not observed;B:Adenoid arrangement of tumor cells,cells were columnar,monolayer or multilayer,nuclei were slightly larger,nucleoli were visible,and mitotic images were occasionally seen(tubular adenoma);C:The MDM2 gene amplification signal detected by fluorescence in situ hybridization was negative.
猜你喜歡
工程爆破(2022年3期)2022-07-26 01:58:56
工程爆破(2022年2期)2022-06-17 14:13:56
太空探索(2016年6期)2016-07-10 12:09:06
筑路機(jī)械與施工機(jī)械化(2015年11期)2015-07-01 16:28:43
筑路機(jī)械與施工機(jī)械化(2015年8期)2015-01-11 09:24:54
筑路機(jī)械與施工機(jī)械化(2014年10期)2014-03-01 03:01:59
筑路機(jī)械與施工機(jī)械化(2014年8期)2014-03-01 03:00:52
筑路機(jī)械與施工機(jī)械化(2014年7期)2014-03-01 03:00:16
筑路機(jī)械與施工機(jī)械化(2014年5期)2014-03-01 02:59:07
筑路機(jī)械與施工機(jī)械化(2014年4期)2014-03-01 02:58:34
 World Journal of Clinical Cases2020年10期
World Journal of Clinical Cases2020年10期
- World Journal of Clinical Cases的其它文章
- Needs and concerns of patients in isolation care units - learnings from COVID-19:A reflection
- Successful use of plasma exchange in fulminant lupus myocarditis coexisting with pneumonia:A case report
- Robot-assisted retroperitoneal laparoscopic excision of perirenal vascular tumor:A case report
- Cryptococcal pneumonia in a human immunodeficiency virusnegative patient:A case report
- Treating severe periodontitis with staged load applied implant restoration:A case report
- Rare recurrent gallstone ileus:A case report