64排螺旋CT常規及增強檢查在涎腺占位性病變的診斷和鑒別診斷中的臨床意義
2020-07-14 08:35:29陳巍嵐馬興燦郭作梁
中外醫學研究 2020年14期
陳巍嵐 馬興燦 郭作梁
【摘要】 目的:探討64排螺旋CT常規及增強檢查在涎腺占位性病變的診斷和鑒別診斷中的臨床意義。方法:選取2015年8月-2019年8月筆者所在醫院收治的涎腺腫瘤患者69例。對所有患者行64排螺旋CT常規及增強檢查,對比不同組織的影像學參數。結果:平掃可見涎腺腫瘤病灶均為等密度或低密度影,不同腫瘤間的CT值差異無統計學意義(P>0.05)。進行雙期增強掃描可見,多形性腺瘤動脈期無強化或輕度強化,靜脈期強化程度高于動脈期;腺淋巴瘤呈“快進快出”的強化特征;基底細胞瘤動脈期和靜脈期均有顯著強化;肌上皮瘤動、靜脈期均有輕度強化;黏液表皮樣癌、腮腺細胞癌和涎腺導管癌等惡性腫瘤則為延遲顯著漸進強化特點。在動脈期,腺淋巴瘤的CT值明顯高于其他腫瘤,在靜脈期,則惡性腫瘤的CT值最高,差異均有統計學意義(P<0.05)。結論:在64排螺旋CT的基礎上增強掃描,不同病理分型腫瘤具有各自顯著特征,該技術還能通過機體血流動力學相關指標對涎腺腫瘤的良、惡性加以鑒別診斷,具有一定臨床價值。
【關鍵詞】 64排螺旋CT 增強掃描 涎腺 腫瘤
[Abstract] Objective: To explore the clinical significance of 64 slice spiral CT routine and enhanced scan in the diagnosis and differential diagnosis of salivary gland space occupying lesions. Method: From August 2015 to August 2019, 69 patients with salivary gland tumor were selected. All patients were examined with 64 slice spiral CT routine and enhanced scan, and the imaging parameters of different tissues were compared. Result: On plain scan, the lesions of salivary gland tumors were isodense or hypodense, there was no significant difference in CT value between different tumors (P>0.05). Double phase contrast-enhanced scan showed that pleomorphic adenoma had no or slight enhancement in arterial phase, and the enhancement degree in venous phase was higher than that in arterial phase; adenolymphoma had the characteristics of “fast in and fast out”; basal cell tumor had significant enhancement in arterial phase and venous phase; myoepithelioma had slight enhancement in arterial and venous phase; mucoepidermoid carcinoma, parotid cell carcinoma, salivary duct carcinoma and other malignant tumors were characterized by delayed and progressive enhancement. In arterial phase, the CT value of adenolymphoma was significantly higher than that of other tumors. In venous phase, the CT value of malignant tumors was the highest, the differences were statistically significant (P<0.05). Conclusion: On the basis of 64 slice spiral CT, enhanced scan can show their own significant characteristics of different pathological types of tumors. This technology can also differentiate the benign and malignant salivary gland tumors through the related indexes of hemodynamics, which has a certain clinical value.
涎腺包括腮腺、頜下腺、舌下腺三對大涎腺及散布在口腔黏膜下的許多小涎腺[1]。腫瘤是涎腺組織中最常見的疾病,其中絕大多數是上皮性腫瘤,由于涎腺上皮性腫瘤的病理類型復雜、形態多變,不同類型的腫瘤在臨床表現、影像學表現、治療和預后等方面均不相同[2]。常規的影像學檢查僅可確定病灶的部位、大小、范圍,但在鑒別涎腺腫瘤良、惡性方面易受到檢查者主觀性因素的影響,準確率較低。故探尋一種行之有效的影像學診斷方法具有重要意義[3]。本研究選取2015年8月-2019年8月筆者所在醫院收治的涎腺腫瘤患者69例,以探討64排螺旋CT常規及增強掃描在涎腺占位性病變的診斷和鑒別診斷的臨床意義,現報道如下。
1 資料與方法
1.1 一般資料
選取2015年8月-2019年8月筆者所在醫院收治的涎腺腫瘤患者69例,其中男35例,女34例。年齡19~72歲,平均(43.8±5.3)歲。納入標準:(1)經相關診斷明確符合涎腺腫瘤的標準;(2)未接受腫瘤放化療治療;(3)腫瘤直徑≥10 mm。排除標準:(1)對造影劑過敏;(2)合并重要臟器器質性病變;(3)合并精神類疾病無法配合完成治療。
1.2 方法
64排螺旋CT檢查使用SOMATOM Definition AS+及AW 4.2工作站進行,具體參數為管電壓120 kV,管電流250 mA,DFOV 25 cm,準直32×0.625 mm,矩陣512×512,球管旋轉周期0.4 s。患者取仰臥位,雙管高壓注射器將碘海醇對比劑(300 mg/ml)以4 ml/s注射,掃描延遲5~15 s,總時間50 s。所有患者接受平掃之后,再進行CT雙期增強掃描,掃描前以3 ml/s高壓注射造影劑85 ml,掃描時相動脈期延遲25 s,靜脈期延遲60 s。
所有圖像結果均由筆者所在科2名經驗豐富的影像醫師共同完成。
1.3 統計學處理
使用SPSS 19.0軟件包對本研究數據進行統計學分析。驗證數據正態分布性后,計量資料使用(x±s)表示,多組間進行單因素方差分析。計數資料使用率(%)表示,進行字2檢驗,以α=0.05為檢驗標準。P<0.05為差異有統計學意義。
2 結果
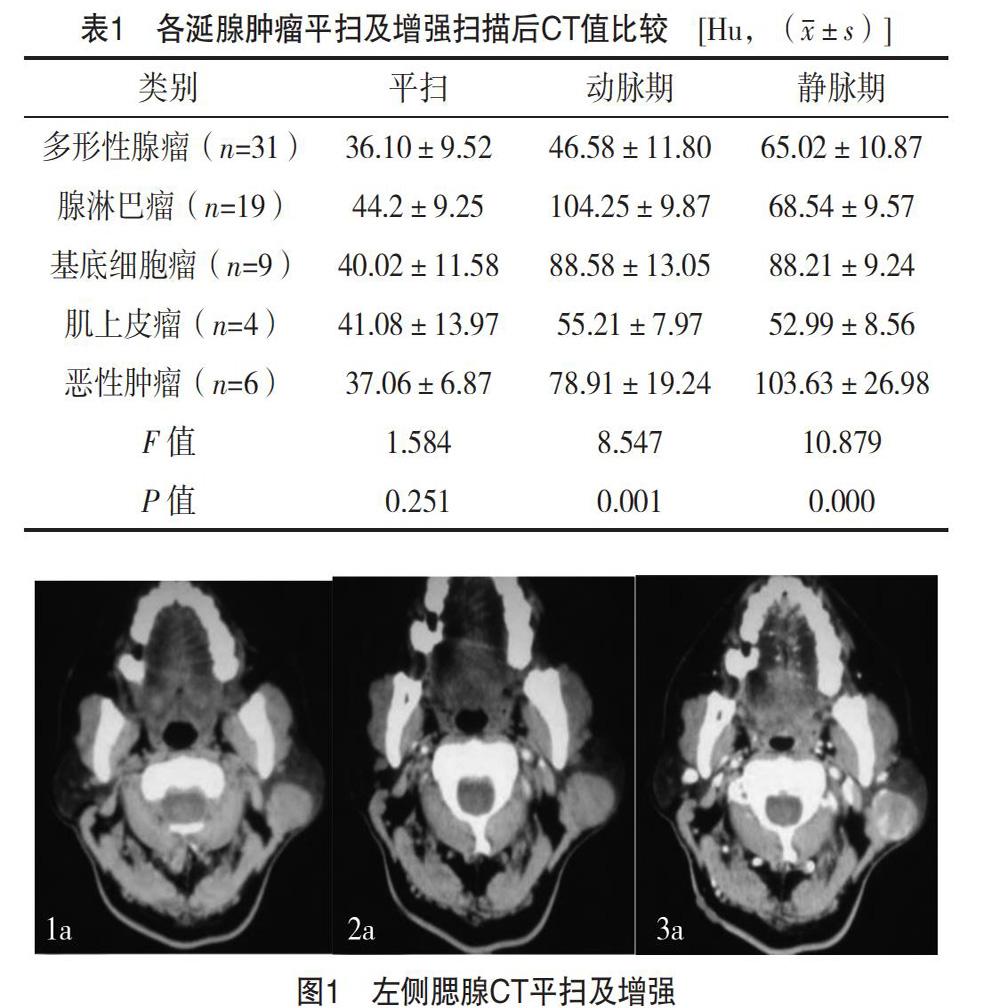
69例患者經病理學檢查,共檢查出涎腺占位性病灶72個,其中多形性腺瘤31例(31個病灶),腺淋巴瘤19例(22個病灶),基底細胞瘤9例(9個病灶),肌上皮瘤4例(4個病灶),黏液表皮樣癌3例(3個病灶),腮腺細胞癌1例(1個病灶),涎腺導管癌2例(2個病灶)。平掃可見上述病灶均為等密度或較低密度影,但不同病理分型腫瘤間的CT值差異無統計學意義(P>0.05),見表1。
進行雙期增強掃描可見,多形性腺瘤動脈期無強化或僅有輕度強化,靜脈期強化程度高于動脈期;腺淋巴瘤呈“快進快出”的強化特征;基底細胞瘤動脈期和靜脈期均有顯著強化;肌上皮瘤動、靜脈期均有輕度強化;黏液表皮樣癌、腮腺細胞癌和涎腺導管癌等惡性腫瘤則為延遲顯著漸進強化特點。在動脈期,腺淋巴瘤的CT值明顯高于其他腫瘤,在靜脈期,則惡性腫瘤的CT值最高,差異均有統計學意義(P<0.05),見表1。影像學檢查見圖1,男,42歲,多形性腺瘤患者。
3 討論
正常涎腺組織因其豐富的脂肪組織含量,在影像學CT平掃檢查時圖像密度與周圍的肌肉組織能形成較清晰的天然對比,因此,絕大部分涎腺腫瘤能通過CT平掃進行清晰顯示,有學者研究認為,平掃檢查對涎腺腫瘤的定位率高達100%[4]。但對于不同病理分型的涎腺腫瘤,其在CT平掃時均變現為等密度或低密度影,難以通過CT值差異對其進行辨別診斷。盡管目前良性涎腺腫瘤多位于淺葉,邊界規整清晰,惡性涎腺腫瘤多膨脹于深葉,并向周圍組織侵犯這一理論已得到廣泛認可[5],但統計學分析卻顯示,良、惡性涎腺腫瘤在形態和邊界上的差異并無意義[6]。故使用CT平掃對涎腺腫瘤進行定性、定量診斷會有較大的局限性[7]。在本研究中,選取筆者所在醫院收治的69例涎腺占位性病變患者進行回顧性分析,發現患者接受CT平掃和雙期增強掃描后,不同病理分型涎腺腫瘤的強化方式與強化程度不一,能夠為該類患者的定性診斷提供理論依據。
筆者將本研究中不同類型涎腺腫瘤接受CT平掃和雙期增強掃描后的影像學特診表述如下:(1)多形性腺瘤,該類腫瘤又被稱為混合瘤,好發于腮腺淺葉,腫瘤直徑以3 cm以下居多,CT平掃時病灶為等密度或低密度影,并可能出現囊變,增強掃描可見動脈期病灶無強化或僅輕度強化,靜脈期病灶強化程度較動脈期明顯,可為輕度或中度強化[8]。(2)腺淋巴瘤,該類腫瘤好發于腮腺淺葉后下極及尾部,筆者推測這與腮腺淋巴結組織的分布有關。病灶以多發性為常見,患者可為單側性多發或雙側受累。腫瘤直徑同樣以3 cm以下居多,CT平掃時病灶為等密度影,約1/4出現囊變[9],增強掃描可見動脈期病灶有顯著強化,推測這與腫瘤實質中豐富的毛細血管含量及毛細血管擴張密切相關,靜脈期病灶則為輕度強化,總體呈“快進快出”的強化特征[10]。(3)基底細胞瘤,病灶常邊界清晰,好發于腮腺淺葉,CT平掃呈等密度影,4/5出現較大囊變[11],增強掃描可見病灶在動脈期和靜脈期均呈顯著強化,這與腫瘤實質內豐富的毛細血管和小靜脈有關,總體呈“早期顯著持續強化”特征[12]。(4)肌上皮瘤多位于腮腺淺葉,邊界清晰,CT平掃示病灶為等密度影,有部分病理出現小囊變,增強掃描示動脈期和靜脈期均有輕度強化[13]。(5)惡性腫瘤包括黏液表皮樣癌、腮腺細胞癌、涎腺導管癌等,腫瘤大小為2~5 cm,CT平掃病灶密度不均,邊界不清晰,有侵犯周圍組織或區域淋巴結轉移的特點[14],腫瘤實質內有不同程度的壞死或囊變,增強掃描體上為“延遲顯著強化持續”的特點[15]。
綜上所述,在64排螺旋CT的基礎上增強掃描,不同病理分型腫瘤具有各自顯著特征,該技術還能通過機體血流動力學相關指標對涎腺腫瘤的良、惡性加以鑒別診斷,局有一定臨床價值。
參考文獻
[1] Benjamin A F,Colin C E,John R,et al.Effect of rituximab on a salivary gland ultrasound score in primary Sj?grens syndrome: results of the TRACTISS randomised double-blind multicentre substudy[J].Annals of the Rheumatic Diseases,2018,77(3):412-418.
[2] Yue D,Feng W,Ning C,et al.Myoepithelial carcinoma of the salivary gland: pathologic and CT imaging characteristics (report of 10 cases and literature review)[J].Oral Surgery,Oral Medicine,Oral Pathology and Oral Radiology,2017,123(6):e182-e187.
[3] Thomas J Vogl,Moritz H Albrecht,Nour-El-din A Nour-Eldin,et al.
Assessment of salivary gland tumors using MRI and CT: impact of experience on diagnostic accuracy[J].La Radiologia Medica,2017,123(2):1-12.
[4] Cheng-En Hsieh,Nai-Ming Cheng,Wen-Chi Chou,et al.Pretreatment primary tumor and nodal SUVmax values on 18F-FDG PET/CT images predict prognosis in patients with salivary gland carcinoma[J].Clinical Nuclear Medicine,2018,43(12):1.
[5] Cheng-En Hsieh,Kung-Chu Ho,Chia-Hsun Hsieh,et al.Pretreatment primary tumor SUVmax on 18F-FDG PET/CT images predicts outcomes in patients with salivary gland carcinoma treated with definitive intensity-modulated radiation therapy[J].Clinical Nuclear Medicine,2017,42(9):655.
[6] Vidiri Antonello,Curione Davide,Piludu Francesca,et al.Non-squamous tumors of the oropharynx and oral cavity:CT and MR imaging findings with clinical-pathologic correlation[J].Current Medical Imaging Reviews,2017,13(2):166-175.
[7] Zou H,Shen Y,You J,et al.Salivary gland scintigraphy in diagnosis of Sj?grens syndrome[J].Chinese Journal of Medical Imaging Technology,2017,33(3):399-403.
[8] Ugga L,Ravanelli M,Pallottino A A,et al.Diagnostic work-up in obstructive and inflammatory salivary gland disorders[J].Acta Otorhinolaryngol Ital,2017,37(2):83-93.
[9] Martin H Cherk,Grace Kong,Rodney J Hicks,et al.Changes in biodistribution on 68Ga-DOTA-Octreotate PET/CT after long acting somatostatin analogue therapy in neuroendocrine tumour patients may result in pseudoprogression[J].Cancer Imaging,2018,18(1):3.
[10] Svitlana Veniaminivna Kolomiiets,Kristina Oleksandrivna Udaltsova,Tetiana Andriivna Khmil,et al.Difficulties in diagnosis of sialolithiasis: a case series[J].Bulletin of Tokyo Dental College,2018,59(1):53-58.
[11] Yasuhiro Nakashima,Riichiro Morita,Akiko Ui,et al.Epithelial-myoepithelial carcinoma of the lung:a case report[J].Surgical Case Reports,2018,4(1):74.
[12] Pingzhong Wang,Jie Yang,Qiang Yu.Lymphoepithelial carcinoma of salivary glands:CT and MR imaging findings[J].Dentomaxillofac Radiol,2017,46(8):20170053.
[13] Yeun J Kim,Hyun S Hong,Sun H Jeong,et al.Lymphoepithelial carcinoma of the salivary glands[J].Medicine,2017,96(7):e6115.
[14] Capaccio P,Canzi P,Gaffuri M,et al.Modern management of paediatric obstructive salivary disorders:long-term clinical experience[J].Acta Otorhinolaryngol Ital,2017,37(2):160-167.
[15] Camelia Liana Buha?,Elena Ro?ca,Gabriela Mu?iu,et al.Acinic cell carcinoma of minor salivary glands-case report[J].Rom J Morphol Embryol,2017,58(3):1003-1007.
(收稿日期:2020-01-18) (本文編輯:何玉勤)
